A Century of Vaccination and What it Teaches.
a book by
W. Scott
Tebb, M.A., M.D. (Cantab.), D.P.H.
London: Swan Sonnenschein & Co, 1898
[Note: the chapter subheadings listed below are page headings in the original book, so don't sometimes correspond exactly to the text as a chapter sub-heading would do. Some have been moved slightly to aid in navigation.]
PREFACE.
CHAPTER 1.
A brief account of the Early History of Vaccination, showing how it was accepted by
the Profession on inadequate evidence
METHODS
OF SMALL-POX INOCULATION.
JENNERS VARIOLOUS TESTS.
THE VALUE OF JENNER'S TESTS.
WOODVILLE AND PEARSON.
"VACCINATION" WITH VARIOLOUS LYMPH.
LANGWORTHY AND ARSCOTT'S
EXPERIMENTS.
OPINION OF THE
ROYAL COMMISSION.
SPURIOUS COWPOX
CONDEMNED BY THE
COLLEGE OF PHYSICIANS.
CHAPTER 2. The Decline
in Small-pox since the Introduction of Vaccination
THE VACCINATION
ACTS.
SMALL-POX AND
VACCINATION SINCE 1872.
DECLINE OF TYPHUS FEVER.
CAUSE OF DECLINE OF
FEVERS.
AGE-INCIDENCE OF
SMALL-POX.
INCREASE IN ADULT MORTALITY
OF SMALLPOX
AGE-INCIDENCE
OF TYPHUS FEVER.
AGE-INCIDENCE OF
INFLUENZA.
AGE-INCIDENCE OF
SMALL-POX.
POCK-MARKED FACES.
CHAPTER 3. Some of the Causes of the
Decline in the Small-pox Mortality
SMALL-POX DIFFUSED
BY INOCULATION.
SALUTARY EFFECT OF
OPEN SPACES.
INCREASE OF
METROPOLITAN AIR-SPACES.
THE WINDOW-TAX
DOMESTIC INSANITARY
CONDITIONS.
EIGHTEENTH CENTURY PRISONS.
AGE-INCIDENCE AND
SANITATION.
BURIAL GROUNDS AND
MORTALITY.
COMMERCIAL DEPRESSION.
THE EFFECTS OF WAR.
MALTHUS
DISCOVERS A NEW PRINCIPLE.
THE ZYMOTIC DISEASES REPLACE EACH OTHER.
CHAPTER 4. The Incidence of
Small-pox on Vaccinated and Unvaccinated Communities.
CHAPTER 5. Does Vaccination Prevent Small-pox ?
CHAPTER 6. The
Mitigation Theory
CHAPTER 7.
Re-vaccination
CHAPTER 8. Influence of Sanitary Measures on the Incidence
and Mortality of Small-pox
CHAPTER 9. The Injurious Results of Vaccination
CHAPTER 10. Summary
and Conclusions
Diagram and Appendix
So long as the practice of vaccination remains established and enforced by law, it will be the duty of every citizen, who is also the father of a family, to form a judgment upon it; unless, indeed, it is to be held that the infallibility of the legislature and of the medical profession, which in this instance directed legislation, is so well assured that enquiry is superfluous, if not culpable. But it is a sounder doctrine that the existence of the law does not relieve parents of responsibility towards their children, and more especially parents (nowadays the majority) who have heard that the efficacy of this operation has been called in question by competent men, while its risks, so long denied, are now on all hands admitted. I am, therefore, not without hopes that among my readers will be included a fair number of the general public" interested in the subject by the pressure of compulsion, and anxious before they submit a child to vaccination to feel assured that they are doing the right thing, being also resolved to withhold the child from the operation if they cannot be satisfied of this.
But I here address myself more particularly to two classes—to my medical brethren, and to those whose business it is to legislate for the country on this subject. On the former I desire, with all respect, to urge the following considerations:—
Can it be said that the Jennerian doctrine of vaccination has ever been placed on a truly scientific basis? I specify the "Jennerian doctrine," for there are other aspects of the vaccination or inoculation theory, which I expressly rule out of my enquiry. It is a generally received opinion that in the case of certain diseases one attack affords some degree of immunity against a second. It is certain that there are exceptions to the rule, and it is further certain that the rule has never been scientifically established as such. Nevertheless, it is a generally accepted belief, with evidence in its favour, and in the pages that follow I do not reject or even attack that belief. Further, it is a postulate of the modern inoculation doctrine that a mild or modified attack suffices to secure this immunity. Whether this be so or not, I cannot tell. It is a matter into which I have not been led to enquire, and I am willing to grant it for the sake of argument, since it does not really concern the position which I am calling in question. What I do deny, as the result of my enquiries, is that an attack of cow-pox secures immunity against small-pox. To use technical terms in order to make the distinction clear: while I may allow within limits the truth of homoprophylaxy or homoeoprophylaxy, I am satisfied that there has never been shown any sort of scientific basis for heteroprophylaxy. If the reply be made that, granting it is wrong to teach that vaccination is homoprophylactic, it is fair to claim for it that it is homoeoprophylactic, I should deny that such a claim can be sustained ; and, though I am, of course, aware that variolous matter can be so modified by being taken at an early stage and passed once or twice through the calf as to produce, when inoculated, not an attack of small-pox, but local effects similar in appearance to those of vaccination, yet that is not what is done every day by medical men who vaccinate. What they are doing they really do not know, nor does any one know, for the ultimate origin of the vaccine lymph in common use has long ago been lost sight of; but if it be true that that ultimate origin is cow-pox, if, that is to say, when we vaccinate we are carrying out the teaching of Jenner, then, certainly, we are acting as if heteroprophylaxy had been established scientifically; for the investigations of Dr. Creighton and Professor Crookshank have proved conclusively that cow-pox is a disease radically different from that against which it is said to protect. Effects similar to those of vaccination can be produced in a variety of ways, and, therefore, to produce them as Dr. Klein and others claim to have done, by means of small-pox virus, attenuated or in other ways concocted, does not identify the disease on which Jenner relied for protection with the disease against which he claimed that it protected, any more than does the production of a vaccine vesicle from cattle-plague identify vaccination with that disease.
Many of my brethren, while willing to acknowledge that there is no true pathological relation between cow-pox and small-pox, fall back on the alleged evidence of statistics, and claim to find in them a scientific vindication of vaccination. The majority of the Royal Commissioners took this view, and rather deprecated the idea that any other scientific vindication was necessary. To the questioning of the position that trustworthy statistics do provide such a vindication my pages are partly devoted. I do not deny that the "century of vaccination" synchronises roughly with a century in which small-pox (in Europe, at any rate) has largely declined. But this coincidence by no means involves any connection in the way of cause and effect. Small-pox, like typhus, has been dying out since 1780. Vaccination in this country has fallen largely into disuse since people began to realise how its value was discredited by the great smallpox epidemic of 1871-72. So that, while small-pox has declined during the last one hundred and twenty years, twenty years may be cut off from each end of this period, as contributing no evidence whatever of the decline being due to vaccination, and as involving the conclusion that some other causes have been at work to promote this result. I am, of course, only speaking approximately. To the evidence afforded by detailed cases criticism of another kind is applicable, and to this I will presently refer. But, first, in passing, I would call attention to the ease with which an alleged protective operation can acquire a great reputation as successful, more especially if its adoption should coincide with a decline from other causes of the disease against which it is supposed to protect. A local epidemic of small-pox is seldom so severe as to attack more than 5 per cent. of the population. If, therefore, a small minority has adopted some alleged prophylactic, it is very unlikely that the disease will count among its victims any considerable proportion of those who are thus fortified, particularly as they would be likely to be more than ordinarily careful in matters relating to health. In this way their prophylactic will acquire a great reputation, and the vastly greater number who have equally escaped without having recourse to the protective operation will be overlooked. This is what happens in pretty nearly every epidemic in regard to re-vaccination and the security it is alleged to provide. In the case of primary vaccination other but not less misleading inferences are drawn. Should there be an epidemic of small-pox in a locality where 85 per cent, of the population are vaccinated, it is obvious that the 95 per cent. of the population who escape the epidemic (assuming, as before indicated, a maximum of 5 per cent, attacked by it) will largely coincide with the 85 per cent, vaccinated ; and vaccination thus gains credit. But it will be objected, if the 5 per cent, attacked coincide, in however small a degree, with the 15 per cent, unvaccinated, this is strong testimony to the risk of being unvaccinated ; and so, no doubt, it would be, but for the fact that in localities where the vaccination law is vigorously carried out, the unvaccinated, as a class, will be found to consist largely of the outcasts of society, nomads whom the law has failed to reach, and of weakly children who on account of their health have been excused the operation. This class, therefore, is likely to furnish a disproportionate number of the victims of the epidemic ; and thus again the prophylactic acquires reputation. Add to this the facts, often overlooked, that medical men, even if officials and highly placed, are still liable as men to err, and that their errors will probably accord with their cherished beliefs, and it will readily be understood that the evidence of detailed cases—which is really the only evidence on which the credit of vaccination depends—cannot be accepted wholesale as if it were not open to question. A vaccinated patient with no visible signs of vaccination is likely to be described as unvaccinated if his case is severe, and especially if death ensues ; while if the marks are not plainly visible, the explanation of "not properly performed" is an obvious one ; and the patient will be included as "belonging to the unvaccinated or imperfectly vaccinated class" in the list of cases, and, tout court, as "unvaccinated " or "having no marks" in the official summary. I think it would be advisable for my medical brethren to accept as authentic only published and tested cases, or such as have come under their own personal observation.
To those who are about to legislate for the country on this vexed question I also address myself particularly. The Queen, in her Speech at the opening of the present Session of Parliament, called for "earnest consideration" of the subject. Hitherto vaccination bills have been passed into law without adequate discussion or debate. Parliament has been assured (incorrectly) that there is complete unanimity in the medical profession concerning the nature, value, necessity, and safety of vaccination ; and that has sufficed. Lords and Commons have at once bowed before this alleged unanimity, with the result, as vaccinists claim, but cannot possibly prove, that small-pox has been practically stamped out, but undoubtedly also with the result that hundreds of infants have died from the effects of the operation, that thousands of otherwise blameless citizens have been lined or imprisoned for their very natural and proper resistance to this extraordinary law, and hundreds of thousands of pounds of public money have been spent on what I am satisfied is nothing but a useless and mischievous fallacy. It is strange that members of Parliament do not perceive that the strength of the pro-vaccinist party lies in the public endowment of the practice. Right through the century there has existed a body of officials, ostensibly paid to promote the practice of vaccination, but also, partly at least, paid to vindicate it theoretically, and to explain away its failures and its accompanying disasters. But for this State aid, vaccination would long ago have been consigned to the same limbo as has received a thousand other similar fads which, fortunately for the public, have not secured official recognition and support. I hardly expect that legislators will have time to read the numerous cases I adduce—some showing that immunity from small-pox exists without vaccination, others that mild attacks of small-pox were recorded long before there was any alleged mitigating power in vaccination to which to ascribe them, and, again, others proving that neither vaccination nor re-vaccination nor recent vaccination can be depended upon to protect from small-pox or even from death from that disease. But to the cases of injury and death resulting from vaccination I trust they will not refuse to give some attention. This evidence should be enough to determine any fair-minded enquirer that the enforcement of vaccination by law is indefensible. Take away first the compulsory law, and then take away (if vested interest is not too strong for you) the endowment of the practice, and, when this has been effected, medical men will find themselves for the first time since 1803 free to discuss the vaccination question as a scientific one on its own merits. To what result that unfettered discussion will lead I have myself (now that I have studied the matter carefully for some years) no sort of doubt.
In conclusion, I desire to express my obligations for the valuable assistance of Mr. A. W. Hutton, whose letters on "The Vaccination Question," addressed to Mr. Asquith and Mr. Balfour in 1894 and 1895, I can recommend as an introduction to the rational study of this vexed problem.
CHAPTER 1.
A BRIEF ACCOUNT OF THE EARLY HISTORY OF VACCINATION, SHOWING HOW IT WAS
ACCEPTED BY THE PROFESSION ON INADEQUATE EVIDENCE.
Dr. JENNER, in one of his later papers, "The Origin of The Vaccine Inoculation," informs us that his inquiry into the nature of cow-pox commenced shortly before the year 1776. There is, however, an incident alluded to by Baron,1 his biographer, which would seem to show that his attention was drawn to the subject during his apprenticeship, which lasted from 1762 to 1768. A young countrywoman came to seek advice; the subject of small-pox was mentioned in her presence; she immediately observed, "I cannot take that disease, for I have had cow-pox." This, we are told, riveted the attention of Jenner. Whether this was so or not, he apparently did not follow it up till the year 1788, when he repeated the tradition of the dairymaids in London, taking with him a drawing of the cow-pox eruption on the hand of a milker.
1. Baron's "Life of Jenner," vol. i., pp. 121, 122.
About the year 1791 Jenner appears to have seriously commenced to collect notes of cases of cow-poxed milkers who were said to have resisted smallpox inoculation. His first paper, which was shown to the Council of the Royal Society in 1797, and afterwards returned to him,1 gives ten such instances. In order to examine somewhat closely this claim—that those who had taken cow-pox were secure against the artificial introduction of small-pox—it is necessary to give a short account of small-pox inoculation as it was practised in the last century.
This practice, the forerunner of vaccination, was first brought to English notice by a letter from Dr. Timoni, a Greek physician practising in Constantinople; the letter was addressed to Dr. Woodward, Gresham Professor of Physic, who had it printed in the "Philosophical Transactions" for 1714. The credit of the introduction of the practice into this country is, however, due to Lady Mary Wortley Montague. Mr. Wortley Montague was appointed Ambassador to the Porte in 1716, and not long after their arrival his wife wrote to a friend about the invention of ingrafting. "Every year," Lady Montague says, "thousands undergo this operation; and the French Ambassador says pleasantly that they take the small-pox here by way of diversion, as they take the waters in other countries." Shortly afterwards, her son, aged five, was submitted to the operation, which was performed by a Greek woman under the supervision of Mr. Charles Maitland, Surgeon to the Embassy. In 1721, Lady Mary, who had returned to London, had
1 Letter from Jenner to Moore. Baron's "Life of Jenner," vol. ii., p. 364.
METHODS OF SMALL-POX INOCULATION.
her daughter inoculated by Maitland. In the same year this surgeon experimented on some condemned criminals at Newgate, and in 1722 variolation was encouraged by Royalty.
Another of the early inoculators was Thomas Nettleton, of Halifax, who recommended long and deep incisions, and the using of matter from ripe pustules. The severity of the disease induced was a great bar to the progress of small-pox inoculation, and by the year 1728 the practice had almost ceased. It was revived about 1740, and in 1754 was authoritatively sanctioned by the Royal College of Physicians, who pronounced it to be "highly salutary to the human race." About the year 1703 a milder method of procedure came into vogue; this was first introduced by Gatti, the French inoculator, and was taken up in this country by Daniel Sutton and Dr. Dimsdale, the latter of whom has published accounts of his practice. Dimsdale says :—
"It seems not improper to add, that the method I now generally use in performing the inoculation, as believing it to be the best, is simply this : The point of a lancet slightly dipped in the recent variolous matter, which I prefer taking during the eruptive fever, is introduced obliquely between the cuticula and the cutis, so as to make the smallest puncture possible, rarely producing a drop of blood." 1
1. "Tracts on Inoculation," p. 130. Hon. Baron T. Dimsdale. London. 1781.
Dimsdale preferred inoculating from mild cases and from arm to arm, for he says :—
" If neither an inoculated patient is at hand, nor anyone in the neighbourhood has a distinct kind of the natural disease, a thread may be used as in the common manner, provided the thread be very recently infected." 1
About the results he adds :—
" In general, the complaints in this state are very moderate, and attended with so little illness that the patient eats and sleeps well the whole time : a few pustules appear, sometimes equally dispersed."2
He also had some very mild cases which not only had little or no pustular eruption on the body or fever, but did not even present a pustule at the seat of inoculation, there being simply local inflammation; and in his book he gives a list of twelve such cases, which, however, he considered protected from any future attack of small-pox.
Another writer, Dr. Giles Watts, in referring to this new method of inoculation, says :—
"To say the truth, it is a fact well known to inoculators, in this way, and I have sometimes known the same happen in the old, that the patients pretty often pass through the smallpox so easily as to have no more than five pustules. Nay, it happens every now and then, in this way of inoculation, that even an adult patient shall pass through the distemper without having one, or even so much as a single complaint, other than, perhaps, a slight shivering, chill, or some such trifling disorder, which he would hardly have taken the least notice of at any other time." 3
1. ''The Present Method of Inoculating for the Small-pox," p. 29. Thomas Dimsdale, M.D. London. 1767.
2. Ibid., p. 37.
3. "A Vindication of the New Method of Inoculating the Small-pox," p. 10. Giles Watts, M.D. London. 1767.
Thus the inoculation-system of Sutton and Dimsdale, which produced such mild
results, depended upon getting matter from the eruption of small-pox at an
early
JENNERS
VARIOLOUS TESTS.
stage of the disease, using it when fresh, inoculating from mild cases or from arm to arm, taking the smallest quantity of matter and introducing it by a superficial puncture. This, it may be noted, is precisely the sort of inoculation Jenner recommended should be used in applying the variolous test in cases which had been vaccinated. Jenner says :—
" In some of the preceding cases I have noticed the attention that was paid to the state of the variolous matter previous to the experiment of inserting it into the arms of those who had gone through the cow-pox. This I conceived to be of great importance in conducting these experiments."1
Now, if we refer to the case of John Phillips, aged sixty-two, who had had the cow-pox at the age of nine years, we learn that the matter for inoculation was taken from the arm of a boy just before the commencement of the eruptive fever, and instantly inserted. A little further on he relates a story of a medical man who used stale small-pox lymph for inoculation, with serious results. Then he continues :—
"As a further cautionary hint, I shall again digress so far as to add another observation on the subject of inoculation. Whether it be yet ascertained by experiment that the quantity of variolous matter inserted into the skin makes any difference with respect to the subsequent mildness or violence of the disease, I know not; but I have the strongest reason for supposing that, if either the punctures or incisions be made so deep as to go through it, and wound the adipose membrane, that the risk of bringing on a violent disease is greatly increased."
1 "An Inquiry into the Causes and Effects of the Variolś Vaccinś." Jenner. London. 1798.
With regard to these ten cases of casual cow-pox in milkers who had been subsequently inoculated with small-pox, the method of inoculation then in vogue was probably used ; therefore, from the conditions under which the test was made, on Jenner's own showing, a slight and trivial result was the most that should have been anticipated. Jenner, however, admits a certain amount of local inflammation supervening in all the cases he describes, which, if we make allowance for the general looseness and ambiguity of his statements, may, not inconceivably, include the appearance of a local pustule at the seat of inoculation.
In 1796 Jenner vaccinated his first case, James Phipps. In less than seven weeks from the insertion of the cow-pox matter Phipps was inoculated with small-pox, with the result that "the same appearances were observable on the arms as we commonly see when a patient has had variolous matter applied, after having either the cow-pox or the small-pox."
Now, the question is, What appearances did Phipps actually have on his arms as the result of the variolous test ? And to guide us in forming an opinion, there is a letter of Jenner's to a medical man, Mr. John Shorter, who wrote to him about two cases in which he had applied the test six months after successful vaccination, with the result of producing a pustule at the seat of inoculation in each case. Jenner, in his reply, December 29, 1799, says :—
" Pray, recollect how seldom we find the skin insensible to the action of variolous matter in those who have previously gone through the small-pox. The cow-pox leaves it in the same state. The patients you mention were not insensible to the local action of the variolous virus." 1
THE VALUE OF JENNER'S TESTS.
Thus, if the skin is seldom insensible to variolous matter after cow-pox or small-pox, and these cases of Shorter's are samples of the result, it seems not improbable that when Jenner applied the variolous test in the case of Phipps he got a local pustule at the seat of inoculation ; for the same appearances, he says, were produced as commonly observed when variolous matter was applied to a person who had had cither cow-pox or small-pox.
Mary James2 is another of the few cases Jenner is known to have subjected to the variolous test. This was applied eight months after vaccination, with the result of a local pustule, fever, and the faint appearance of a rash about the wrists; matter taken from the arm of this case produced small-pox when inoculated on her brother.
To sum up the value of these tests. It amounts to this: that Jenner, in applying them, used a form of inoculation which produced little more than a local result, and the appearances he obtained were not very different from what would be produced by that form of inoculation when there was no question of cow-pox at all.
Apparently the test broke down, not only in the case of Mary James, but in other instances. Mr. Thornton,3 surgeon, of Stroud, published his experience. The cases are important as being the first independent evidence after the publication of Jenner's "Inquiry." He vaccinated a Mr. Stanton and four of his children
1. Medical and Physical Journal, vol. iii., p. 351. (April, 1800.)
2. ''Further Observations on the Variolś Vaccinś , or Cow-pox." Jenner. 1799.
3. Letter dated February 7, 1799, and published in Dr. Beddoes' "Contributions to Physical and Medical Knowledge," p. 398.
from a milker on the Stonehouse Farm, a source used by Jenner himself. The matter was taken from a purulent pock, the only one which was not degenerated into a sordid and painful ulcer. In the four children the inflammation was severe and protracted, the scabs falling off about the twentieth day. "From the long continued local excitement," Mr. Thornton adds, " I began to entertain a hope that the virus might imperceptibly have crept into the habit, and proved a security against the variolous infection." So, to relieve his own doubts, and to ensure the safety of the patients, he inoculated them with smallpox, with the result that "all the children received the infection, and passed through the different stages of the disease in the usual slight manner." Mr. Stanton, in whom the inflammation had not been so severe, was the only one who resisted the variolous inoculation.
At the end of 1798, six months after the publication of Jenner's "Inquiry," the case for vaccination stood thus : Most of the children's arms had ulcerated, and the variolous test, in the few cases in which it had been applied, had produced equivocal results. Moreover, all Jenner's stocks of lymph had been lost, so that no further experiments could be made. Dr. Beddoes, of Bristol, in writing to Professor Hufeland, of Berlin, said :—
"You know Dr. Jenner's experiments with the cow-pox. His idea of the origin of the virus appears to be quite indemonstrable, and the facts which I have collected are not favourable to his opinion that the cow-pox gives complete immunity from the natural infection of smallpox. Moreover, the cow-pox matter produces foul ulcers, and in that respect is a worse disease than the mildly inoculated small-pox."
The celebrated Dr. George Gregory, Physician to the London Small-pox Hospital, in his lectures at St. Thomas's Hospital, has alluded to the inconclusiveness of Jenner's thesis. "When we were engaged in tracing the early history of vaccination, you must have been struck with the extraordinary contrast between the absolute scepticism concerning the prophylactic virtue of cow-pox which prevailed before the publication of Jenner's first essay and the unlimited confidence reposed in it, within two years afterwards, in all parts of the world. A calm and dispassionate examination of Jenner's first essay is calculated to awaken some surprise at this sudden conversion of men's minds." 1
1 " Lectures on the Eruptive Fevers," p. 207. London. 1843.
It can thus be quite understood that the profession required more satisfactory proof before accepting the new doctrine; and they shortly afterwards obtained evidence which to them appeared to support Jenner's theories.
On January 20, 1799, Dr. William Woodville, Physician to the London Small-pox Hospital, received intelligence of an outbreak of cow-pox among the cows at a dairy in Gray's Inn Lane. The disease on a milker's hand was compared with Jenner's plates and pronounced genuine. It was then decided to give it a trial; and the experiments were conducted by Drs. Woodville and Pearson at the Small-pox Hospital. The first inoculations were made from the cow and from the hand of a dairymaid, and the subsequent ones, to the number of five hundred, from arm to arm. With regard to the testing of the cases by small-pox inoculation, Dr. Woodville says :—
" Of all the patients whom I inoculated with variolous matter, after they had passed through the cow-pox, amounting to upwards of four hundred, none were affected with the small-pox."1
Concerning these tests M'Ghie says :—
" Suffice it to observe, that the trials which were made by the profession, to communicate variola to those whom they had vaccinated, completely failed. The cow-pox having thus triumphantly undergone the experimentum crucis, vaccination was soon eagerly adopted by the unprejudiced and disinterested in every country to which the vaccine lymph was conveyed." 2
If we analyse these so-called vaccinations, we find that three-fifths of the patients had pustules about the body—and it is no longer disputed that these pustular cases were cases of small-pox—and hence the subsequent variolous tests were of no value in settling the question of the protective value of cow-pox. Let us now consider the remaining two-fifths, which only presented a local pustule at the seat of inoculation; and to do this it is important to discuss the means by which Woodville's cases became contaminated. As the Vaccination Commissioners3 have pointed out, small-pox may have been introduced—
(1) By infection at the Hospital or at the patients'
homes.
(2) By the inoculation of small-pox; several patients
being purposely inoculated with small-pox a few days after " vaccination."
(3) The lymph with which the patients were " vaccinated" may have become contaminated with small-pox.
1. Reports of a Series of Inoculations for the Variolś Vaccinś, on cow-pox. William Woodville, M.D. London. 1799.
2. "Thoughts on Vaccination," p. 11. Dumfries. 1827.
3. Final Report, Royal Commission on Vaccination, p. 147.
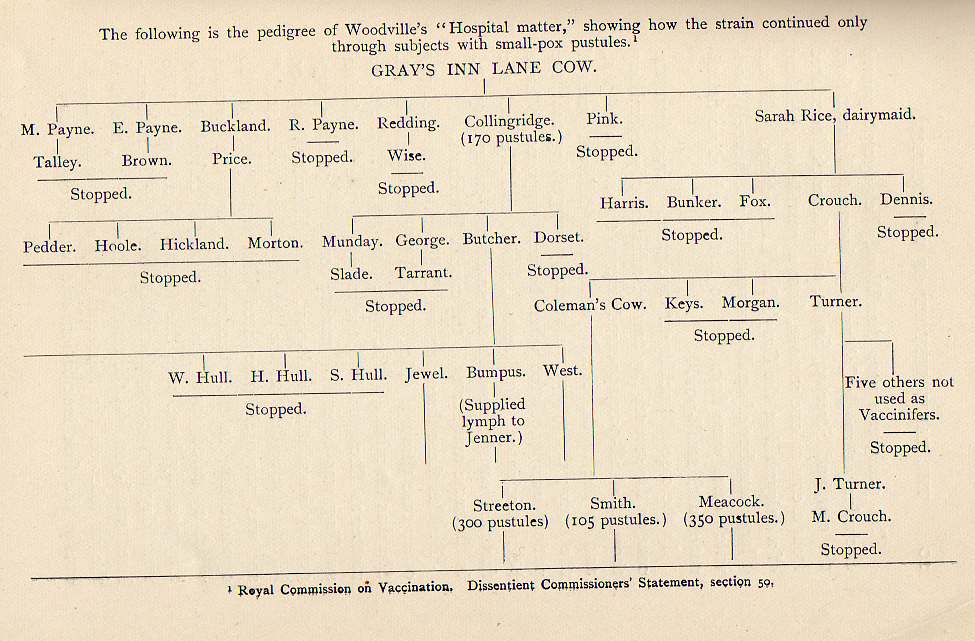
This pedigree shows that Woodville's lymph passed exclusively through Collingridge, inoculated direct from the cow, and Streeton, Smith, and Meacock, inoculated from a cow at one remove, from a pustule on the hand of a dairymaid at the Gray's Inn Lane dairy. All had a large number of small-pox pustules, and hence Woodville's cases were from first to last hopelessly contaminated with small-pox.
In the case of Buckland, "vaccinated " direct from the cow, on the seventh day two pustules exactly resembling those of small-pox appeared near to the inoculated part, and on the tenth, several pustules on different parts of the body; the symptoms strongly suggesting that the patient was inoculated when he was supposed to have been vaccinated. In Streeton, Smith, and Meacock the facts are consistent with the small-pox being acquired in the same manner as in the case of Buckland.
Besides these three persons, Collingridge was the only other case through which Woodville's strain continued. She was inoculated at the same time and with the same matter as Buckland, and, the margin of the inoculation swelling, was beset with minute confluent pustules, suggesting inoculated small-pox. The difficulty, however, in this case is that on the fifth day after "vaccination" she was purposely inoculated with small-pox (on the opposite arm to the "vaccination"), and the pustules which appeared about the body on the thirteenth day may possibly have been due to this inoculation. The usual day for the eruption to appear in ordinary inoculated small-pox was the tenth or the eleventh, and thus the pustules on the thirteenth day were rather late if due to the first inoculation, and early (eighth day) if
"VACCINATION" WITH VARIOLOUS LYMPH.
due to the second ; and therefore it is just as likely as not that Collingridge was variolated on her first inoculation.
Hence it is probable that the whole of Woodville's "Hospital matter" was contaminated at its sources, and the absence of pustules in two-fifths of the cases does not prove that these were of other than variolous origin ; for, as Dr. Collins and Mr. Picton1 say, "on the assumption that Woodville was dealing with arm-to-arm variolation, he only succeeded in obtaining what inoculators before and since claimed to have obtained when working with undoubted small-pox matter."2 There is the further argument that matter from secondary small-pox pustules in several instances produced only a local pustule in the next remove.
Woodville's lymph, when used by others away from the Hospital, produced eruptions : thus Jenner was supplied with a thread from Bumpus, who had three hundred and ten variolous pustules. In the first case inoculated by him, "spots" appeared on the face; and in the second, the local vesicle assumed "more perfectly the variolous character than is common with the cow-pox at this stage," and the areola was studded over with 'minute vesicles." Baron tells us that "the eruptions which attended many of the early cases of vaccination in London were unfortunately also propagated in different parts of the country, where the contaminated matter had been distributed by Dr. Pearson."3
Moore says:— '
'Variolous matter, under the denomination of vaccine lymph, was spread widely through England, and transported
1 Ibid.
2 Baron's "Life of Jenner," vol. i., p. 245.
3 Ibid, p. 339.to Germany, and even to the Island of Madeira, where a physician described the vaccine as a pustular disease."1
Woodville's lymph, or the "world's vaccine," as it has been called, had an enormous circulation both in England and abroad, at a time when Jenner had no stocks; it was this lymph, in fact, which convinced the world of the efficacy of vaccination.
In summing up the value of the Woodville evidence, Dr. Collins and Mr. Picton say:—
" It is, therefore, probable that the whole of Woodville's five hundred cases, which appeared to confirm Jenner's thesis, and secured the support of professional authority, were, in fact, only a series of mild variolations. It is certain that they were, from first to last, contaminated with small - pox. We agree with Professor Crookshank that, in either case, they must be set aside for the purpose of arriving at a decision as to whether uncontaminated cow-pox confers immunity towards small-pox. Woodville's cases, therefore, which did so much to establish the practice of vaccination, and which for nearly a century have been cited as demonstrating the truth of Jenner's doctrine, must be rejected as furnishing false evidence, and valueless as a scientific experiment."2
Although at first some of the cases inoculated with Woodville's lymph were undoubtedly infectious, after a time, whether from attenuation or dilution of the original matter, from the selection of mild cases, or from other causes, the number of pustules
1 "History of Vaccination," p. 36.
2. Royal Commission on Vaccination. Dissentient Commissioners' Statement, section 51
LANGWORTHY AND ARSCOTT'S EXPERIMENTS.
diminshed. Thus Woodville, writing in June, 1799, with reference to three hundred and ten cases subsequent to the Reports, says:—
"Out of the first hundred, nineteen had pustules, out of the second thirteen, and out of the List hundred and ten only seven had pustules."1
The pustular eruptions ultimately ceased, and the appearances came to assume the ordinary phenomena of vaccination.
That small-pox matter may, by a judicious selection of cases or lymph, be so attenuated as to produce restricted effects, which might be mistaken for the appearances generally recognised as pertaining to ordinary vaccination, is illustrated by the experience detailed by Mr. John Mudge, of Plymouth ; but these cases differ from Woodville's recorded results, in that when they were subsequently inoculated with small-pox, they were found unprotected.
Mr. Mudge2 relates that Messrs. Langworthy and Arscott, surgeons at the neighbouring town of Plymton, inoculated forty patients in 1776. In thirty the operation was performed "with crude matter from the arm of a young woman, five days after she herself had been inoculated with concocted matter. (She had smart fever and eruption later.) The other ten were done with concocted matter from a pustule of the natural small-pox. All the forty took, "and the latter ten, after the eruptive fever, had the small-pox in the usual way," but "of the other thirty, though the infection took place on their arms so as to inflame them considerably, and to produce a very large prominent pustule, with matter in it, on
1 Medical and Physical Journal, vol. i., p. 417. (July, 1799.)
2 "A Dissertation on the Inoculated Small-pox," pp. 20, 21. London. 1777.
each of them, yet not one had any eruptive fever or a single subsequent eruption on any part of the body ; but about the eighth, in some the ninth, and in others the tenth day, the inflammation began to disappear, and about the twelfth or thirteenth the pustules on their arms scabbed off." Matter from those pustules inoculated on others "produced on them exactly the same appearances, unattended also with either fever or smallpox."
The whole thirty were re-inoculated (no date given), this time with concocted matter taken subsequently to the eruptive fever, five being done from natural and twenty-five from artificial small-pox. The result was that "every one of them had the eruptive fever, and succeeding eruptions; in short, they had the small-pox in different degrees, but all in the usual way of inoculated patients."
These experiments differ from those described by Woodville. In criticising variolous tests in general we must always remember, as the Commissioners have pointed out, "that, in this as in other things, a sanguine hasty person might be led by the desire of seeing his expectations fulfilled to minimise the effect of the operation ; he might be led to overlook results which a more cautious observer would regard as evidence that smallpox had been really produced."
Now Woodville's tests are by no means perfectly satisfactory. In some of the early cases,1 which he described individually and in more detail, he obtained
1 In the case of George Reed (No. 33) Woodville says: "He was afterwards {i.e., after the fourteenth day) inoculated with variolous matter, which formed a pustular appearance; but no disorder was produced."
OPINION OF THE ROYAL COMMISSION.
slight local appearances, whereas in the latter ones the results of the tests are for the most part given collectively, and we obtain such vague expressions as "no disease ensued ;" concerning Nos. 89, 90, and 91 we read, "none of the above three patients took the small-pox," and in referring to sixty-seven tests (Nos. 132 to 200, omitting Nos. 193 and 194), all the information we have is that "the above patients . . . had variolous matter inserted in their arms . . . but it produced no disorder." If Woodville had given details in each instance, it seems probable that a considerable number would have been described as presenting some local manifestation, and if, as suggested by the Commissioners, we are to make allowance for the expectant attitude of mind betrayed by the sanguine experimenter, these cases were evidently not so immune as generally believed ; but, as shown above, even if we accept the position that the whole of Woodville's four hundred cases were immune to inoculated small-pox, this proves nothing in favour of Jenner's thesis.
Instances of the variolous test breaking down were not uncommon. Thus a surgeon, named Boddington, found in the case of his own child that the inoculation test produced not only a local pustule, but also a general small-pox eruption. He wrote to Jenner on the subject, who replied, "How a gentleman, following a profession the guardian angel of which is Fame, should have so committed himself as to have called this a case of smallpox after cow-pox, is not only astonishing to me, but must be so to all who know anything of the animal economy."1
1 Baron's " Life of Jenner," vol. i., p. 445.
Baron refers to this as a sample of Jenner's method of dealing with "rumours" of this kind. Ultimately Jenner discarded the test, for in 1804 he writes:—
"I will just remark that the fairest of all tests is exposure to variolous contagion. This is the natural test; inoculation is not. Who does not know (all medical men ought to know) that the insertion of the variolous poison into the skin of an irritable person will sometimes produce great inflammation, disturbance of the system, and even eruptions ? " 1
1. Letter from Jenner to Dunning, July 22, 1804. Baron's "Life of Jenner," vol. ii., p. 339.
Any other evidence brought forward by Jenner is entirely discounted by his invention of the term "spurious cow-pox." This was first used to describe cases of cow-pox which did not originate from grease in the horse, and subsequently as an excuse when it was discovered that the vaccinated were liable to be attacked by small-pox. In his paper on "The Origin of the Vaccine Inoculation," he gives the following ingenious explanation:—
"In the course of the investigation of this subject, which, like all others of a complex and intricate nature, presented many difficulties, I found that some of those who seemed to have undergone the cow-pox, nevertheless, on inoculation with the small-pox, felt its influence just the same as if no disease had been communicated to them by the cow. This occurrence led me to enquire among the medical practitioners in the country around me, who all agreed in this sentiment— that the cow-pox was not to be relied upon as a certain preventive of the small-pox.
" This for a while damped, but did not extinguish, my ardour; for, as I proceeded, I had the satisfaction
to learn that the cow was subject to some varieties of spontaneous eruptions upon her teats ; that they were all capable of communicating sores to the hands of the milkers, and that whatever sore was derived from this animal was called in the dairy the cow-pox.
" Thus I surmounted a great obstacle, and in consequence was led to form a distinction between these diseases, one of which only I have denominated the true, the others the spurious cow-pox, as they possess no specific power over the constitution."
I may here remark that Jenner never gave any signs by which the true and spurious cow-pox could he distinguished, and the mystery remains unsolved until this day.
In some concluding remarks of the "Inquiry," he relates the cases of Hannah Pick and Elizabeth Sarsenet, who contracted cow-pox with all the other servants at a farm in the parish of Berkeley. These cases fairly puzzled him; for Hannah, when inoculated with smallpox, was found protected; but Elizabeth, on exposure to the infection, contracted the disease. In the latter case, although there were multiple vesicles, there was no glandular or constitutional affection. Jenner says:—
" This impediment to my progress was not long removed before another, of far greater magnitude in its appearances, started up. There were not wanting instances to prove that, when the true cow-pox broke out among the cattle at a dairy, a person who had milked an infected animal, and had thereby apparently gone through the disease in common with others, was liable to receive the small-pox afterwards."
Baron observes—
"Most men would, at this stage, have abandoned the investigation in despair. It was not so with Jenner."1
Jenner continues—
" This, like the former obstacle, gave a painful check to my
fond and aspiring hopes; but reflecting that the operations of nature are
generally uniform, and that it was not probable the human constitution (having
undergone the cow-pox) should in some instances be perfectly shielded from the
small-pox, and in many others remain unprotected, I resumed my labours with
redoubled ardour.
"The result was fortunate, for I now discovered that the virus of cow-pox was
liable to undergo progressive changes, from the same causes precisely as that of
smallpox, and that when it was applied to the human skin in its degenerated
state, it would produce the ulcerative effects in as great a degree as when it
was not decomposed, and sometimes far greater; but, having lost its specific
properties, it was incapable of producing that change upon the human frame which
is requisite to render it unsusceptible of the variolous contagion; so that it
became evident a person might milk a cow one day, and, having caught the
disease, be for ever secure, while another person milking the same cow the next
day might feel the influence of the virus in such a way as to produce a sore or
sores, and in consequence of this might experience an indisposition to a
considerable extent; yet, as has been observed, the specific qualities being
lost, the constitution would receive no peculiar impression."
1 Baron's " Life of Jenner," vol. i., p. 132.
CONDEMNED BY THE COLLEGE OF PHYSICIANS.
Only think of the absurdity of it. One day matter from the nipple of the cow, when inoculated on a human being, produces true cow-pox, and renders that person for ever afterwards secure from small-pox ; the very next day matter from the same cow will produce identical symptoms, but the cow-pox having lost its specific properties, the second person remains entirely unprotected !
The " spurious cow-pox " cry contributed largely to establish vaccination; for before the Committee appointed by the House of Commons to consider Jenner's claim for reward, some of the leading medical men gravely asserted that cases of failure must have been done with spurious matter.
It is only fair to mention that this explanation was condemned by the College of Physicians. "Some deviations from the usual course have occasionally occurred, which the author of the practice has called spurious cow-pox, by which the public have been misled, as if there were a true and a false cow-pox."1 This condemnation, however, came too late to arrest the mischief, for cow-poxing had already become an established practice.
It was also unfortunate that the early opponents of vaccination were almost entirely an interested opposition, being pledged to small-pox inoculation ; and it was especially unfortunate that if they had questioned the validity of the variolous test they would have exposed their own nostrum, which, as I have shown, was in some cases little else than an imposture.
1 Report of the Royal College of Physicians of London on Vaccination. (Ordered to be printed by the House of Commons, July 8, 1807.)
Another thing which largely contributed to establish vaccination was the misleading name of " variolś vaccinś" or small-pox of the cow, given to the disease by Jenner; and this, giving as it did a truly scientific ring, most materially assisted the cow-pox propagandists in their innovation. The theory that cow-pox was smallpox of the cow was quite new to the veterinary surgeons and other practical people of that time, and was objected to by one of Jenner's leading contemporaries, Dr. George Pearson, on the ground that "cow-pox is a specifically different distemper from the small-pox in essential particulars, namely, in the nature of its morbific poison, and in its symptoms." Dr. George Gregory, a more recent authority, was also entirely opposed to the identity theory. "On all these grounds, I demur to the theory of identity, and hold that small-pox and cow-pox are antagonistic affections—that cow-pox, instead of being, as Dr. Baron maintains, of a variolous, is, in fact, of an anti-variolous nature—that it alters and modifies the human constitution so as to render some individuals wholly, others partially, and for a time, unsusceptible of small-pox."1 The total unlikeness of cow-pox to smallpox in all respects, save their names, has been much dwelt upon by several modern pathologists,2 to whose writings I refer my readers.
1 "Lectures on the Eruptive Fevers," p. 207. London. 1843.
2 " Vaccine et Variole" p. 100. Chaveau. Paris. 1865. "Human
and Animal Variolce" p. 4. George Fleming, F. R.C.V. S. London.
1881. " The Natural History of Cow-pox and Vaccinal Syphilis." Charles
Creighton, M. D. London. 1887. " History and Pathology of Vaccination." Edgar M. Crookshank, M.B. (2 vols.) London. 1889.
CHAPTER 2.
THE DECLINE IN SMALL-POX SINCE THE INTRODUCTION OF VACCINATION.
The argument that small-pox has declined since the introduction and more efficient enforcement of vaccination is an important one. It is commonly asserted that in former times this disease raged like the plague,1 but a careful examination of the London Bills of Mortality will show the absurdity of the claim. In the whole history of small-pox it never raised the total deaths so as to make them stand out conspicuously among surrounding years ; but this was very far from being the case with the plague.
Burials within the London Bills of Mortality from plague and "all causes" for the plague years 1603, 1625, 1636, and 1665.2
Years. Deaths from plague. Deaths from all cause
1603 30,561 ....
37,294
1625 35,417
54,265
1636
10,400 ....
23,359
1665 ... 68,596
97,306
1 ''Your Committee, however, believe that, ... if vaccination had not been general, this epidemic (1871-72) would probably have become a pestilence, raging with destructive force, like the plague of the Middle Ages." (Draft Report proposed by the chairman of the Select Committee on the Vaccination Act, 1867.)
2 Second Report, Royal Commission on Vaccination, pp. 289, 290.
For the non-plague years, 1604-24, the average annual number of deaths from all causes was 8,548 ; for the years 1626-35, 8,986; and the years 1637-64, 12,554. It is thus evident that the plague made an enormous difference to the total mortality, which was never the case with small-pox.
Let us now see what small-pox was at its worst. The only continuous set of figures we have extending over a long period of time are those for London, and, in the absence of any reliable information about the population, we are forced to the imperfect method of comparing the ratios of deaths from small-pox to those for all causes. The following figures give the highest years for small-pox in the seventeenth, eighteenth, and nineteenth centuries :—
Deaths Deaths Ratio per 1,000
Years. from from from
small-pox, all causes. small-pox.
Seventeenth century (1634) 1,354 10,400 130
Eighteenth century (1796) 3,548 19,288 184
Nineteenth century (1871) 7,912 80,430 98
Although there is not a great difference between the maxima of the seventeenth and nineteenth centuries, a sensible decline has nevertheless taken place, for the small-pox epidemics appear at much less frequent intervals than formerly.
Since the commencement of the Registrar-General's returns in 1838 we have the advantage of exact figures, and the interval from this date to the present time may be conveniently divided by the great epidemic of 1871-72. It was during the first of these periods that all the important laws relating to vaccination came into force.
THE VACCINATION
ACTS.
In 1840 an Act (3 and 4 Victoria, cap. 29) was passed making it the duty of
Guardians to provide facilities for vaccination ; but it was not until 1853
(16 and 17
Victoria, cap. 100) that neglect of vaccination was made punishable by fine, or
imprisonment in default of distress.
The effect of this law was seen in the large increase of the number of vaccinations in 1854. By the Act of 1861 (24 and 25 Victoria, cap. 59), Guardians were authorised to appoint officers to institute and conduct proceedings for the purpose of enforcing obedience to the law. The most important Act of all, however, was that of 1867 (30 and 31 Victoria, cap. 84), which imposed on the Guardians the duty of seeing that children were duly vaccinated, and empowered them to pay any officer appointed by them to prosecute persons charged with offences against the Act.1 It also introduced a provision (section 31) to secure the vaccination of children born before the Act came into force ; but the most important provision of all was that relating to repeated penalties for the non-vaccination of the same child, and this harsh process of the law could hardly fail, in the then state of public opinion, to greatly increase the number of vaccinations. Referring to this Act, the Select Parliamentary Committee say—"Your Committee are glad to find that wherever the Guardians endeavour to carry out the law, it is very generally, and indeed almost universally, enforced;" and they proposed an amendment to the effect that the appointment of vaccination officers should be made obligatory—a suggestion which was embodied in the Act of 1871 (34 and 35 Victoria, cap. 98).
1. Dr. Seaton informed the House of Commons' Committee of 1871 that of two hundred and sixty Unions, inspected in 1870, only one hundred and twenty were reported as not having vaccination officers; a large number of these, however, had appointed officers since (before May, 1871).
The Act of 1871 made other alterations. By the 27th section of the 1867 Act, it was provided that the Guardians shall make inquiry, and " if they find that the provisions of the Act have been neglected, shall cause proceedings to be taken against the persons in default." This clause was repealed by the Act of 1871. The repeal of this section absolved the Guardians from the duty of prosecuting for the time being; but in 1874 an Act was passed (37 and 38 Victoria, cap. 75) empowering the Local Government Board to make "rules, orders, and regulations prescribing the duties of Guardians and their officers in relation to the institution and conduct of proceedings to be taken for enforcing the provisions of the said Acts (1867 and 1871)." The Local Government Board have acted on this power, and in their General Order, dated October 31, 1874, have introduced a clause (art. 16) which takes the place of the repealed 27th section of the Act of 1867.
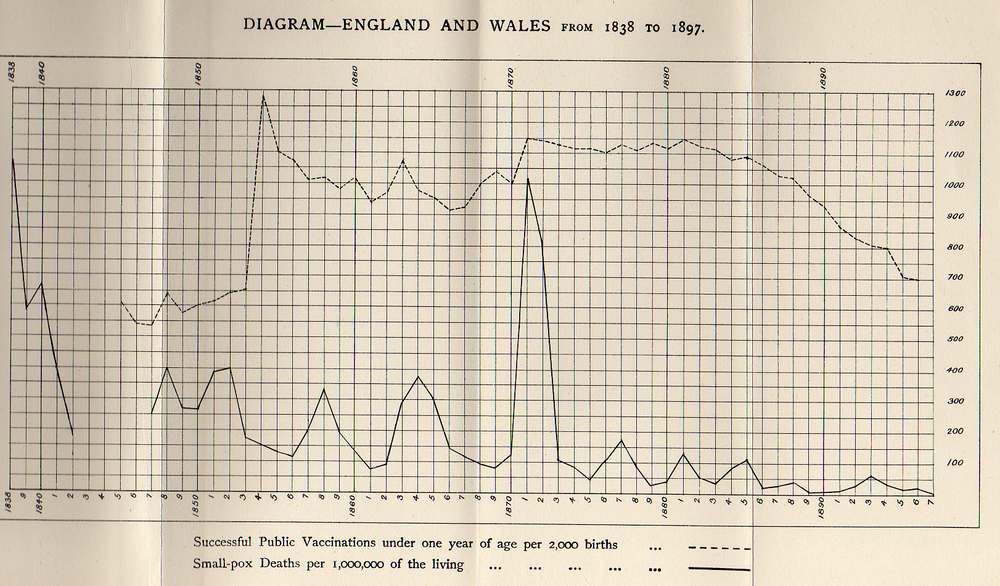
If we refer to the diagram in the Appendix, which gives the proportion of public vaccinations under one year of age to the births, from 1845 to 1895, we find that the Act of 1853 doubled the number of vaccinations; after this the number diminishes, to increase again in 1863-64. This increase was probably due to an outbreak of smallpox. After another decline, there is an increase of vaccinations in 1868-69, which may be attributed to the Act of 1867; and a still further rise in 1871, due, no doubt, to the great epidemic of small-pox then prevailing.
SMALL-POX AND VACCINATION SINCE 1872.
The effect of the legislation of 1871 is not apparent, for there is no further increase in the number of vaccinations in 1872, when the Act came into operation.
Another method of testing the increasing efficiency of the Vaccination Acts is the proportion of the small-pox cases vaccinated. The figures for the London Small-pox Hospital work out as follows :—
Percentage of small-pox
Years. cases vaccinated.
1826-34 35
1835-45 44
1845-55 64
1855-65 78
1867 ...... 84
1871 92
An examination of the diagram referred to shows that with the gradually increasing proportion of the population vaccinated there is no diminution in smallpox, and the epidemic of 1871-72, coming when England was thoroughly vaccinated, points forcibly to the inutility of the operation.
Let us now examine the history of small-pox and vaccination subsequent to the great epidemic. The same diagram shows that the infantile public vaccinations remained practically stationary until 1881 or 1882, when they began to decline; from 1881 to 1895 they decreased from 57-3 to 35-1 per cent, of the births, which is a considerable reduction. It will be seen that since the great epidemic (1871-72), and coincident with the decline in vaccination, small-pox has diminished, and quite recently markedly so.
An examination of the statistics for London, since the opening of the hospitals of the Metropolitan Asylums Board, also shows conclusively that the enormous decline in the small-pox mortality in recent years cannot be attributed to vaccination. The figures are taken from the last published reports of the Metropolitan Asylums Board (1895) and the Local Government Board (1895-96).
Estimated Smallpox Percentage of births
population in the Deaths from death-rate not finally accounted
Years- middle of each small-pox. per million for in regard to
year. ' vaccination.
1871 3,267,251 7,912 2,421 No return.
1872 3,319,736 1,786 537 8.8
1873 3,373,065 113 33 8.7
1874 3,427,250 57 16 8.8
1875 3,482,306 46 12 9.3
1876 3,538,246 736 207 6.5
1877 3,595,o85 2,551 709 7.1
1878 3,652,837 1,417 387 7.1
1879 3,711, 517 450 120 7.8
1880 3,77i,i39 471 124 7.0
1881 3,824,964 2,367 617 5.7
1882 3,862,876 430 110 6.6
1883 3,901,164 136 34 6.5
1884 3,939,832 1,236 307 6.8
1885 3,978,883 1,419 347 7.0
1886 4,018,321 24 5 7.8
1887 4,058,150 9 2 9.0
1888 4,098,374 9 2 10.3
1889 4,138,996 — — 11.6
1890 4,180,021 4 1 13.9
1891 4,221,452 8 2 16.4
1892 4,263,294 41 10 18.4
1893 4,306,411 206 48 18.2
1894 4,349,166 89 22 Returns not yet
1895 4,392,346 55 13 published.
Thus it will be seen that with an increasing proportion of the population vaccinated, up to the great epidemic of 1871-72, there was no corresponding decline in the small-pox mortality, and more recently, while the reduction in small-pox has been enormous, the vaccinations have also declined.
As pointed out above, however, if this century be compared with the two previous ones, a large decline in small-pox has taken place; and this has been accompanied by an equal if not a greater decline in another zymotic disease, which is spread by overcrowding and insanitation—viz.: typhus fever. In 1685-86 the country suffered from a severe epidemic of a fever which has been described by Sydenham, and, according to Dr. Murchison,1 presented all the symptoms of typhus—viz.: headache, pains in the limbs, dry brown tongue, delirium, and an eruption resembling that of measles, and often accompanied by true petechiae. According to the London "Bills" there were 3,832 deaths from fever in 1685, or a rate of 165 per 1,000 of the total deaths (23,222) in the year; and 4,185 deaths in 1686, or one of 185 per 1,000 (total deaths, 22,609).
1 "The Continued Fevers of Great Britain," p. 30. Second edition. 1873-
The most severe fever year was in 1741. In London 7,528 died, or a rate of 234 per 1,000 from all causes (32,169). This considerably exceeds the figures for small-pox, which, at its worst, in 1796, had only a rate of 184 per 1,000 total deaths. Dr. Murchison, in speaking of the fever epidemic in 1741 (p. 34), says:—
In London it is said to have broken out among the poor, who had been half-starved for two years, and obliged to eat uncommon and unwholesome things. In all the accounts mention is made of the eruption : in some cases it is described as like that of measles, in others as like so many small flea-bites, while in a few instances it is said to have been mixed up with petechiae and vibices."
From the description given by one of the writers at the time—Barker,1 of Salisbury—there can be but very little doubt that this epidemic was one of true typhus. The patient, after having languished for several days, was seized with rigors or cold chills, and with a heavy pain in the forehead or over the eyebrows, which rendered him stupid and dejected. About the seventh day petechiae or spots sometimes appeared upon the breast or arms; these were commonly of a pale red colour, like measles, and sometimes purple, like so many small flea-bites. In a very few the eruption was of a deep violet colour, and in others very broad, like scurvy spots or bruises. In the later stages the patient became delirious, the breathing was often laboured, and there was also convulsive twitching of the tendons, and fumbling with the bedclothes.
1 " An Inquiry into the Nature, Cause, and Cure of the present Epidemic Fever," pp. 39-42. J. Barker, M.B. London. 1742.
In 1837-38, epidemics of small-pox and typhus took place simultaneously. In England and Wales, during the eighteen months ending December 31, 1838, 27,822 died from typhus, and 22,079 from small-pox ; while in the Metropolis, during the same period, there were 6,011 deaths from typhus, and 4,580 from small-pox. In London we know that this epidemic of fever was almost wholly typhus. Of sixty cases in 1837-38, of which notes were kept by West, under Latham, at St. Bartholomew's Hospital, none that died and were examined post-mortem had ulcerations of Peyer's patches, pathognomonic of enteric or typhoid fever, although some had congestion of Peyer's patches, the cases being all reckoned typhus exanthematicus.1 Sir Thomas Watson has also testified to the nature of this epidemic :—
" Fever is very rife in St. Giles's, and in other crowded parts of this town, just now (1838). Our wards at the Middlesex are full of it; and scarcely a case presents itself without these spots. We speak of it familiarly as the spotted fever, or (from the resemblance which the rash bears to that of the measles, hereafter to be described) as the rubeoloid fever."2
1 "A History of Epidemics in Britain," vol. ii., p. 194. Creighton.
2 " Lectures on the Principles and Practice of Physic," vol. ii., p. 732.
The 1847 epidemic of fever in England was almost entirely one of typhus, there being 30,320 deaths, or a number considerably exceeding any year for smallpox over the whole period of registration. Since this epidemic, typhus fever has largely diminished ; but it has been noticed that at the London Fever Hospital all the great annual rises in the deaths from fever in London since 1849 (after which year enteric fever and typhus were first separated in the returns of the Hospital) have corresponded to a greatly increased admission of typhus, and not of enteric cases.
In the returns of the Registrar-General it was separated from enteric fever in 1869; and from 1871-75 to 1891-95 the average annual typhus death-rate in England and Wales has declined from 81 to 4 per million, or a fall of 95 per cent, on the earlier rate. The fact that this complaint, which was formerly more prevalent than small-pox, should have diminished to such an extent as to have become practically extinct, has a very important bearing on the decline of small-pox, for it is admitted that typhus fever is a disease which is spread by overcrowding and insanitation, and in a subsequent chapter it will be seen also that small-pox is largely disseminated in the same manner.
The following table shows the decline that has taken place in small-pox, fever, typhus fever, and scarlet fever since the commencement of registration. It is divided into five-year periods.
England and Wales.—Average annual death-rate per million living, from small-pox, fever,1 typhus fever, and scarlet fever, in five-year periods from 1838-95.2
Years. Small-pox.3 Fever. Typhus fever. Scarlet fever.
1838-42 576 1,053 — —
1847-50 (4 years) 292 1,246 — —
1851-55 248 983 — —
1856-60 198 842 — —
1861-65 219 922 — 982
1866-70 105 850 — 960
1871-75 408 599 81 759
1876-80 82 380 34 680
1881-85 83 273 23 436
1886-90 16 202 7 241
1891-95 24 185 4 182
Over the whole period it will be found that the small-pox death-rate declined 96 per cent., while fever declined 82 per cent. But the most extraordinary feature of the table is the large small-pox death-rate in 1871-75,
1 The term "fever" includes typhus, typhoid, and simple and ill-defined fevers.
2 From 1843-46 the causes of death were not abstracted.
3 The figures for small-pox include chicken-pox.
twenty years after vaccination had been made compulsory. Thus, between 1838-42 and 1871-75 the death-rate from small-pox had only abated 29 per cent., while fever diminished 43 per cent.; and, therefore, since the commencement of registration there was practically no important decline in small-pox until after the 1871-72 epidemic, although the death-rate from fever had materially diminished. Let me call attention to what has happened with the other diseases in the table. Since 1871-75, typhus (for which we have no State-enforced preventive inoculation) has declined 95 per cent, or a fall as great as there has been in small-pox over the whole period of registration ; and scarlet fever shows the important reduction of 81 per cent, since 1861-65.
An objection has been made to the fever figures, on the ground, it is said, that formerly fever included other diseases, such as pneumonia, influenza, etc., which now appear under their respective headings. The following quotation, however, from the Registrar-General's forty-second annual report (1879) proves that this is not the case to any large extent. The cause of the decline is also explained. The Registrar-General says (p. xxx.):—
" Had the deaths from one or more of this group of causes fallen, while those from others in the same group had risen, or had the fall been trifling, or the totals dealt with insignificant in amount, it might have been suspected that the alteration was a mere alteration in name. But as the deaths under each heading have declined, as the fall in the death-rate from them has been enormous— 62.4 per cent, in the course of ten years—and as the totals are by no means small, it may be accepted as an indisputable fact that there has in truth been a notable decline in these pests, and it may be fairly assumed that the decline is due to improved sanitary organisation."
I will now allude to the alterations that have taken place from time to time in the age-incidence of the small-pox mortality. Dr. Creighton has pointed out that, in all probability, in the seventeenth century smallpox was more a disease of adults than in the eighteenth century, when it was largely a disease of children ; at any rate, it was on account of its incidence on adults that the disease obtained its evil repute. In the diary of John Evelyn, we read that he himself had small-pox when a young man. His two daughters died of it in early womanhood within a few months of each other; and a suitor for the hand of one of them died of it about the same time. Among the medical writers, Willis gives four cases, all in adults ; and Morton, sixty-six clinical cases of small-pox, twenty-three of which were under twelve and the rest over twelve years of age.1
Again, in their writings the physicians of that time indicated that small-pox was a mild disease in infants. Willis says, "There is less danger if it should happen in the age of childhood or infancy;" again, "the sooner that anyone hath this disease, the more secure they are, wherefore children most often escape."2 Dr. Walter Harris, in a treatise on the acute diseases of infants, says :—
" The small-pox and measles of infants, being for the most part a mild and tranquil effervescence of the blood, are wont to have often no bad character, where neither the helping hands of physicians are called in, nor the abounding skill of complacent nurses is put in requisition." 3
1 "A History of Epidemics in Britain," vol. ii., pp. 443, 444. Creighton.
2 Thomas Willis, M.D., on "Fevers." Translation by S. Pordage, pp. 139, 142. London. 1681.
3. "A History of Epidemics in Britain," vol. ii., pp. 441. Creighton.
In the eighteenth century, on the contrary, the incidence of the small-pox mortality, especially in the manufacturing towns, was almost entirely on infants and young children, as is shown in the following table :1
Small-pox Small-pox Percentage
Years. deaths at deaths under under five years
all ages. five years of age. of age.
Kilmarnock, 1728-63 ... 622 563 90.5
Manchester, 1769-74 ... 589 559 94.9
Warrington, 1773 ... 209 197 94.3
Chester, 1774 ... 202 180 89.1
Carlisle, 1779-87 ... 241 229 95.0
In country districts, however, where small-pox appeared at less frequent intervals, there was time for the children to grow up without having the disease; and thus, in some instances, there were very few cases and deaths in the early years of life. Aynho, a small market town in Northamptonshire, is an instance in point. The following figures are recorded by the rector of the parish for fifteen months in 1723-24 : 2
Ages. Cases. Deaths.
0-1 ... — ... —
1-2 ... — ... —
2-3 3 - 2
3-4 4 1
4- 5 ... 6 ... 0
5-10 ... 15 ... 1
10-15 33 3
15-20 14 ... 1
20-25 16 ... 3
25-30 9 3
30-40 ...12 ... 3
40-50 . 10 ... 4
50-60 ... 4 ... 1
60-70 ... 4 ... 2
Above 70 ..2 ... 1
Total, 132 251 "A History of Epidemics in Britain," vol. ii., p. pp. 527, 536, 538, 554. Creighton.
2 Ibid., p. 520.
Thus, in the eighteenth century, although there may have been exceptions in some country districts, in towns the rule was for small-pox to be almost entirely a children's disease. This continued to be the case until after the 1837-38 epidemic. The Registrar-General first separated ages for all England in 1847, and the following table gives the proportion of small-pox deaths under five years of age from that time.
England and Wales.—For small-pox1 the deaths at all ages and under five, and the percentage of deaths under five to deaths at all ages in five-year periods from 1847-95.
Small-pox deaths Small-pox deaths Percentage
Years. at under under
all ages. five years of age. five years of age.
1847-50
(4 years) - 20,439 14,307 70.0
1851-55 ... 22,801 15,091 66.2
1856-60 ... 19,270 11,010 57.1
1861-65 ... 23,007 12,477 54.2
1866-70 ... 11,779 6,403 54.4
1871-75 ... 47,696 14,929 31.3
1876-80 ... 10,243 2,938 28.7
1881-85 ... 11,025 3,002 27.2
1886-90 ... 2,320 820 35.3
1891-95 ... 3,515 1,313 37.41 These figures include chicken-pox; if this disease be omitted from the calculations, 26 .9 per cent, of the total deaths from small-pox were under five years of age in the period 1891-95, or a percentage reduction of 62 since 1847-50.
INCREASE IN ADULT MORTALITY OF SMALLPOX
The figures in this table are corrected for chicken-pox; this disease was included with small-pox until 1874, but since that date chicken-pox deaths have been separately classified. My authority for adding them is contained on page x. of the fifty-second annual report of the Registrar - General (1889): —
"There were, however, eighty-three deaths ascribed to chicken-pox, and it is very probable that most of these were in reality cases of modified small-pox, true chicken-pox being an ailment that is rarely, if ever, fatal."
It will be seen from the table that over the whole period the percentage of deaths from small-pox under five years of age has declined from 70.0 to 37.4, or a percentage reduction of 47.
Not only has the children's share of the small-pox death-rate diminished, but at ages above ten the mortality has actually increased ; that is to say, there has been an age-shifting of the small-pox death-rate. This is shown by the following figures taken from the forty-third annual report of the Registrar-General (1880, p. xxii.).
England and Wales.—Mean annual deaths from small-pox at successive life-periods, per million living at each life-period.
Age periods 5. 5- 10- 15- 25- 45 and upwards.
Vaccination optional, 1847-53... 1,617 337 94 109 66 22
Vaccination compulsory, 1872-80 323 186 98 173 141 58
The increase in the adult mortality of small-pox during the period of compulsory vaccination has been urged by Dr. Bridges as a sufficient ground for altering the law. He thought that, if these facts had been generally known at the time, the Legislature would have hesitated before making vaccination compulsory. Dr. Collins and Mr. Picton1 have also shown that since the last century there has been an alteration in the share borne by children of the small-pox deaths independently of vaccination. From 1881 the Registrar-General has classified the small-pox deaths into three groups—the vaccinated, the unvaccinated, and those in which there is no statement. In the unvaccinated class, from 1881-93, there were in all 3,746 deaths, 1,483, or 39.5 per cent., of which were under five years of age ; during the last century, as pointed out above, the proportion under five years of age was more than double this figure. It is not easy to understand how vaccination can have brought about this change in the unvaccinated.
1 Royal Commission on Vaccination. Dissentient Commissioners' Statement, section 147.
Comparisons have been instituted with other diseases. In this connection Dr. Ogle, the late Superintendent of Statistics to the Registrar-General, informed the Royal Commission (Q. 516 and 518) that the zymotic diseases were the better ones with which to compare small-pox; but he said, "It is impossible to make similar comparisons in the case of scarlet fever or measles, and diseases that only affect children. Fever is the only one of the zymotic headings that you can take, because it is the only one that affects all ages to any extent. Fever is, therefore, the only one which it is possible to subject to this kind of investigation."
AGE-INCIDENCE OF TYPHUS FEVER.
The following table gives the children's proportion of deaths for fever in five-year periods from 1847-95. Corrections have been made for remittent fever. From 1869 to 1880 the deaths from remittent fever, under five years of age, were classed with typhoid, and therefore I have added these deaths to fever for the other years in the table—viz.: from 1847-68 and from 1881-95.
England and Wales.—For fever the deaths at all ages and under five, and the percentage of deaths under five to deaths at all ages in five-year periods from 1847-95.
Fever deaths Fever deaths Percentage
Years. at under under
all ages. five years of age. five years of age.
1847-50 ... 88,093 15,880 18.0
(4 years)
1851-55 ... 92,440 19,539 21.1
1856-60 ... 82,847 19,072 23.0
1861-65 95,723 19,166 20.0
1866-70 ... 94,057 17,352 18.4
1871-75 ... 70,109 12,994 18.5
1876-80 ... 47,524 8,375 17.6
1881-85 37,005 4,692 12.7
1886-90 ... 28,698 2,908 10.1
1891-95 ... 27,628 2,180 7.9
Over the whole period the children's proportion of deaths from fever has declined from 18 to 7.9 Per cent., or a percentage reduction of 56. This is greater or less than the figure for small-pox, according to whether the chicken-pox deaths are included or not in the smallpox totals.
Not only has there been an alteration in the age-incidence of fever as a whole, but there is every reason to believe that the same change has taken place in the several diseases composing the group. Except in quite recent years this is difficult to prove in the case of typhoid fever; but in typhus there is very little doubt that such has been the case. In order to compare present-day typhus with some former period, it is necessary to find, not only years of undoubted typhus, but also years in which the ages are separated. The epidemic years, 1837-38, are out of the question, because deaths were not classified at different ages ; but the epidemic took place later in the North of England, and for 1839 we have the figures for Manchester and Liverpool. I also give the statistics for all England and London for the epidemic of 1847, which was almost exclusively typhus fever.
Deaths from typhus fever at all ages and under five, with percentage under five years of age, for Manchester and Liverpool in 1839, and for England and Wales and London in 1847.
Typhus Typhus deaths Percentage
Years. deaths at under five under five
all ages. years of age. years of age.
Manchester1 ... 1839 323 51 15.8
Liverpool1 ...- ... 1839 305 46 15.1
England and Wales2 1847 30,320 4,364 14.4
England and Wales2
(excluding London) l847 27,136 3,823 14.1
London2 ...............1847 3,184 541 17.01 Third Annual Report of the Registrar-General, pp. 194 and 206.
2 Tenth Annual Report of the Registrar-General.
In 1869 the typhus deaths were separated from typhoid in the returns of the Registrar-General. The following gives the figures for typhus from 1871-95 for England and Wales and for London :—
Typhus
Typhus deaths
Percentage
Years
deaths at
under five
under under five
all ages
years
of age
years of age
England and Wales 1871-95 18,206
1,040
5.71
England and Wales"
(excluding London) l871-95
15,955
848
5.31
London ... ... 1871-95
2,251
192
8.53
Thus it would appear that there has been a great alteration in the age-incidence of typhus fever from the commencement of registration. Since the separation of typhus and typhoid fevers in the returns of the Registrar-General, both diseases have shown a change in this particular. The percentages under five years of age are as follows1:—
1871-75. 1876-80. 1881-85. 1886-90. 1891-95.
Typhus................ 6.4 6.1 3.5 3.4 5.1
Typhoid ... 17.4 16.0 11.2 8.4 6.6
In typhoid, there has been a marked change in the age-incidence ; but in typhus, the quinquennium, 1891-95, shows only a slight decline in the children's share of deaths as compared with the earlier period, 1871-75.
The age-shifting of the small-pox death-rate—that is to say, the lessened death-rate in children combined with an increased death-rate in adults—has been claimed as a "phenomenon" which is " without a parallel in the history of human mortality."2 Mr. Alfred Milnes3 has, however, pointed out that a similar "phenomenon " has occurred in the case of influenza.
1. The figures up to 1890 are those given by Mr. Alfred Milnes in The Vaccination Inquirer for February, 1893. The last column has been calculated by me from the returns of the Registrar-General. The typhoid fever percentages have been corrected for remittent fever deaths under five years of age.
2. "Vaccination Vindicated," p. 18. John C. M'Vail, M.D. 1887.
3. The Vaccination Inquirer, May, 1893.
The Registrar-General, in his fifty-fourth annual report (1891, p. xx.), gives the death-rates per million living at different ages in the influenza epidemics of 1847-48 and 1890-91.
Age-periods. Under 5- 5- 10- 15- 25- 35- 45- 55- 65- 75- 85-
1847-48... 713 80 49 51 79 139 284 809 2,372 5,510 11,243
1890-91... 306 55 46 115 197 347 595 1,060 1,985 3,355 4,821
On comparing this table with that on page 45, it will be seen that both small-pox and influenza show a decline up to ten years of age. In the next age-period, 10-15, the death-rate at both periods is nearly the same, while from fifteen onwards the later period shows a greater mortality from both diseases ; but the influenza mortality in persons aged sixty-five and upwards shows a decline in the later epidemic of 1890-91 as compared with the earlier one of 1847-48.
Before leaving the subject of age-incidence, I would draw the attention of my readers to a table in section 171 of the Final Report of the Royal Commission. It gives for England and Wales the deaths from smallpox at certain age-periods to 1,000 deaths from smallpox at all ages. The figures under one year of age are as follows :—
Deaths from small-pox under one
Years. year of age to 1,000 deaths from
small-pox at all ages.
1848-1854 ... 251
1855-1859 ... 231
1860-1864 ... 237
1865-1869 ... 231
1870-1874 ... 143
1875-1879 ... ............. 112
1880-1884 ... 113
1885-1889 112
1890-1894 166
From 1848-54 to 1855-59 the proportion of infantile small-pox deaths declined from 251 to 231, or a reduction of 8 per cent. The successful public vaccinations of infants under one year of age are given in the Appendix.1 On calculation it will be found that from 1848-54 they averaged 36.9 per cent, of the births, and from 1855-59,. 51-5 per cent.; that is to say, that between the two periods the proportion increased from 36.9 to 51.5 Per cent., or a percentage increase of 39.6. By a similar calculation, from 1865-69 to 1870-74 they increased from 48.5 to 55-6 per cent., or a percentage increase of 14.6. Between the latter periods the proportion of small-pox deaths under one year of age declined from 231 to 143, or a reduction of 38.1 per cent. To put it in tabular form :
Percentage increase
Percentage decline in the
in the proportion of
proportion of small-pox
successful public
deaths under one year
From the period vaccinations under
of age to 1,000
deaths
one year of age to from small-pox at
the births, all ages.
1848-54 to
1855-59...............
39.6
8.0
l865-69 to
1870-74................
14.6
38.1
It is obvious from the above that there is some cause other than vaccination contributing to the alteration that has taken place in the age-incidence of the smallpox mortality.
1 It will be observed in the Appendix that the returns are made up to September 29, but for the purposes of these calculations, the proportion of successful public vaccinations under one year of age to the births has been estimated to December 31 for the years in question.
There is another point on which the Commissioners have laid considerable stress. They show that at Leicester and Gloucester the proportion of small-pox deaths under ten years of age is greater than in the well-vaccinated towns of Sheffield and Warrington. The figures given are as follows :—
Small-pox Small-pox deaths Percentage
Epidemics. deaths under ten under ten years
at all ages. years of age. of age.
Warrington, 1892-93 ... 62 14 22.5
Sheffield, 1887-88 ... 500 128 25.6
London, 1892-93 ... 182 67 36.8
Dewsbury, 1891-92 ... 110 57 51.8
Gloucester, 1895-96 ... 434 280 64.5
Leicester, 1892-93 ... 21 15 71.4 (or 66.6) 11 At Leicester, in consequence of the proximity of a scarlet fever ward to the hospital in which small-pox cases were treated, several children in that ward were attacked by small-pox, of whom three died. The 66 .6 per cent, is obtained by deducting these three deaths.
If the reader will consult the diagram in the Appendix, he will find that England and Wales, for seventeen years previous to the epidemic of 1871-72, was very well vaccinated. In that epidemic there were 42,220 deaths from small-pox, of which 20,094, or 47.6 per cent., were under ten years of age. This is double the proportion at Warrington and Sheffield, and very nearly the same as at Dewsbury, where, according to the Commissioners, vaccination had been greatly neglected. In 1892, the second year of the Dewsbury epidemic, the percentage of children born and not finally accounted for with regard to vaccination was 377. In England and Wales, in 1872, the default was only 5.1 per cent.
As the Commissioners have, in two of the towns named, based their conclusions on a small number of deaths, perhaps I may be forgiven if I add the following :—
Small-pox Small-pox deaths Percentage
Epidemics. deaths under five under five years
at all ages. years of age. of age.
Mold,1 1871-72 ... 44 15 34.1
Willenhall,2 1894 ,.. 47 16 34.0
Keighley, 1893 ... 7 0 0.01 The local Registrar has kindly supplied me with the figures for the registration sub-district of Mold.
2 At Leicester, in 1892-93, of twenty-one small-pox deaths, nine were under five years of age. Two of these were among the children who suffered from the proximity of the scarlet fever ward to the hospital in which small-pox cases were treated. If these be deducted, 36.8 per cent, of the total deaths from small-pox were under five years of age, a proportion not much higher than that of Willenhall or Mold.
I shall have occasion to refer to Mold and Willenhall in subsequent chapters. It is sufficient to say here that at the time of their respective epidemics, both were very well-vaccinated districts. With regard to Keighley, there is no reason to believe it to be better vaccinated than Leicester or Gloucester ; indeed, evidence points to the contrary. I do not wish to infer from the experience of these districts that vaccination increases the share of the small-pox mortality borne by children ; the figures are too small for accurate inferences, as also are those of the Commissioners.
To sum up the contents of the present chapter, it will appear that, although there has been a marked decline in small-pox since the last century, there has been an equal, if not a greater, reduction in typhus fever. It has also been shown that since the commencement of registration the vaccination of a gradually increasing proportion of the population previous to the great epidemic of 1871-72 had very little effect on the smallpox death - rate, although there was an appreciable diminution in fever. From this epidemic to the present time, with an increasing neglect of vaccination since 1881, an enormous decline in small-pox has taken place, and a corresponding diminution in typhus and scarlet fevers ; the reduction in all three diseases being due, no doubt, in large measure to the sanitary improvements introduced by the Public Health Act of 1875.
With regard to the age-incidence, when small-pox first began to be much known, in the Stuart period, it was chiefly as a malady attacking adults ; as it became more generally diffused, in the eighteenth century (except in a few country districts where epidemics came infrequently), it was almost entirely a disease of childhood; and more recently it is recognised again as a disease attacking adults as well as children. That this is not due entirely, or even principally, to vaccination, seems clear from the fact that a similar alteration of incidence has taken place in the unvaccinated. Another notable point is that, since the commencement of registration, the most important decline in the proportion of infantile small-pox deaths has not coincided with the period representing the greatest increase in the public infantile vaccination; nor is there sufficient evidence to show that the children in well-vaccinated towns suffer less than in those districts where vaccination has been largely neglected. When we come to compare the behaviour of other diseases in this particular, we find that in the only group which are fairly comparable with small-pox a similar change has been observed.
Before concluding the chapter, I must allude to a favourite argument in defence of vaccination, which seems to weigh with a large number of people—that is, the rarity of pock-marked faces at the present time, as compared with some former period. As to the disfigurement of the population in the seventeenth and eighteenth centuries, there is little or no evidence; but it is significant that in the issues of the London Gazette,1 from 1667-1774, of one hundred advertisements for runaway apprentices, servants who had robbed their masters, horse-stealers, highwaymen, etc., only sixteen were described as more or less marked with small-pox, four being black men or boys. This consecutive hundred included only those who were so particularly described in feature that pock-marks would have been mentioned had they existed. Apparently pock-marked faces were not so common as is generally imagined.
1 "A History of Epidemics in Britain," vol. ii., p. 454. Creighton.
The argument that vaccination has lessened the number is an old one, for in their annual report for 1821 the National Vaccine Board say : "We appeal confidently to all who frequent the theatres and crowded assemblies, to admit that they do not discover in the rising generation any longer that disfigurement of the human face which was obvious everywhere some years since." In the report for 1825 we read: "What argument more powerful can be urged in favour of vaccination, than the daily remark which the least observant must make, that in our churches, our theatres, and in every large assemblage of the people, to see a young person bearing the marks of small-pox is now of extremely rare occurrence ?" Haifa century afterwards, in 1872, The Lancet, of June 29 (vol. i., p. 907), lamented "the growing frequency with which we meet persons in the street disfigured for life with the pitting of small-pox. Young men and, still worse, young women are to be seen daily whose comeliness of appearance is quite compromised by this dreadful disease."
Thus, while with the limited vaccination of 1825 the disfigurement of the young was extremely rare, yet, after nineteen years of compulsion, pock-marked faces had conspicuously increased. It is difficult to construct any scientific theory of protection from these facts, and we may therefore conclude that the argument so often brought forward as conclusive is illusory and untrustworthy.
CHAPTER 3.
SOME OF THE CAUSES OF THE DECLINE IN THE SMALL-POX MORTALITY.
In the last chapter attention was directed to the fact that although some of the epidemics of small-pox in the present century have been nearly as severe as those of the two previous ones, yet they took place at longer intervals; and thus there has been an important reduction in the mortality from this malady. The disease began to subside, however, before the introduction of vaccination, and was part of a general improvement in the public health which was taking place about this time. This is seen in the following table compiled by Dr. Farr.
London.—Average annual death-rates per 100,000 living at six different periods, from 1629-1835.1
All causes. Small-pox.2 Fever.
1629-35 ... ... 5,000 189 636
1660-79 .................. 8,000 417 785
1728-57 ...................... 5,200 426 785
1771-80 ... ... 5,000 502 621
1801-10 ... ... 2,920 204 264
1831-35 ............. 3,200 83 1111 "M'Culloch's Statistical Account of the British Empire," vol. ii., p. 579. Second edition. London. 1839.
2. In a pamphlet by Mr. Ernest Hart, entitled "The Truth About Vaccination" (1880, p. 35), it is stated that "In Dr. Farr's valuable article on Vital Statistics in M'Culloch's 'Account of the British Empire,' it is shown that in the twenty-seven years, 1629-35 and 1660-79, the annual mortality from small-pox in London was equal to nearly 16,000 per million persons living; and in the forty years, 1728-57 and 1771-80, to nearly 18,000 per million living." It is not at first sight apparent how these high rates have been deduced from Dr. Farr's figures.
Commenting on these figures, Dr. Farr says :—
" Smallpox attained its maximum mortality, after inoculation was introduced. The annual deaths of small pox registered 1760-79 were 2,323 ; in the next twenty years, 1780-99, they declined to 1,740; this disease, therefore, began to grow less fatal before vaccination was discovered, indicating, together with the diminution of fever, the general improvement of health then taking place."
Considering, also, that since the commencement of registration smallpox has completely ignored the fluctuations in the amount of vaccination, it is begging the question to assume that this is in any way relevant to the diminution that has been recorded. I propose, therefore, in the present chapter, to indicate some of the causes which have led to the decline of the disease.
It will be convenient at this juncture to consider the effect produced on the small-pox mortality in the displacement of small-pox inoculation by vaccination. As it was only in rare instances, that the inoculated were subjected to any form of isolation, it cannot be denied that they must often have acted as centres of infection and have diffused the disease. Dr. Wagstaffe,1 writing in 1722, related an instance where, in consequence of a few inoculations, small-pox was spread in the town of Hertford, and occasioned a considerable mortality. In Paris, in 1763, the unusual severity of small-pox was attributed
1 A Letter to Dr. Freind, p. 38. London. 1722.
SMALL-POX DIFFUSED BY INOCULATION.
to increased infection from inoculation, and a decree was issued prohibiting the practice. The advocates of vaccination were almost unanimous in their opinion, that inoculation was responsible for much loss of life from small-pox; thus Moore1 declared, that the neglect of the precaution of preventing the spread of infection from the inoculated had "occasioned the loss of millions of lives." The last statement must, however, for obvious reasons, be received with caution.
If we consult the London Bills of Mortality, we find that the small-pox mortality in the eighteenth century exceeded that of the seventeenth century. There are reasons, however, for believing that other causes besides inoculation must be sought for to explain the high small-pox rates in the eighteenth century. One of these is, that small-pox rose to a higher level of mortality about the year 1710; whereas inoculation was not introduced into this country until 1721. Dr. Creighton2 informs us, that "from 1721 to 1727 the inoculations in all England were known with considerable accuracy to have been 857; in 1728 they declined to 37; and for the next ten or twelve years they were of no account." In London inoculation was revived about 1740, and after a few years became a lucrative branch of surgical practice, but was restricted almost exclusively to the well-to-do.
1 "History of Small-pox," pp. 232, 233. James Moore. London. 1815.
2. " A History of Epidemics in Britain," vol. ii., p. 504.
Gratuitous inoculation commenced with the opening of a hospital in 1746; but it was not till 1751-52, that any considerable number of people were inoculated in connection with the charity.
According to the London Bills it does not appear that the few inoculations which took place during the years 1721-28 had any appreciable effect on the smallpox mortality, nor should we expect them to do so ; but if a diagram be prepared showing year by year the rates of small-pox deaths to those for all causes, it will be found that from 1751 to 1781 a still higher level of small - pox mortality was reached than that which prevailed from 1710 to 1751 ; this seems to suggest an inoculation factor in the case. After 1781 smallpox was certainly at a lower level than that obtained between 1751 and 1781 (although in the one year, 1796, it touched the highest point in the century). This diminution, as Dr. Farr has pointed out, was associated with a decline in the general death-rate, and was no doubt brought about by the sanitary improvements introduced at that period ; and thus small-pox became less prevalent, in spite of the fact that inoculation still remained in full operation.
To sum up the case, it is evident that the large mortality from small-pox in the last century cannot be wholly attributed to inoculation ; but from the facts here presented I am led to believe that the augmentation which took place in 1751, and continued for a large number of years, might with fairness be put down to this cause. The first sign of any diminution in the small-pox death-rate commenced after 1781. This cannot be due to any falling off in the amount of inoculation, but must be associated with a general improvement in the public health then observable ; the further decline after the introduction of vaccination was in part probably brought about by the substitution of a non-infectious process.1
FLUCTUATIONS IN SMALL-POX MORTALITY.
One of the causes of the spread of small-pox is overcrowding and want of air-space in and around houses. The fifth annual report of the Registrar-General gives the country and the town mortality from various causes for the four years 1838-41 ; in the case of small-pox the former is 507, and the latter 1,045 Per million ; for all causes the figures are 19,300 and 27,073 respectively. This shows, that small-pox is much more influenced by the aggregation of the population than by all other causes of disease combined. The mortality from smallpox appears to vary according to the greater or lesser proportion of open spaces in towns. The following table illustrates this point.
1 As most of the lymph with which the early " vaccinations" were performed was of variolous origin, it is important to show that after a time the cases inoculated with Woodville's lymph ceased to be infectious. The following, in a letter from Jenner to Lord Egremont (Baron's " Life of Jenner," vol. i., p. 342), is very much to the point. Referring to the threads distributed by Dr. Pearson, Jenner says : "In many places where the threads were sent, a disease like a mild small-pox frequently appeared ; yet, curious to relate, the matter, after it had been used six or seven months, gave up the variolous character entirely, and assumed the vaccine; the pustules declined more and more, and at length became extinct. I made some experiments myself with this matter, and saw a few pustules on my first patients ; but in my subsequent inoculations there were none."
For twenty large towns1 the acres of town area to one acre of park and the average annual death-rate per 1,000, for the ten years 1870-79, from small-pox, measles, scarlet fever, fever and whooping cough.
| Acres of Town area to one acre of park | Average annual death-rate per 1,000 living, for the ten years 1870-79. | |||||
| Smallpox | Measles | Scarlet Fever | Fever | Whooping Cough | ||
| Bristol | 10 | .21 | .45 | .99 | .50 | .54 |
| Liverpool | 10 | .58 | .76 | 1.35 | .95 | .88 |
| Brighton | 22 | .13 | .29 | .47 | .26 | .49 |
| London | 23 | .48 | .52 | .71 | .42 | .79 |
| Leicester | 32 | .33 | .38 | .84 | .48 | .49 |
| Bradford | 34 | .09 | .46 | 1.12 | .65 | .58 |
| Manchester | 34 | .19 | .57 | 1.02 | .69 | .88 |
| Birmingham | 38 | .37 | .42 | 1.15 | .48 | .84 |
| Leeds | 47 | .18 | .48 | 1.11 | .73 | .65 |
| Plymouth | 63 | .39 | .71 | .32 | .49 | .73 |
| Nottingham | 66 | .40 | .30 | .65 | .69 | .34 |
| Salford | 74 | .55 | .81 | .97 | .68 | .86 |
| Oldham | 78 | 16 | .53 | 1.53 | .48 | .66 |
| Sunderland | 115 | .92 | .33 | 1.19 | .74 | .72 |
| Hull | 117 | .25 | .27 | .84 | .83 | .48 |
| Newcastle-on-Tyne | 153 | .65 | .30 | 1.19 | .67 | .55 |
| Sheffield | 249 | .42 | .40 | 1.50 | .85 | .66 |
| Portsmouth | 280 | .52 | .38 | .62 | .75 | .40 |
| Norwich | 1,067 | .70 | .26 | .55 | .52 | .57 |
| Wolverhampton (no parks) | .68 | .31 | .93 | .56 | .60 | |
This table indicates generally, that towns with the greatest amount of park space have low small-pox death-rates, and vice versa. Liverpool appears to be an exception, but it will be noticed that in this town the rates for the other zymotic diseases are also very high, due to overcrowding and sanitary neglect. It must be
1 Fortieth and Forty-second Annual Reports of the Registrar-General.
SALUTARY EFFECT OF OPEN SPACES.
remembered, that with regard to air supply, small towns would have the advantage of large ones. A single dwelling would be surrounded on all sides with air; but suppose we have a group of houses of equal sizes arranged symmetrically in the form of a square, with five houses to a side, there will be sixteen outside houses with twenty-five altogether, and the fraction 16/25 will represent the external aerial supply ; with one hundred houses to a side, this will be shown by the smaller fraction 396/10,000; and hence the difference in the external ventilation of the two groups of houses would be very large, being represented by the difference between the two fractions 6,400/10,000 and 396/10,000. Thus, independently of park space, a small town would have better external ventilation for its houses than a large one; this may to some extent explain several exceptions in the table.
It may be, that there are other causes than the amount of park space to account for the difference in the small-pox mortality in the several towns specified, but the figures, in comparison with those of the other zymotic diseases, appear to be so striking as to suggest that external ventilation really exercises an important influence on the prevalence and mortality of this disease.
The epidemic of 1871-72, which largely dominates the small-pox figures in the last table, was conspicuously severe in the mining districts, which, as a rule, are most overcrowded. Durham was one of the most devastated counties, eleven of the thirteen registration districts having enormous small-pox death-rates.
| Registration districts | Population in 1871 | Deaths from small-pox in the 1871-72 epidemic.1 | Smallpox death-rate per million |
| Darlington | 40,812 | 152 | 3,724 |
| Stockton | 99,705 | 432 | 4,333 |
| Hartlepool | 39,970 | 175 | 4,378 |
| Auckland | 69,159 | 536 | 7,750 |
| Durham | 91,978 | 835 | 9,078 |
| Easington | 33,694 | 293 | 8,696 |
| Houghton-le-Spring. | 26,171 | 193 | 7,375 |
| Chester-le-Street | 33,300 | 209 | 6,276 |
| Sunderland | 112,643 | 1,011 | 8,975 |
| South Shields | 74,949 | 744 | 9,927 |
| Gateshead | 80,271 | 514 | 6,403 |
Dudley, in Staffordshire, had a small-pox death-rate of 8,977, Newcastle one of 6,456, and Bedwellty, Pontypridd, Merthyr, Swansea, Abergavenny, rates of 8,520, 7,492, 6,380, 5,627, and 4,768 per million respectively. Thus we see that small-pox picks out its victims from thickly-populated centres, and more especially towns which are imperfectly aerated, and where, as in mining districts, the industrial conditions predispose to overcrowding.
That our ancestors had a less plentiful supply of fresh air in and around their houses goes without saying. It is a well-known fact that our towns have increased in area quite out of proportion to the increase in the population. Mr. John Timbs2 observes, that the majority of the London squares were the growth of the last century, and that few of those in the western district existed before 1770, their sites being then mostly sheep-walks,
1 The epidemic was not limited to the years 1871 and 1872, in some cases it extended over several years.
2 " Curiosities of London," pp. 746, 747. John Timbs, F.S. A. 1867.
INCREASE OF METROPOLITAN AIR-SPACES.
paddocks, and kitchen - gardens; but we know that several of the London squares existed in the seventeenth century, and there is a reference to Bloomsbury Square in " Evelyn's Diary," under the date February 9, 1665 :—
" Dined at my Lord Treasurer's, the Earle of Southampton, in Blomesbury, where he was building a noble square or piazza, a little towne ; his owne house stands too low, some noble roomes, a pretty cedar chapell, a naked garden to the north, but good aire."
At the beginning of the eighteenth century Grosvenor, Cavendish, and Hanover Squares were laid out, the last two about the year 1718. Portman, Manchester, Finsbury, and Fitzroy Squares were constructed at the end of the last century; and at the beginning of the present century, about 1804, Russell Square, one of the largest in London, was finished, and about this time, also, Bedford and Euston Squares were opened. In 1829 a variety of important improvements were made immediately around St. Martin's Church; a whole labyrinth of close courts and small alleys were swept away, a district including places known as the Bermudas, the Caribbee and Cribbe Islands, and Porridge Island, notorious for its cook-shops;1 this wholesome and wholesale clearance prepared the site for the construction of Trafalgar Square. Other squares, such as Lowndes and Woburn Squares, were made about 1836; while Blandford, Harewood, and Dorset Squares are of more recent construction.
1 See Cassell's " Old and New London," vol. iii., p. 141.
Besides a deficient aeration of towns, our ancestors suffered under an insanitary tax upon light and air, known as the window-tax. This was imposed in order to make good the deficiencies of the clipped money. Its origin, in 1695, has been described by Lord Macaulay:—"It was a maxim received among financiers that no security which the government could offer was so good as the old hearth-money had been. That tax, odious as it was to the great majority of those who paid it, was remembered with regret at the Treasury and in the City. It occurred to the Chancellor of the Exchequer that it might be possible to devise an impost on houses, which might be not less productive nor less certain than the hearth-money, but which might press less heavily on the poor, and might be collected by a less vexatious process. The number of hearths in a house could not be ascertained without domiciliary visits. The windows a collector might count without passing the threshold. Montague proposed that the inhabitants of cottages, who had been cruelly harassed by the chimney men, should be altogether exempted from the new duty. His plan was approved by the Committee of Ways and Means, and was sanctioned by the House without a division. Such was the origin of the window-tax, a tax which, though doubtless a great evil, must be considered as a blessing when compared with the curse from which it rescued the nation."1
1 "History of England," vol. iv., p. 641. Macaulay.
The tax first fell largely on the landlord, but by the 20th of George II. (1746) it was levied upon the several windows of a house at so much per window, and consequently fell more cruelly upon the tenants of the tenement houses. By the 21st of George II., cap. 10, all skylights, the lights of staircases, garrets, cellars, and passages, were to count for the purpose of the tax ; and it was further enacted (11th section) that "no window or light shall be deemed to be stopped up unless such window or light shall be stopped up effectually with stone or brick, or plaister upon lath, etc." The law was enforced by a corrupt machinery of commissioners, receivers-general, and collectors, who were paid by results, and thus could hardly fail to act injuriously. In 1803 the law was altered, the houses being rated as a whole according to the number of their windows, and at the same time the tax for tenement houses was made recoverable from the landlord ; it thus became a sort of modern house-tax rated on windows.1
The great speculative builder of the Restoration was Nicholas Barbone, and his method of procedure may be inferred from the following:—" He was the inventor of this new method of building by casting of ground into streets and small houses, and to augment their number with as little front as possible, and selling the ground to workmen by so much per foot front, and what he could not sell, built himself. This has made ground rents high for the sake of mortgaging; and others, following his steps, have refined and improved upon it, and made a superfoetation of houses about London." 2
1 For the above description of the window-tax, I am indebted to Dr. Creighton's " History of Epidemics."
2 Quoted by Dr. Creighton from "Lives of the Norths." "A History of Epidemics in Britain," vol. ii., p. 86.
" In these mazes of alleys, courts or rents,'" Dr. Creighton says, "the people were, for the most part, closely packed. Overcrowding had been the rule since the Elizabethan proclamation of 1580, and it seems to have become worse under the Stuarts. On February 24, 1623, certain householders of Chancery Lane were indicted at the Middlesex Sessions for sub-letting, 'to the great danger of infectious disease, with plague and other diseases.' In May, 1637, one house was found to contain eleven married couples and fifteen single persons; another house harboured eighteen lodgers. In the most crowded parishes the houses had no sufficient curtilage, standing as they did in alleys and courts. When we begin to have some sanitary information long after, it appears that their vaults, or privies, were indoors, at the foot of the common stair. In 1710, Swift's lodging in Bury Street, St. James's, for which he paid eight shillings a week, had a 'thousand stinks in it,' so that he left it after three months. The House of Commons appears to have been ill-reputed for smells, which were specially remembered in connection with the hot summer of the great fever-year, 1685."
In the days of the Tudors and the Stuarts, the personal habits even of the upper classes left much to be desired. Fresh linen being a luxury, the clothes were seldom changed, and the dyer was more often in requisition than the laundress. Sir John Falstaff thus describes the contents of the buck or linen-basket:— " Foul shirts and smocks, socks, foul stockings, and greasy napkins ; that, Master Brook, there was the rankest compound of villainous smell that ever offended nostril."1
1 " The Merry Wives of Windsor," act iii., scene v.
DOMESTIC INSANITARY CONDITIONS.
From a washing tally found behind some oak panelling in the old chaplain's room at Haddon Hall, in Derbyshire, it would appear that towels had not always belonged to the domestic arrangements of this establishment, for in place of that word, which was scratched out, "laced bands " had been written on the horn of the tally.
Some interesting relics called "scratch-backs" have come down to us, the name sufficiently indicating the habits of the aristocracy of the time. A scratch-back is a hand or claw set in a long handle, which was sometimes made of silver elegantly chased, and there is one instance where a ring on the finger of the hand is set with brilliants. At one time these implements were as indispensable to a lady of fashion as her fan or her patch-box. They were kept in her toilet, and carried with her even to her box at the play. They belong to a period when personal cleanliness was not considered essential, when the style of dress worn was anything but conducive to comfort and ease, and when ladies wore immensely high head-dresses, which, when once fixed, were frequently not disturbed or altered for a month, and not until they had become almost intolerable to the wearer and to her friends.
In the sixteenth and seventeenth centuries, the state of the public health in London was at a very low ebb. The town ditch was a receptacle for all kinds of rubbish and decomposing organic matter ; the streets were unpaved and saturated with slops and other filth. Instead of regular highways, the out-parishes were reached by a maze of narrow passages and alleys. The dwellings of the poor were as bad as they well could be ; the houses projected over the roadway, which was so narrow that they almost met at the top ; there was no attempt at ventilation, and up to and even beyond the time of Queen Elizabeth, the floors were strewn with rushes, and, if we may trust to an epistle from Erasmus to his friend Dr. Francis, physician to Cardinal Wolsey, it would appear that these were seldom thoroughly changed, and, the habits of the people being uncleanly, the smell soon became intolerable. He speaks of the lowest layer of rushes (the top only being renewed) as sometimes remaining unchanged for twenty years, a receptacle for beer, grease, fragments of victuals, excremental and other organic matter. To this filthiness, Erasmus (one of the most acute observers) ascribed the frequent pestilences with which the people were afflicted.
Even as late as the beginning of the present century thing's were very different to what they are now. Thus, Willan, writing of fever, says :—
"Among the poor the mortality from this cause (contagious malignant fever) was nearly one in four of all persons affected, notwithstanding the attentive administration of proper articles of diet, and of suitable remedies, with plenty of wine.
" The good effects of all these applications are almost wholly superseded by the miserable accommodations of the poor with respect to bedding, and by a total neglect of ventilation in their narrow, crowded dwellings. It will scarcely appear credible, though it is precisely true, that persons of the lowest class do not put clean sheets on their beds three times a year ; that, even where no sheets are used, they never wash or scour their blankets and coverlets, nor renew them till they are no longer tenable ; that curtains, if unfortunately there should be any, are never cleaned, but suffered to continue in the same state till they drop to pieces ; lastly, that from three to eight individuals, of different ages, often sleep in the same bed ; there being, in general, but one room, and one bed for each family. To the above circumstances may be added, that the room occupied is either a deep cellar, almost inaccessible to the light, and admitting of no change of air; or a garret, with a low roof and small windows, the passage to which is close, kept dark in order to lessen the window-tax, and filled not only with bad air, but with putrid, excremental, or other abominable effluvia from a vault at the bottom of the staircase. Washing of linen, or some other disagreeable business, is carried on while infants are left dozing, and children more advanced kept at play whole days on the tainted bed ; some unsavoury victuals are from time to time cooked. In many instances idleness, in others the cumbrous furniture or utensils of trade with which the apartments are clogged, prevent the salutary operation of the broom and whitewashing brush, and favour the accumulation of a heterogeneous, fermenting filth. The rooms do not change their condition till they change their tenants. Often, indeed, so little care is taken that enough of the old leaven remains to infect all the inmates who successively occupy the same premises. I recollect a house in Wood's Close, Clerkenwell, wherein the fomites of fever were thus preserved for a series of years ; at length a friendly fire effectually cleared away the nuisance. A house notorious for dirt and infection, near Clare Market, afforded a further proof of negligence ; it was obstinately tenanted till the walls and floor giving way in the night crushed to death the miserable inhabitants. From all these causes combined there is necessarily produced a complication of fetor, to describe which would be as vain an attempt as for those to conceive who have been always accustomed to neat and comfortable dwellings.
" The above account is not exaggerated. For the truth of it I appeal to the medical practitioners, whose situation, or humanity, has led them to be acquainted with the wretched inhabitants of some streets in St. Giles's parish, of the courts and alleys adjoining Liquor-pond Street, Hog Island, Turnmill Street, Saffron Hill, Old Street, Whitecross Street, Grub Street, Golden Lane, the two Brick Lanes, Rosemary Lane, Petticoat Lane, Lower East Smithfield, some parts of Upper Westminster, and several streets of Southwark, Rotherhithe, etc.
" It cannot be wondered at, that in such situations contagious diseases should be formed, and attain their highest degree of virulence. The inhabitants of the second storey in houses occupied by the poor are usually better accommodated, and therefore experience, during sickness of any kind, the best effect from public and private charities. But persons thus stationed suffer from contiguity, and from their friendly attentions to those above them, or to the tenants of the cellars ; so that in whatever part of the house a fever commences, it is soon diffused among all the inmates and their occasional visitors, especially in seasons which favour its progress like the last autumn and winter. ... It is a melancholy consideration that in London and its vicinity hundreds, perhaps thousands of labourers, heads of families, and in the prime of life, are thus consigned to perish annually, being often so situated that medical applications or cordial diet cannot in any wise alleviate their distress."1
The sanitary condition of the prisons in the last century, as discovered by the great prison reformer, John Howard, gives some indication of the ignorance that prevailed in regard to the public health at that time. In the Introduction to his book,2 he tells us that in his inspection of gaols, he noticed a complication of distress, but his attention was principally arrested by the gaol fever and the small-pox, which he saw prevailing to the "destruction of multitudes," not only of felons in their dungeons, but of debtors also. On page 8, in describing the air in prisons, he says :—
" My reader will judge of its malignity, when I assure him that my clothes were in my first journeys so offensive, that in a post-chaise, I could not bear the windows drawn up, and was therefore often obliged to travel on horseback. The leaves of my memorandum book were often so tainted, that I could not use it till after spreading it an hour or two before the fire ; and even my antidote, a vial of vinegar, has, after using it in a few prisons, become intolerably disagreeable. I did not wonder that in those journeys many gaolers made excuses, and did not go with me into the felons' wards.
" From hence anyone may judge of the probability there is against the health and life of prisoners, crowded in close rooms, cells, and subterranean dungeons, for fourteen or sixteen hours out of the four-and-twenty. In some of those caverns the floor is very damp ; in others there is sometimes an inch or two of water, and the straw, or bedding, is laid on such floors, seldom on barrack bedsteads. Where prisoners are not kept in underground cells, they are often confined to their rooms, because there is no court belonging to the prison, which is the case in most city and town gaols."1 Dr. Willan's "Observations on Diseases in London." Medical and Physical Journal, vol. iii., pp. 298-300. (April, 1800.)
2 " The State of the Prisons in England and Wales." Second Edition.1780. John Howard, F.R.S.
There was much overcrowding. On page 21 we read :—
"Debtors crowd the gaols (especially those in London) with their wives and children. There are often by this means ten or twelve people in a middle-sized room, increasing the danger of infection."
John Howard observes the effect of the window tax (p. 9):—
"One cause why the rooms in some prisons are so close, is perhaps the window tax, which the gaolers have to pay; this tempts them to stop the windows, and stifle their prisoners."
Concerning the water supply and drainage, we read (pp. 8,9):—"
Many prisons have no water. This defect is frequent in bridewells and town gaols. In the felons' courts of some county gaols there is no water ; in some places where there is water, prisoners are always locked up within doors, and have no more than the keeper or his servants think fit to bring them. In one place they were limited to three pints a-day each—a scanty provision for drink and cleanliness! . . . Some gaols have no sewers, and in those that have, if they be not properly attended to, they are, even to a visitant, offensive beyond expression. How noxious, then, to people constantly confined in those prisons!" Under these conditions, is it to be wondered at, that typhus and small-pox prevailed to the "destruction of multitudes "?
Howard's attention was arrested by the insanitary state of the prisons, but it is doubtful whether the poor, especially in the large towns, lived in a much healthier atmosphere than the prisoners. Dr. William Buchan, in his work on "Domestic Medicine," says:
"Whenever air stagnates long, it becomes unwholesome. Hence the unhappy persons confined in jails not only contract malignant fevers themselves, but often communicate them to others. Nor are many of the holes, for we cannot call them houses, possessed by the poor in great towns much better than jails. These low, dirty habitations, arc the very lurking-places of bad air and contagious diseases. Such as live in them seldom enjoy good health, and their children commonly die young."1
Thus, Dr. Buchan connects the high mortality of children in the last century with overcrowding and filth. From these facts we may infer, that sanitary reform would tend to alter the age-incidence of zymotic disease. This has been fully recognised by the Regrstrar-General in the following notable words :
" That the sanitary efforts made of late years should have more distinctly affected the mortality of the young is only what might be naturally anticipated; for it is against noxious influences to which the young are more especially sensitive that the weapons of sanitary reformers have been chiefly directed."2
1. "Domestic Medicine," p. 86. Tenth edition. 178S. William Buchan, M.D.
2. Forty-second Annual Report of the Registrar-General, p. xxiii. 1879.
There is no reason to believe that small-pox is any exception to this general law, and in this connection the following table quoted by Dr. Collins and Mr. Picton is not without interest.1
|
Fatal small-pox in Scotland, 1871 |
|||
| Smallpox deaths at all ages | Smallpox deaths under 5 years of age | Percentage under 5 years of age | |
|
Principal towns (population above 25,000) |
886 |
195 |
22.0 |
|
Large towns (population from 10,000 to 25,000) |
143 |
32 |
22.3 |
| Small towns (population from 2,000 to 10,000). | 209 | 55 | 26.3 |
|
Mainland rural districts |
183 |
0 |
13.6 |
|
Insular rural districts |
11 |
|
0.0 |
The larger proportionate small-pox mortality of children in the towns, compared with rural and insular districts is certainly not due to any difference in the amount of vaccination, and it is difficult to resist the conclusion that the young are more injuriously affected by overcrowding and other insanitary conditions associated with town life than adults.2
1 Royal Commission on Vaccination, Dissentient Commissioners' Statement, section 148.
2 See Paper read by Mr. Alfred Milnes before the Statistical Society, June 15, 1897.
While discussing the subject of sanitation, it is necessary also to allude to the influence of burial grounds on mortality. In the last century it was usual to establish these in the midst of populous towns, and there can be no question, that the constant inhalation of effluvia from dead bodies, had a deleterious effect on the living.
Buchan observes (p. 85):
"Certain it is, that thousands of putrid carcases, so near the surface of the earth, in a place where the air is confined, cannot fail to taint it; and that such air, when breathed into the lungs, must occasion diseases."
With the growth of sanitary institutions, reforms have been made with regard to the disposal of the dead, and, in nearly all urban districts, the dead are now buried in outlying cemeteries. The next generation will no doubt witness a great extension of the still more sanitary practice of cremation, already introduced in London, Glasgow, Manchester, Liverpool, and other places.
Besides insanitation, other causes have probably had their effect on the small-pox mortality.
A number of typhus and small-pox epidemics have been intimately associated with periods of scarcity and want. The winter of 1683-84 was very severe. This was followed by a long drought in the summer of 1684, and another severe winter in 1684-85, and not until the spring of 1685 was there plentiful rain.1 In 1685-86 the country was visited by a terrible epidemic of fever, and in 1685 small-pox was above the average, with 2,496 deaths in London, or a rate of 107 per 1,000 deaths from all causes. The winter of 1708-09 was excessively severe, frost lasting all over Europe from October to March. This was followed by a bad crop of cereals in 1709, the price of wheat per quarter running up from 27s. 3d. on Lady-day, 1708, to 81s. 9d. on Lady-day, 1710.2 In 1710,the proportion of small-pox deaths was 127 per 1,000 deaths from all causes (3,138 small-pox deaths). 2,810 died from small-pox in 1714, or a rate of 106 per 1,000 from all causes. This followed a rise in the price of wheat.
1 "A History of Epidemics in Britain," vol ii., p. 23. Creighton.
2 Ibid., pp. 54, 55.
In 1718 the harvest was a bad one; and about this time there was scarcity of employment amongst the weavers in the east end of London ;1 during the year 1719, there were 3,229 deaths from small-pox in London, or a rate of 114 per 1,000 from all causes. Up to the month of February, 1756, the season had been a forward one, but the early promise of spring was blighted by cold. This was succeeded by a wet summer and autumn ; the fruit crop was ruined, and the corn harvest spoilt by long, heavy rains ; dearth and bread riots followed.2 In 1757, the proportion of small-pox deaths rose to 155 per 1,000 from all causes (3,296 small-pox deaths).
A bad harvest in 1794 raised the price of wheat to 55s. (January 1,1795); by August, 1795, it rose to 108s., falling in October to 76s., owing to the action of the Government, in order to avert famine, causing neutral ships —bound to French ports with corn—to be seized and brought to English ports. In the spring of 1796, the acme of distress was reached, wheat being sold for 100s. per quarter.3 Mr. Pitt admitted in Parliament that the condition of the poor "was cruel, and such as could not be wished on any principle of humanity or policy ;"4 in this year, the mortality figures showed the largest number of small-pox deaths of any year within the London Bills, being 3,548, or 184 per 1,000 deaths from all causes.
1 "A History of Epidemics in Britain," vol. ii., pp. 62, 64. Creighton.
2 Ibid., p. 125.
3. Ibid., pp. 158, 159.
4 Eighth Annual Report of the Registrar-General, p. 12.
The harvest in 1816 proved deficient in quantity, and inferior in quality. Prices rose from 66s. a quarter in 1815, to 78s. in 1816, and 98s. in 1817.1 This was succeeded by epidemics of small-pox, relapsing fever, and typhus in 1817-19.
From the Registrar-General's eighth annual report we learn that the year 1837 was one of great commercial depression. In referring to joint stock banks, Major Graham says :—
" Many of the companies were got up by speculators, for the sole purpose of selling shares. The signal of collapse was given by the failure of the Agricultural Bank of Ireland in November, 1836. The Bank of England assisted the Manchester Northern and Central Bank in December, the large American houses in February and March, 1837. It was in vain. Commercial credit fell to its lowest point of depression in the first half of the year 1837."2 Again—"In 1837 the price of bread rose rapidly, while trade was depressed, and speculation sat exhausted in the midst of ruin."3
During the several years commencing in 1837, one of the most disastrous small-pox epidemics of the nineteenth century occurred, and also a very severe epidemic of typhus.
1 Eighth Annual Report of the Registrar-General, p. 16.
2. Ibid., p. 23.
3 Ibid., p. 24.
Another cause of the diffusion of small-pox, as well as of typhus and dysentery, is probably war. Dr. Guy writes :—
" War is a special cause of that more general condition of overcrowding, so destructive to health, so productive of disease. It consists in bringing one crowd of trained, armed, and disciplined men into collision with another, under circumstances highly unfavourable to health. It reaches its climax in civil war, in prolonged siege operations, and when armies are quartered among civil populations."1
The shock of battle also, with its attendant anxiety and the high tension of the organism, are important and undeniable factors in the production of epidemic diseases.
Mr. Alexander Wheeler pointed out before the Royal Vaccination Commission (Q. 7,994) that during almost the whole of the last century Europe was one huge battle-ground, and wars continued on and off until the year 1815. The fact, that small-pox was declining during the opening years of the present century, does not exclude war as one of the causes of this disease.
As to the effects of war. In a work by Mr. William F. Fox, entitled "The Losses of the American Civil War," we read:—
"110,070 were killed, 249,458 died of other causes, making 359,528 in all in the Northern army."
In speaking of the 249,458 who died from disease, Mr. Fox says :
" One-fourth died from fever, principally typhoid ; one-fourth from diarrhoea or other forms of bowel complaint; one-fourth from influenza and lung complaints ; and one-fourth from small-pox, measles, brain diseases, erysipelas, and various other forms of disease common to the masses."2
With regard to the Franco-Prussian war, Mr. Wheeler, in his evidence before the Royal Commission, quoted some of the commissioners sent to Eastern France to aid the peasantry. One of these, Dr. Robert Spence Watson, has published his experiences,3 from which the following have been extracted. I may state that in 1870 there was not more small-pox than usual until the later months of the year. Its increase was at the time of the terrible slaughter following the invasion of France.
1 Journal of the Statistical Society, December, 1882, p. 579.
2 Third Report, Royal Commission on Vaccination, Q. 8056.
3 "The Villages Around Metz." Newcastle-on-Tyne. 1870."November 6, 1870. Then I went to Lessy and Chatel St. Germain, hearing everywhere the same state of distress. All the crops gone, all the winter's firewood gone, many houses destroyed, and numbers needing help in every village. . . . When the mare's hoofs sunk deep, she knocked up bits of flesh, and the stench was so sickening that 1 should have fainted but for my smelling salts. It was a strange and sad sight; sometimes twenty-five heaps of graves within sight at once. These graves are in a bad state, many of them were too shallow to begin with. The heavy rains have caused them to sink in, and they are covered with an inch or more of black, oily water, which has, when disturbed, a most disgusting stench" (pp. 22, 23).
" November 7th. All men and officers alike speak of the terrible loss of blood. At Rezonville, and in its neighbourhood, the people say 18,000 Germans are buried. This I doubt, but the number must be enormous" (p. 25).
" November 9th. Metz was literally crammed with soldiers. The Germans—strong, hearty, conscious of victory ; the French—cowed, worn, starved, and miserable. ... In one place there were fifteen long streets of railway vans, filled with typhus patients ; in another as many streets of canvas tents, also filled with sick. I visited these places, and found them in the filthiest state ; but the Germans had begun to put them into order. At first, you might see soldiers, in full small-pox, walking about the streets, but this was soon forbidden " (p. 28).
Dr. Watson concluded his last letter with the observation that
" unless England puts forth her hand liberally and wisely, the coming winter must see in that beautiful and fertile land an amount of misery, famine, and plague which it is too dreadful to contemplate " (p. 36).
Another commissioner has kindly furnished me with the following statement:—
" Mr. William Jones, of Sunderland, was one of those who went out on behalf of the Society of Friends to relieve the sufferings of the people. He was present at Metz when Marshal Bazaine's army surrendered. The main body were encamped outside the walls of Metz, on low ground near the Moselle, the wetness of the season having converted the camping-ground into a morass. In some places the impress of the men's bodies was left as a cast in the mud in which they had lain. Their clothes and their blanket were saturated with mud. Their food for weeks had only been a biscuit and a bit of horseflesh without salt. Dysentery was universal, and typhus and smallpox raged. Over a wide area around the camp the carcases of dead horses were left to rot and contaminate the air. On the 29th of October, 1870, Mr. Jones and his companion, Mr. Allen, were permitted to enter the city, which had opened its gates to admit the German army, which marched through in triumph. The narrow streets were crowded with French soldiers disarmed, and looking diseased and hunger-bitten. Numbers of them were going about the streets with confluent small-pox fully out over their faces. Black typhus raged in the hospitals. Ultimately the worst cases were removed into 320 railway vans drawn up in the 'Grande Place.' No one was allowed to pass the German sentries into the square, but the constant cry of the wretched sufferers for water was distinctly heard by Mr. Jones outside the square in which they were isolated. It was stated that all these black typhus patients perished, and were buried in huge trenches outside the walls of the city.
" Mr. Jones's companion, Mr. Allen, who was vaccinated, and, he believes, re-vaccinated, took the small-pox, and his own sister, who came over to nurse him, caught the disease from him and died there, and was buried in the cemetery at Plantieres outside the walls of Metz.
" N.B.—Mr. John Bellows, of Gloucester, who followed Mr. Jones to Metz, states in his pamphlet, 'The Track of the War round Metz,' that, of the twelve commissioners of the Society of Friends who were present in Metz, eight were at one time ill, five being down with small-pox, and one (Miss Allen) died of small-pox."
MALTHUS DISCOVERS A NEW PRINCIPLE.
There is, indeed, some reason to believe that this war was the starting point of the great European pandemic of small-pox in 1871-72.
Another cause of the decline in small-pox during the present century, especially among children, remains to be told. Malthus, in 1803, wrote :—
" For my own part, I feel not the slightest doubt, that, if the introduction of the cow-pox should extirpate the small-pox, and yet the number of marriages continue the same, we shall find a very perceptible difference in the increased mortality of some other diseases."1
1 "An Essay on the Principle of Population," p. 522. T. R. Malthus. London. 1803.
Malthus, thus early, clearly saw that even if cow-pox had possessed all the virtues that were claimed for it, the reduction in the mortality from one zymotic disease would, other things being equal, have no appreciable effect on the death-rate.
This principle was first worked out experimentally by Dr. Robert Watt, lecturer on the theory and practice of medicine at Glasgow. He examined the Glasgow burial registers over a space of thirty years, from 1783-1812, and divided the thirty years into five periods of six years each. The following table gives his figures for small-pox, measles, and whooping-cough, as percentages of the deaths from all causes :—1
|
|
Of the total deaths The percentage |
||||
|
Periods |
Total deaths from all causes |
Under 10 years of age |
From smallpox |
From measles |
From whooping cough |
|
1783-88 |
9,994 |
53.48 |
19.55 |
0.93 |
4.51 |
|
1789-94 |
11,103 |
58.07 |
18.22 |
1.17 |
5.13 |
|
1795-1800 |
9,991 |
54.48 |
18.70 |
2.10 |
5.36 |
|
1801-06 |
10,034 |
52.03 |
8.90 |
3.92 |
6.12 |
|
1807-12 |
13,354 |
55.69 |
3.90 |
10.76 |
5.57 |
These statistics proved that while small-pox had diminished, measles and to a lesser extent whooping-cough had increased, so that a child had no better chance of reaching its tenth year in the last period2 than in the first. Dr. Watt was somewhat staggered at the result.
1 An Inquiry into the Relative Mortality of the Principal Diseases of Children, and the numbers who have died under ten years of age, in Glasgow, during the last thirty years (p. 49). Robert Watt, M.D. 1813.
2 Dr. Watt remarks that in Glasgow during the last period (from 1807-12) vaccination may be said to have been pretty fully established, "perhaps, as much so, as in any other city in the Empire."
THE ZYMOTIC DISEASES REPLACE EACH OTHER.
He says (p. 6):—
"Taking an average of several years, I found that more than a half of the human species died before they were ten years of age, and that of this half more than a third died of the small-pox, so that nearly a fifth part of all that were born alive perished by this dreadful malady. I began to reflect how different the case must be now! In eight years little more than 600 had died of the small-pox ; whereas, in 1784, the deaths by that disease alone amounted to 425, and in 1791 to 607, which, on both occasions, exceeded the fourth of the whole deaths in the year.
" To ascertain the real amount of this saving of infantile life, I turned up one of the later years, and by accident that of 1808, when, to my utter astonishment, I found that still a half or more than a half perished before the tenth year of their age! I could hardly believe the testimony of my senses, and therefore began to turn up other years, when I found that in all of them the proportion was less than in 1808 ; but still, on taking an average of several years, it amounted to nearly the same thing as at any former period during the last thirty years."
Dr. Farr was a firm believer in Watt. He writes :—
"The zymotic diseases replace each other; and when one is rooted out it is apt to be replaced by others, which ravage the human race indifferently wherever the conditions of healthy life are wanting. They have this property in common with weeds and other forms of life : as one species recedes, another advances. By improving the hygienic conditions in which men live, you fortify them against infection ; and further, by isolating the infected, the chances of attack are diminished." 1
1 Thirty-fifth Annual Report of the Registrar-General, p. 224.
In this chapter, I have attempted to deal with some of the principal causes of the diminution of small-pox. Firstly, I have shown that a part of the decline, and especially that part which has taken place in children, is not necessarily a saving of life, but only a shifting of the mortality on to some other disease, such as measles or whooping-cough, which happens for the time being to be more predominant.
The residue of the diminution is a real gain, and is probably due partly to the displacement of small-pox inoculation by a non-infectious malady; and to this extent was vaccination an advantage as compared with the old variolous inoculation. Other causes have been due to the more abundant air supply in and around houses ; the greater cleanliness of the people in their persons, their houses, and their towns ; and last, but not least, the greater material prosperity and freedom from war, which has been the lot of those who have been fortunate enough to be born into the present century.
CHAPTER 4.
THE INCIDENCE OF SMALL-POX ON VACCINATED AND
UNVACCINATED COMMUNITIES.
The experience of Leicester has proved conclusively that small-pox
can be kept from spreading in un-vaccinated districts. In 1872, Leicester was a
well-vaccinated town, and had an epidemic of small-pox, with 346 deaths
registered from the disease. This failure to protect led to a revolt against the
practice. The default commenced after 1874, and since 1885 the percentages of
vaccinations to births have been as follows :—l
Years Births
Primary Percentage of vaccina-
te3™- Birtns.
vaccinations. tions to births.
1885 ... 4,682 ... 1,842 ... 39-3
1886 ... 4,858 ... 1,122 ... 23-1
1887 ... 4,689 ... 474 ... io'i
1888 ... 4,787 ... 314 ... 6-6
1889 ... 4,789 ... 172 ... 3-6
1890 ... 4,699 ... 131 ... 2-8
1891 ... 4,790 ... 92
... 1-9
1892 ... 5,816 ... 133 ... 2-3
1893 ... 6,006 ... 249 ... 4-1
1894 ... 5,995 ... 133 ... 2-2
1895 ... 5,962 ... 75 ... 1-3
As far as the children are concerned, therefore, Leicester is
practically unvaccinated. Let us see what
1 Report of the Medical Officer of Health for the year 1895, pp. 31, 38.
law, says:—
" I made a point of enquiring during my stay there, in August last, as to what had been the subsequent course of affairs. I learned on the very best authority that the objections of the French Catholics had been completely overcome. . . . Vaccination being now (1883) as well carried out in Montreal by its officers of health as in the other great cities of the Dominion, smallpox has become almost entirely extinct." 1
The causes of the epidemic in 1885 were not far to seek. Towards its close a member of the staff of the Montreal Herald interviewed Dr. Garceau,2 of Boston, a supporter of vaccination, but who was declared by the editor to be one of the best-informed sanitarians on the American continent. When asked to what cause he attributed the extent of the epidemic, Dr. Garceau replied—
" One cause is the fact that the people have not been properly vaccinated, but I attribute the chief cause to the frightful system of cesspits which prevails, and the insanitary condition of the place generally. It is unclean ; and unless some action is taken to clean the privy vaults and remove all garbage, the city will next season be in excellent shape for cholera, or any other equally contagious disease."
The Secretary of the Citizens' Committee (Mr. Michaels) appointed to enquire Into the epidemic, said—
"The streets and lanes are in a disgraceful condition. Not only in the distant portions of the city, but within the most aristocratic quarters mid in the heart of the commercial portion, the lanes, and even portions of the streets, are reeking with filth."
1 A letter to the Right Hon. Lyon Playfair, C.B., pp. 13, 14. 1883.
2. Vaccination Inquirer, vol. viii., p. 179. (February, 1887.)
MR. REDHEAD'S CASES.
proportion to the proximity of the vaccination; nor docs tht; incidence of
small-pox seem to be regulated in this manner, for the National Vaccine Board
says :— " It appears to us to be fairly established, that the disposition in
the vaccinated to be thus affected by the contagion of small-pox, does not
depend on the time that has elapsed after vaccination ; since some persons have
been so affected who had recently been vaccinated; whilst others, who had been
vaccinated eighteen and twenty years have been inoculated, and fairly exposed to
the same contagion with impunity."1 This evidence is, 1 venture to suggest, more
valuable than present-day experience, for these theories of prevention and
mitigation had not then obtained the same hold on the medical mind.
Mr. Redhead also gives several instances of small-pox being taken by means of
inoculation after vaccination. One of these, James Shepherd, was vaccinated at
fifteen months of age by Mr. T. Carter, and when a year and a half old, i.e.,
three months after vaccination, was inoculated with matter from Elizabeth James,
above-mentioned. Mr. Redhead notes that the patient was very feverish, the arm
much inflamed, but the pustules not very large.
Mr. Harrison, in referring to Mr. Redhead's cases, says (p. 10):—"We cannot but
feel our confidence in the preventive power of the cow-pox to be somewhat
shaken." He also relates three instances in one family; these excited
considerable interest among medical men, from one of them having been vaccinated
at a public institution in London by Jenner himself, who, after having inspected
the vaccination, pronounced the child secure from small-pox.
1 Report of the National Vaccine Establishment for 1819.
There is every reason to believe that about this time vaccination was rapidly
falling into disrepute. Thus, Jcnner's old friend, Gardner, writing to him from
Frampton, on May 21, 1817, says:—"From some unaccountable causes, the fame of
vaccination seems to decline in this part of the country : I find my offers of
gratuitous service very frequently rejected even by those whose former children
have undergone the operation."1
In the London Medical Repository for July, 1817, the editors, Dr. G. M. Burrows
and Mr. A. T. Thomson, in their observations on prevailing diseases, say: "
Variola, above all, continues and spreads a devastating contagion. However
painful, yet it is a duty we owe to the public and the profession to apprise
them, that th'e number of all ranks suffering under small-pox who have
previously undergone vaccination, by the most skilful practitioners, is at
present alarmingly great. This subject is so serious, and so deeply involves
the dearest interests of humanity, as well as those of the medical character,
that we shall not fail in directing our utmost attention to it."2
In the August number the editors remark: "Generally, the diseases of last month
partake of that nature usual to the season ; hence there is nothing but variola
particularly demanding notice. Smallpox, however, still forces itself upon our
observation. It has, we believe, been more prevalent than for many years past,
and has assumed a more than usually virulent character; many of the cases having
been of the confluent kind. This may in some degree account for so many, who
1 Baron's "Life of Tenner," vol. ii., p. 203. "London Medical Repository, vol.
viii., p. 95.
OFFICIAL EXCUSES FOR FAILURE. I43
had previously undergone vaccination, being infected by small-pox, as we
remarked in our last report; and we are concerned to find, from the increasing
testimonies of medical practitioners, that these instances have been much and
widley extended. So little modified has the disease in some cases appeared to
have been by the influence of the vaccine inoculations, that death has ensued ;
an effect which, as far as our information goes, was never before produced by
small-pnx, after the patient had been subject to the action of the vaccine
virus."1
Baron informs us that in 1818 "there was great clamour about the prevalence of
small-pox after vaccination," and that " the greatly exaggerated statements on
the subject of the vaccine failures, and the hesitating manner in which
respectable individuals spoke on the subject, threatened to lead to a
considerable abandonment of the practice."2
About this time we even find failures recorded by the National Vaccine
Establishment, coupled with ingenious but far-fetched explanations. Thus, in the
report of 1818, we read:—"Five cases have been reported to the Board, of
vaccinated persons who have subsequently died of small-pox. In one of these
cases, it was clearly ascertained, that the only vaccine vesicle which had been
excited, was disturbed and broken in its progress, which there is great reason
for believing has been a frequent cause of the insecurity of vaccination ; in
the other cases, no detail respecting the vaccination could be obtained, and
they were, moreover,
i- London Medical Repository, vol. viii., p. 183. 2 Baron's "Life of Jenner,"
vol. ii., pp. 237, 238.
all vaccinated at a period of time when the mode of vaccination, and the
management of the vesicle, were not well understood."
In the report of 1819 it is stated :—"The testimonies of some of our
correspondents in this country, are by no means so favourable. They concur in
showing, that great numbers of persons who had been vaccinated, have been
subsequently seized with a disease presenting all the essential characters of
small-pox ; but that in the great majority of such cases, the disease has been
of comparatively short duration, unattended by symptoms of danger. In several of
these cases, however, the malady has been prolonged to its ordinary period ; and
in eight reported cases it has proved fatal."
In the London Medical Repository^ for August, 1819, Mr. William Gaitskell,
surgeon of Rotherhithe, was " truly sorry to report two cases of malignant
smallpox subsequent to vaccination." The first, a stout young man, eighteen
years of age, contracted small-pox two years after vaccination, and died on the
twelfth day, a mass of putrefaction. The second, about twenty-two years old,
took small-pox of a very malignant description, twelve years after vaccination,
but recovered. Both patients were supposed to have gone through a regular
vaccination; they were pronounced safe (according to their own statement), and
presented distinct impressions of the disease on their arms.
In the Medical and Physical Journal*1 for July, 1820, Dr. Macleod, physician to
the Westminster General Dispensary, contributed a communication,
entitled,
^London Medical Repository, vol. xii., pp. 113, 114. 2 Medical atid Physical
Journal, vol. xliv., pp. I -12.
DR. MACLEOD'S EXPERIENCES. 145
" Remarks on the Small-pox, as it has occurred in London subsequent to
Vaccination." He gives the following cases (pp. 10-12) illustrating some of the
appearances assumed by small-pox after vaccination. (See next page.)
Dr. Macleod says (p. 6) :—" I have seen too many instances of small-pox in
children vaccinated in London, where that process was carried on in the way
which the National Vaccine Establishment has recommended as the most
efficacious, to retain much faith in its preventive powers, in whatever manner
conducted." Again he remarks (pp. 8,9):—"The history of vaccination altogether
forms a severe satire upon the mutability of medical doctrines. In the first
ardour of discovery, not contented with its blessings to mankind, its benefits
were also extended to the brute creation. It was to annihilate small-pox, prove
an antidote to the plague, to cure the rot in sheep, and preserve dogs from the
mange. These good-natured speculations, however, were soon abandoned ; and more
recently all had agreed in acknowledging its anti-variolous powers, which, we
were told, were as well established as anything human could be.
" But the present epidemic shows too clearly the mortifying fallibility of
medical opinions, though founded on the experience of twenty years, and
guaranteed by the concurring testimony of all the first physicians and surgeons
in the world."
In 1820 we have also further official admission of vaccine failures. " It is
true, indeed, my Lord, that we have received accounts from different parts of
the country, of numerous cases of small-pox having
At e
when
. t ,, !
Name. infected
Vaccination.
Nature of the small-pox.
Thomas Lucas - 5 Vaccinated when six months of age.
Smart fever, followed by copious pustular eruption
on face, neck, chest, and limbs.
Selina Duve 9 Vaccinated when seven years of age, at
Attacked with fever, headache, and delirium. Copi-
thejenneriau Institution in Holborn. ous pustular eruption on face,
chest, and extremities. Eruption particularly crowded on the face.
Henry Oldfield 7 Vaccinated at the Small-pox Hospital
Considerable fever, and pustular eruptions on the
when a few months old, had a perfect face, chest, and back, cicatrix on
the arm. Lucy Stillwell - 22 Vaccinated 14 years previous to
attack, Small-pox ushered in with considerable fever, but
and had a perfect cicatrix on the arm. the number of pocks was
inconsiderable.
William Pyihe - 8 Vaccinated at the Small-pox Hospital
Violent fever, headache, and delirium, accompanied
when a few months old, and had a by extreme restlessness and fits of
screaming. A
perfect cicatrix on the arm. copious pustular eruption appeared
on different
parts of the body. On the face the eruptions were confluent round the mouth and
under the eyes, and coherent in other parts. Many of the pocks on the forearms
were surrounded with a narrow purple areola, giving the appearance of pustules
arising from the centre of petechife. Several of the pocks were filled with a
purple fluid.
Robert Page - 21 month.1- Vaccinated, and supposed to have had The
disease ushered in with fever, and followed in
the disease in a satisfactory manner. several days by a rash resembling
measles. The
child continued restless and feverish, and vesicular eruptions, with central
depressions, appeared on the back. The vesicles were first of a pearly
appearance, and afterwards became more opaque. The constitutional symptoms did
not abate, and occasional convulsions supervened; these became more severe, and
the child died about the tenth day of the illness.
— Page - - 3 Vaccinated, and supposed to have had
Was affected in a similar manner to his brother, but
the disease in a satisfactory marmer^ldisease milder.
COW-POX KAILUKES KXTKNS1VK. I47
occurred after vaccination ; and we cannot doubt that I lie prejudices of the
people against this preventive expedient arc assignable (and not altogether
unreasonably perhaps) to this cause. These cases the Board has been
industriously employed in investigating ; and though it appears that many of
them rest only on hearsay evidence, and that others seem to have undergone the
vaccine process imperfectly, some years since, when it was less well understood,
and practised less skilfully than it ought to be, yet, after every reasonable
deduction, we are compelled to allow that too many still remain on undeniable
proof, to leave any doubt that the pretensions of vaccination to the merit of a
perfect and exclusive security in all cases against smallpox, were admitted at
first rather too unreservedly."1
It was the small-pox epidemic of 1817-19 which, however, demonstrated the
failure of vaccination on a large scale, for a majority of the cases were
admittedly " protected." Dr. John Thomson writes :—" It is to the severity of
this epidemic, I am convinced, that we ought to attribute the greatness of the
number of the vaccinated who have been attacked by it, and not to any
deterioration in the qualities of the cow-pock virus, or to any defects in the
manner in which it has been employed. Had a variolous constitution of the
atmosphere, similar to that which we have lately experienced, existed at the
time Dr. Jenner brought forward his discovery, it may be doubted whether it ever
could have obtained the confidence of the public."2
1 Report of the National Vaccine Establishment for 1820. - " Historical Sketch
of Small-pox," p. 394. John Thomson, M.D., F.R.S.E. London, 1822.
each case, were read. The account stated that in the last year twelve persons
had died of small-pox whose deaths were presumed to be subsequent to
vaccination. The Duke of York here interposed, and observed that the fact of the
cases having previously been vaccinated was distinctly stated in copy of the
report sent to him ; and the Home Secretary, Mr. Peel, who was also present,
said that, after reading his copy of the report, he became uneasy about his own
children, all of whom had been vaccinated.
Dr. Gregory, the physician to the hospital, stated that the copies alluded to by
his Royal Highness had been sent before they had been finally settled by him. He
wished to add notes, but finding that the copies had been made, and that the
words could not be introduced without the making of fresh copies, he did not
think the omission of any great consequence, and therefore he let them go as
they were. He regretted he had not inscribed the word ''presumed" but one
reason was that it was not a term generally used by the profession.
It is fairly evident what Dr. Gregory thought of the cases. They were, however,
the subject of inquiry by the National Vaccine Establishment,1 and, as we might
have expected, the result was so satisfactory " as to leave no cause to doubt
that these individuals had not been properly vaccinated."
From this time onwards medical criticism became less acute, but neither then nor
at any other time has it subsided, and there was a strong undercurrent of
scepticism amongst able and trustworthy observers at
1 Baron's " Life of Jenner," vol. i., pp. 273, 274.
UNM1TU1ATKI) BY PREVIOUS VACCINATION. I 5 I
t he period with which we are engaged. Thus, in a letter from Mr. Edward
Greenhow, of North Shields, to the London Medical Gazette of February 2, 1833,
vol. xi., p. 590, we read :—" And not only is the small-pox after vaccination
becoming much more frequent, but it is becoming also much more virulent. It is
true, in the greater number of cases, the disease is modified, often turning on
the fifth and sixth day ; but cases are by no means rare where the disease is
confluent, and runs its full course, unmitigated by the previous vaccination,
and death occasionally ensues.
" From what I have above stated, it would appear that vaccination is losing its
protective influence ; and it becomes a matter of serious consideration to
ascertain to what causes we are to attribute this failure. Is it that its
protective power wears out after a certain number of years, and that it becomes
necessary to repeat the operation ? Or is it that the vaccine virus loses
wholly, or in part, its virtues, by passing so repeatedly through the human
system ? The latter is the opinion that has forced itself upon my conviction,
because the disease has principally attacked young persons, and such as have
been vaccinated within the last ten or twelve years, and by far the largest
portion have been done much within that period, so that the numbers attacked are
in the inverse ratio to the number of years which have elapsed since they were
vaccinated." I may observe that the age-incidence of this disease did not begin
to alter very much until after the epidemic of 1837-38, which would account for
the large proportion of young persons attacked at an earlier date. The same
fact was noticed by one of Dr.
John Thomson's correspondents, Mr. William Gibson,1 in his experience at New
Lanark, where, of 251 vaccinated cases of small-pox, 191, or y&i per cent.,
took the disease at intervals up to ten years after vaccination. In 1837 the
reviewer in the British Annals of Medicine, in criticising certain statements
.^bout vaccination, pertinently inquired, " Will it not "b"e better to collect
facts patiently, and to remain a little longer in suspense, than assume a
dogmatical tone, or assert a blind belief, and thus silence inquiry?"2
Sir Henry Holland, in his "Medical Notes and Reflections,"3 writes (p. 401)—"Not
only in Great Britain, but throughout every part of the globe from which we have
records, we find that small-pox has been gradually increasing again in frequency
as an epidemic ; affecting a larger proportion of the vaccinated; and inflicting
greater mortality in its results." Again he says (p. 414)—"It is no longer
expedient, in any sense, to argue for the present practice of vaccination as a
certain or permanent preventive of small-pox. The truth must be told, as it is,
that the earlier anticipations on this point have not been realised."
Dr. George Gregory was also known to be somewhat sceptical as to the merits of
vaccination, and this fact comes out clearly in his writings. In 1823 he
wrote,
1 Letter from Mr. William Gibson to Dr. John Thomson, dated
January II, 1819. "An account of the varioloid epidemic which has
lately prevailed in Edinburgh, and other parts of Scotland," pp. 251-258.
John Thomson, M.D., F.R.S.E. London, 1820.
2 "British Annals of Medicine, Pharmacy, Vital Statistics, and General
Science," vol. i., p. 235. (February 24, 1837).
3 "Medical Notes and Reflections." Henry Holland, M.D., F.R.S.
London, 1839.
<>VKk-SANGUINE PATHOLOGISTS. 153
I'hr acknowledged frequency of cases of small-pox uli'ici|ii(-iit to
vaccination, in all parts of the country, is ucli iih to liiivc excited, in no
inconsiderable degree, the i'-art of many, and the anxieties of all. No one can
Ionic buck upon the history of the last few years without ii'dinjjf sensible
that these unpleasant occurrences are ■ hi the increase."1 In 1837 he says,
"Many of the physicians and surgeons who flourished at the com-nii'iiccmcnt of
this century, and to whose generous efforts in behalf of vaccination the world
is deeply indebted, are passed from this scene. A few still ■■iirvive, who, when
they call to mind the strong hopes which were held out, in their day, of the
ultimate extermination of small-pox, will probably be surprised In find that,
after the lapse of thirty-six years, smallpox still prevails; that the same
necessity exists now as formerly for studying its various aspects ; and that I
ho benevolent anticipations of 1800 receive no countenance from the facts of
1836. It is impossible to deny, and useless to conceal, that these bright
prospects were originally built upon very slender foundations. The wish was
father to the thought." 2
I n 1840 Dr. Gregory writes :—" It is often noticed that persons (vaccinated
persons, for instance) who resist small-pox in common years, though fully
exposed to the contagion, are attacked by it in years of epidemic prevalence.
These and other facts, which bear on the epidemic origin and diffusion of
small-pox, were overlooked by those sanguine pathologists, who
1 " Mcdico-Chirurgical Transactions," vol. xii., p. 324, 1823. v " British
Annals of Medicine, Pharmacy, Vital Statistics, and General Si'ience," vol. i.,
p. 193. (February 17, 1837.) 11
imagined that in vaccination nature had provided us with means adequate for the
complete extermination of small-pox from the earth."1
Increased experience does not appear to have modified Dr. Gregory's views, for
twelve years later we find him writing, " When we look around us,—when we
observe the quantity of small-pox, now (at the close of the first half century
from the promulgation of vaccination) diffused through this and other countries,
—when we see the practice of revaccination almost universal on the continent of
Europe, and greatly increasing in this country, we are led irresistibly to the
conclusion, that these broadly-urged claims in favour of vaccination have not
been substantiated. Small-pox does invade the vaccinated, and the extirpation of
that direful disorder is an event as distant now as when it was first heedlessly
(and, in my humble judgment, most presumptuously) anticipated by Jenner."2
In the Report of the Vaccination Section of the Provincial Medical and Surgical
Association, it is stated, " It will be observed in subsequent parts of our
Report, that failures are noticed at all periods, from a few weeks after
vaccination up to thirty or more years. It has been supposed that they are most
common at and after the age of puberty ; but this is certainly not the opinion
of our correspondents in general. Some, it must be admitted, do affirm that
small-pox has more frequently occurred in persons
1 Article by Dr. Gregory on "Small-pox" in Tweedie's "Library of Medicine," vol.
i., p. 310. London, 1840.
''Medical Times and Gazette. New series, vol. iv., p. 633. (June 26, 1852.)
ADMISSIONS OF THE "LANCET." 155
recently vaccinated, than in those at a remote period, while others assert that
time makes no difference."1
Even the Lancet, which has generally been known as a thorough-going advocate of
vaccination, reluctantly writes:—"In the public mind extensively, and, to a more
limited extent, in the profession itself, doubts are known to exist as to the
efficacy and eligibility of the practice of vaccination. The failures of the
operation have been numerous and discouraging. It has failed frequently by
producing no effect at all; it has failed by producing a vesicle by no means
clearly indicative of the existence of the vaccine disease ; and it has failed
in protecting persons so vaccinated from a future attack of small-pox."2
Thus, in the early epidemics, the cases of smallpox after vaccination were
numerous; but, in estimating the number, we must take account of some of the
cases which have been ascribed to chicken-pox. Sir Thomas Watson, writing in
1848, said, "These mild and irregular forms of variola, both parents and medical
men, wishing, I suppose, to believe nothing in disparagement of the protecting
power of vaccination, are very apt to consider, and to call chicken-pox."3 In
the early days, however, it was by no means only the mild cases that were thus
designated.
In a report on the cow-pox inoculation from the practice at the
Vaccine-pock Institution, during the
1 " Transactions of the Provincial Medical and Surgical Association," vol.
viii., pp. 35, 36. (1840.)
- The Lancet, May 21, 1853. (Vol. i., p. 476.)
3" Lectures on the Principles and Practice of Physic," vol. ii., p. 805. Third
edition. 1848.
years 1800-02, we read (pp. 19, 20):—"It may be also useful to notice that we
have been alarmed two or three times with the intelligence of the small-pox
occurring several weeks or months after our patients had undergone the cow-pock.
We thought it our duty to visit and examine these patients, and also to inquire
into their history among their attendants, and by these means we obtained the
completest satisfaction that the pretended small-pox was generally the
chicken-pox.'' They gave the following instance as an illustration in which the
eruptions were, by their resemblance, mistaken for small-pox by the friends of
the patient, and even by a medical practitioner, "who accordingly gave a
representation of the case by no means advantageous to the Institution." The
child was vaccinated on April 1, 1S00; a genuine vaccine scab was formed, which
fell off and left a cicatrix. Four months afterwards the child was attacked with
fever, followed by an eruption, which when seen at the Institution, presented
over one hundred eruptions of blackish scabs and red spots, " apparently the
chicken-pox, in the scabbing state." Small pits were observed some months
afterwards.
Dr. John Walker,1 the resident vaccinator of the Royal Jennerian Society,
related that a father called on him and informed him that, of two children he
had vaccinated the previous spring, one was now covered with small-pox, and the
other sickening, and that he (the father) was advised to advertise it. On
consulting the register, Dr. Walker found both the cases marked perfect, and he
told the father that it was impossible for
1 Medical and Physical Journal, vol. xii., p. 543. (December, 1804.)
' \SI«:s ATTRIBUTED TO CHICKEN-POX. 157
i-illii-i nl the cliildren to be infected with small-pox ; he linn railed on the
vice-president, Mr. John Ring, and i li,illcii|;c(l him to come and detect his
(Dr. Walker's) l.iilurc. " Me had the goodness to accompany me, mil mi our
seeing the child, he immediately declared 11 i hicken-pox."
I >i. William Farquharson, Mr. James Bryce, and Mr. \. (iillcspie, of Edinburgh,
in a joint letter to Dr. Walker,1 remark on many children who had passed
K'Hiilarly through the process of vaccination, but on whom eruptions appeared at
different periods afterwards, which by some ignorant people were supposed i" he
variolous; but which, upon investigation, uniformly i Mined out to be
chicken-pox. In some of these cases i lie eruptive fever was very severe,
sometimes even iilended with convulsions; and the consequent erup-i ii his very
numerous, and in a few cases the last of i he pustules did not disappear until
the fifth or sixth
■lay. "These cases," they add, "were repeatedly visited
l>\' many medical practitioners of this place, as well as
l>v ourselves, and none of them entertained any doubt
■pi the disease being chicken-pox."
A case is recorded in the Medical and Chirurgical h'rvitrwi1 A child was
operated on by Mr. Ring in May, 1804, who expressed himself as perfectly
satisfied with the progress of the vaccination, saying that "he would forfeit a
hundred guineas if the child ever took I he small-pox afterwards." A distinct
scar was left on each arm as the result of the operation. In October or
1 Medical and Physical Journal, vol. xiii., pp. 286, 287. (March, 1805.,
'Medical and Chirurgical Review, vol. xi., pp. cvi.-cviii. (March) 1 hi
15.)
November of the same year it was taken ill, and the pustules were pretty
numerous, particularly on the scalp, two of them leaving pits ; the patient was
seen repeatedly during the progress of the eruption by Mr. Ellis, apothecary, of
Drury Lane, who asserted it to be small-pox. The child was next taken to Mr.
Soley, apothecary, in Bloomsbury Square, about the ninth day. He declared
immediately, and without hesitation, that it was undoubtedly small-pox, and he
chided the mother for not having taken means to prevent it by vaccination. She
replied that she had done all in her power by having the child vaccinated by Mr.
Ring. "Then," said Mr. Soley, "it cannot be small-pox, for small-pox never
occurs after cow-pock. It must be a rank kind of chicken-pox ;" and he sent her
to Mr. Ring. On calling at Mr. Ring's house, she first saw his assistant, who
declared it to be small-pox, and upbraided the mother for not having had the
child vaccinated. When Mr. Ring was informed of this unusual circumstance, and
on seeing the child, he remarked that it could not be small-pox, for this
disease was never attended by itching, nor did it appear in clusters, as in this
case. He told the mother she might rest satisfied that it was not small-pox, and
he begged her to say nothing about it, as it might excite alarm. In a foot-note
on p. cvii., the editors remark on the above case :—" This attempt to conceal
everything that appears unfavourable, so frequently resorted to by certain
pretended friends of vaccination, cannot be too much reprobated. It shows the
business to have got into very bad hands. Were truth their only object, they
would court investigation, not endeavour to suppress it."
CASKS OK CONFLUENT CHICKEN-POX. 159
Mr. John Ring, in the Medical and Physical Journal? Have a description and
drawing of a case of confluent chicken-pox in a boy four years of age, who had
been vaccinated some time before. He added : "When the chicken-pox broke out in
so formidable a manner, it was mistaken for the small-pox."
In the Medical and Physical Journal11 for November, 1X05, Mr. R. Hall, of
Clement's Inn, related instances in I lie family of a Mr. Ross. An eruption
appeared on two of his children, one of whom had been vaccinated about a year
before. In both cases, the eruption was extremely copious, but the pustules were
much larger and more confluent in the one which had not been vaccinated. Mr.
Hall says : " In both, the pustules so exactly resembled—in form, figure, and
other circumstances—those of small-pox, that, had we founded our opinion on the
external character alone, we should most unquestionably have deemed them both
cases of genuine small-pox ; but, as they neither went through the regular
course, nor were attended with any of those symptoms which uniformly accompany
violent cases of small-pox, .... we did not hesitate to consider them as cases
of confluent varicella."
In the twentieth volume of the Medical and Physical Journal, on pp. 257, 258
(September, 1808), Mr. Thomas Hardy relates the case of a patient who, four
years after he had vaccinated her, was much indisposed, and had a considerable
eruption, which he supposed to be the chicken-pox, until the fourth day of the
eruption,
1 Medical and Physical Journal, vol. xiv., pp. 141, 142. (August, 1^05.)
when the phenomena, both local and general, induced him "reluctantly" to alter
his opinion.
Dr. Richard Pew, of Sherborne,1 also saw a post-vaccinal case, in which the
pustules " bore so general a resemblance to real small-pox, that anyone
acquainted with the subject must immediately acknowledge them to be a branch of
the same family."
In 1818 there was published the Substance of a Correspondence between the
Directors of the Cow-pock Institution, Sackville Street, Dublin, and their
subscribers or other medical practitioners; and also with the Irish Medical
Staff and Militia Surgeons, being replies to certain queries circulated by the
Directors, occasioned by alleged failures in vaccination. A number of the
replies testified to the occurrence of chicken-pox after vaccination.
Mr. Heron, of Lucan, remarked "that in the summer and autumn of 1810 a very bad
kind of pustular eruption made its appearance among the children about Banagher
and its neighbourhood, which many of the practitioners in these places took for
small-pox, and inoculated with matter from it as such. From observations,
however, then made, it appeared to Mr. Heron to be nothing more than a malignant
chicken-pock, of which some died."2
Dr. Little, of Ballina, stated that, " about three years ago, the regiment to
which he belonged, being quartered in Tuam, a very severe form of confluent
varicella prevailed epidemically, and he was repeatedly called
1 Medical and Physical [ournal, vol. xxi., p. 250. (March, 1809.)
2 " Historical Sketch of Small-pox," p. 252. John Thomson, M.D.,
F.R.S.E. London, 1822.
DR. P. MUDIE'S EXPLANATION. l6l
upon to see children as well of the townspeople as the soldiers, whom he had
vaccinated, and who were marked in his journal as having gone regularly through
the disease; but in no instance could he hesitate as to the nature of the
disease, which, though often of a mixed nature, was genuine, and of the conoidal
form, as described by Dr. Bateman."1
Dr. P. Mudie, in a letter to Dr. Thomson, dated October 18, 1818, freely
acknowledges a bias in his own mind with regard to the prevalence of small-pox
after vaccination. " Of late years," he says, " I have remarked, that the
disease called chicken-pox has been much more severe than it used formerly to
be, and many of the cases, occurring after vaccination, so much resembled
small-pox, that if my mind had not been prejudiced against the possibility of
such an occurrence, I would have pronounced the eruption to have been of a
variolous nature."2
Thus there were a large number of vaccine failures in the early years of the
century ; and, if we include some of the chicken-pox patients, there must have
been thousands of such cases in the epidemic of 1817-19. Secondly, these
failures took place at all periods after vaccination, even within a few weeks or
months of the operation. Thirdly, post-vaccinal small-pox, according to these
early records, did not seem to be an especially mild disease; and lastly, there
did not appear to be any
1 "Historical Sketch of Small-pox," pp. 252, 253. John Thomson, M.D.,
F.R.S.E. London, 1S22.
'* An account of the varioloid epidemic which has lately prevailed in Edinburgh
and other parts of Scotland, p. 240. John Thomson, M.D., F.R.S.E. London,
1820.
relation between the severity of the disease and the length of time which had
elapsed since the operation.
Vaccination was first made compulsory in 1853. It is difficult at this day to
understand how the promoters of vaccination managed to get this Act on our
Statute Books, except on the assumption that the overwhelming evidence of the
early failures of vaccination had been overlooked or forgotten.
Mr. George Canning declared, in 1808, that although he considered the discovery
(vaccination) to be of the very greatest importance, he could not figure any
circumstances whatever that could induce him to follow up the most favourable
report of its infallibility, which might be brought forward, with any measure of
a compulsory nature.1
We have it on the authority of Mr. T. S. Duncombe, M.P. for Finsbury, that in
1840, Sir Robert Peel, being urged to make vaccination compulsory, expressed his
opinion that such a course would be repugnant to the habits and feelings of the
British people, and to that freedom of opinion and action to which they were
well accustomed.2 Mr. Duncombe quotes Sir Robert as saying that:—" The proposal
to make it compulsory was so contrary to the spirit of the British people, and
the independence in which they rightly gloried, that he would be no party to
such compulsion."3 Sir Robert Peel, however, died in 1850, and in 1853 a measure
involving an enormous curtailment of the liberty of the
' Hansard's Parliamentary Debates. First series, vol. xi., p. S44. (June 9,
1808.)
-Ibid., third series, vol. cxliii., p. 552. (July 10, 1856.) "Ibid., vol.
clxiv., p. 674. (July IO, 1861.)
VACCINATION MADE COMPULSORY. 163
subject, without any demand for such legislation, and without previous inquiry,
was passed through both Houses of Parliament with very little discussion.
Lord Lyttelton introduced the Bill into the House of Lords, and, on the motion
to go into Committee, explained that, having no scientific knowledge of the
subject himself, he was indebted for almost all his information to some able and
learned members of the Epidemiological Society. " It was unnecessary," he
informed the House, " to speak of the certainty of vaccination as a preventive
of the small pox, that being a point on which the whole medical profession had
arrived at complete unanimity."1
If we refer to the Return on "Small-pox and Vaccination,"2 prepared by the
Committee of the Epidemiological Society, and from which Lord Lyttelton obtained
his information, we find certain extraordinary and wholly unwarrantable
statements (p. 4). " Small-pox is a disease," say the authors, " to which every
person is liable, who is not protected by a previous attack or by vaccination."
Again : " Every case of it is a centre of contagion, and every unvaccinated or
imperfectly vaccinated population is a nidus for the disease to settle in and
propagate itself."
' Hansard's Parliamentary Debates. Third series, vol. exxv., p. 1002. (April 12,
1853.)
" Copy of " Letter from Dr. Edward Seaten to Viscount Palmerston, with enclosed
Copy of a Report on the State of Small-pox and Vaccination in England and Wales
and other Countries, and on Compulsory Vaccination, with Tables and Appendices,
presented to the President and Council of the Epidemiological Society by the
Small-pox and Vaccination Committee, the 26th day of March, 1851."
Parliamentary Paper, No. 434. Ordered, by the House of Commons, to be printed,
3rd May, 1853.
The two latter propositions, we are seriously informed, " do not admit of being
controverted." We will suppose, for the sake of argument, that none of these
propositions are capable of refutation. We then read : " If it admit of doubt,
how far it is justifiable in this free country to compel a person to take care
of his own life and that of his offspring, it can scarcely be disputed that no
one has a right to put in jeopardy the lives of his fellow-subjects."
Here the question presents itself, if vaccination is a preventive of small-pox,
as asserted by Lord Lyttelton, how could the unvaccinated put in jeopardy the
lives of their protected fellow-subjects? Thus, there is no argument for
compulsion, even if it be admitted that vaccination protects for life; if
vaccination does not protect for life, and it is evident from the numerous cases
I have quoted, that it does not do so, then the profession should show how long
its protective value lasts. Of the various medical experts who have been
examined before the recent Vaccination Commission it is important to remember
that none have endorsed the opinion of Jenner, Sir John Simon, and others, that
vaccinated persons are for ever afterwards secure from the infection of
small-pox. Although some have maintained that vaccination protects for
considerable intervals, one prominent official expert, Dr. Wiiliam Gayton,
thinks that "primary vaccination is a very fleeting protection indeed. As to the
time that that primary protection lasts, I do not know, but I think it is a very
short time" (Q. 1,755). Another authority, Dr. R. A. Birdwood, with an
experience of 12,000 cases of small-pox, emphatically stated that vaccination
cannot
DR. JAMES COPLAND'S VIEWS. 165
be relied on as an absolute protection up to any age whatever (Q. 31,191). And
lastly, there have been witnesses of the very highest professional standing and
scientific attainments, who have maintained that vaccination exerts no specific
protective influence at all. When the profession are agreed on this important
point, then the vaccinated will be able to make themselves secure by periodical
re-vaccinations, and their lives will not be placed in peril by anti-vaccinists.
It is interesting to note that the first compulsory Act of Parliament entirely
failed to remove the honest doubts of some distinguished members of the medical
profession. Thus Dr. James Copland expressed the opinion that vaccination " will
never be generally adopted, and that, if it were so adopted, it could never
altogether banish small-pox, nor prove a complete or lasting preventive of
variolous infection."1
Again he writes (p. 829):—"At the time of my writing this, just half a century
has elapsed since the discovery and introduction of vaccination ; and after a
quarter of a century of most transcendental laudation of the measure, with
merely occasional whisperings of doubt, and, after another quarter of a century
of reverberated encomiums from well-paid vaccination boards, raised with a view
of overbearing the increasing murmurings of disbelief among those who observe
and think for themselves, the middle of the nineteenth century finds the
majority of the profession, in all latitudes and hemispheres, doubtful as
to the preponderance of
lf'A Dictionary of Practical Medicine," vol. iii., part ii., p. 831. James
Copland, M.D., F.R.S. London, 1858.
advantages, present and prospective, to be obtained either from inoculation or
from vaccination."
I now propose to show that the unvaccinated when exposed do not necessarily take
small-pox, and also, that since the population has been more ■ largely "
protected," it is the vaccinated who form not only an overwhelming proportion of
the sufferers, but in a large number of instances they are the means of
propagating the disease.
Some very remarkable cases are recorded by Dr. William Baylies in his little
book, entitled, " Facts and Observations Relative to Inoculation in Berlin"
(1781, pp. 132-144). The King of Prussia having given his sanction to
inoculation in February, 1775, eight orphan children were chosen to commence the
series, and only those were selected who were perfectly free from all marks or
signs of their having gone through the smallpox before ; a thread was used,
which had been charged with fresh variolous matter at the London Small-pox
Hospital; the matter was inserted into both arms of the patients, and Dr.
Baylies had not the least doubt the disease would come on as it ought to do; yet
we are informed that " neither fever nor any other symptom followed in
consequence of it, though the arms of two of them, on the third or fourth day
from the operation, had a degree of inflammation for a day or two" (p. 138).
He then used a thread of much older matter, and re-inoculated these eight
children, and also inoculated, for the first time, four others, with a similar
result; and lastly, having learnt that the child of a baker was down with the
disease, he resolved to inoculate them with fresh
UK. MICHAEL UNDERWOOD'S OPINIONS. 167
vui'iolouK matter. The twelve children before-mentioned, willi seven others,
were conducted to the baker's house, ami they were all inoculated with warm
fluid matter limn ripe pustules, and for nearly an hour the children were kept
in the infected atmosphere, and " not one of all the nineteen children
manifested the least symptom nf the disease in consequence of it" (p. 143).
As Dr. Baylies was a practised inoculator, we are forced to the conclusion that
either the children had had Min.ill-pox before — the conclusion arrived at by
Dr. Hay lies himself—or that they were naturally immune to the* disease ; but,
considering that the most careful examination was made for marks of small-pox,
the latter view appears to be the more probable.
In this connection some remarks made by Dr. Michael Underwood, in his work on
the diseases of children, are not without interest. Dr. Underwood
observes:—"Though the small-pox is a complaint so incident to the early part of
life, that comparatively lew children living to the age of eight or ten years,
arc found to escape it, yet it is not so readily communicated, in the state of
early infancy, as hath been |.;rnerally imagined, unless by immediate infection.
The poor furnish frequent instances of the truth of I his observation. I have
attended where children born In an air, saturated as it were, with the miasma
(or Infectious particles) of this disease (as well as of the measles), and even
lying continually in a cradle in which another child has died a few days before,
have, nrvcrtheless, escaped the disease, and sometimes, when I hey have slept
together in the same bed with one loaded with it. Hence it appears, that
highly tainted
air, and even personal contact, are often insufficient t< communicate the
poison. Yet we know that infant; are very easily infected, receiving the
small-pox b\ inoculation as readily as adults ; though neither are a all times
equally susceptible of it."1
In the Medical and Physical Journal2 for April, 1803 Mr. C. Dennett, of Soho
Square, related the following
instances :—In August, 1800, Mr.----- had two childrei
who were laid up with confluent small-pox, one of whorr died ; an infant, three
weeks old, was exposed to th< infection the whole time, being always in the same
room and sometimes in the same bed. Mr. Dennett says hi could not persuade the
parents to have the baby inocu lated, and to vaccination they positively
objected. I did not take the infection ; later in the year, the chile was
inoculated with fresh variolous matter withou' effect, and this was repeated
three times with no bette; success.
Another child in the same family, born later, escapee the disease, although it
had slept in the same bed witr the former child, who had now contracted
confluen1 small-pox. Mr. Dennett inoculated the infant on foui separate
occasions with small-pox matter without effect These cases were evidently not
very uncommon, for Mr Dennett remarked that " every practitioner must have met
with cases when, under some peculiar constitution the habit is not susceptible
of the disease, either bj infection or inoculation " (p. 364).
1 "A Treatise on the Disorders of Childhood, and Management o
Infants from the Birth," vol. i., pp. 299-301. Michael Underwood, M.D.
Physician to Her Royal Highness the Princess of Wales. London, 1797.
2 Medical and Physical Journal, vol. ix., p. 365.
IMMUNITY IN THE UNVACCINATED. 169
Dr. Lionel Beale gives the following on the authority of the Lady Superior of
St. John's House :—" S. L., aged 1.3, Westminster, took the small-pox in March,
1871. The rash was fully out all over face and body March 10th. The mother and
baby of a week old slept in the same bed and continued to do so. The baby has
never been vaccinated, and is now nine weeks old, and has been sleeping in the
bed night and day. The mother was vaccinated as a child thirty-five years ago.
The other children in the room had been vaccinated. The father has never been
vaccinated at all, and slept in the same room. No other member of the family has
had the small-pox."1
Dr. W. N. Thursfield, Surgeon to the Wellington Dispensary, refers to the
following cases in the Lancet of June 1, 1872 (vol. i., p. 754):—"On the 25th of
March of this year, I was sent for to see a Mrs.
W----- , a lady I had attended in her confinement five
months previously, and whose child had not been vaccinated in consequence of the
express prohibition of both parents. I found the lady suffering from a severe
attack of small-pox. The eruption, which was said to have appeared four days
previously, was then in the pustular stage. She had not discontinued nursing the
infant, and it was taking the breast at the time of my visit. The child was at
once removed from the mother, but not from the house, where it
remained
throughout. Before Mrs. W---- could be said to have
completely recovered, she, in spite of remonstrance,
1 " Disease Germs ; their Nature and Origin," p. 441. Second edition. Lionel S.
Beale, M.B., F.R.S. London. 1872.
resumed suckling the child, and continued to do so for some time. At the present
date (May 2Oth) the child is quite well, and has had no eruption or feverish
symptoms whatever, and is still unvaccinated. This lady's husband contracted
small-pox during his wife's illness ; both had been vaccinated in infancy, and
both recovered.
"In another case, a young man, lodging in a house near to where small-pox had
been for some time, was taken with a moderately severe attack of the disease,
and came under my care as a dispensary patient on Good Friday last. The old
woman of the house, who nursed and looked after the patient, was bringing up by
hand an illegitimate infant, then ten weeks old, which had been put out to nurse
with her. This infant had not been vaccinated; and, though in constant contact
with the nurse, and sleeping with her in the room next to the small-pox patient,
did not take the disease, and through the neglect of the woman to take it to the
public vacci-nator, it remained unvaccinated. About five weeks after the
recovery of the young man, the nurse-child died of general debility. I kept it
under my observation until its death, and know that it had not small-pox.
" In both these cases, there certainly was no error in diagnosis, nor was either
of the infants vaccinated or out of my personal observation at any time."
In the Sheffield Report (p. 46, foot-note), Dr. Barry, in referring to the case
of Mary P., aged twenty-four, who took small-pox after vaccination, says :—" Of
five other children in this family, three, aged eleven, fifteen, and sixteen,
who had been vaccinated in infancy, all suffered from small-pox ; the last two
were badly pitted.
DR. COUPLAND'S REPORT. 171
'I'wo other persons, aged fourteen and twenty, who had never been vaccinated,
and who slept with the others, did not contract small-pox."
The above instances appear to show that immunity in the unvaccinated, even when
strongly exposed to .mall-pox, is not nearly so rare as has been generally
believed. It is also instructive to note that Dr. Coupland,1 in his report on
the Leicester outbreak, ■hows, with regard to 193 invaded households, that at
cveral specified age-periods, the small-pox attack-rates were much the same,
although, according to his census (if the inmates, the proportion of the
unvaccinated at 1 liese age-periods vastly differed. The figures cited are as
follows :—
Of the total inmates, the percentage.
Age-periods. inmates.2 Unvaccinated.
Attacked.
Under 1 year ... ... 33 (pro
21'2
1-10 years............................... 328 74^0
28^9
10-30 years ... ... 534 15-5 28'i
30 years and upwards ... 330 27 2C5
With these figures before him, it is not surprising that Dr. Coupland should
have come to the conclusion that " the natural liability to small-pox,
unaffected by vaccination, was not so great as has been supposed."
To resume our inquiry into the question as to whether vaccination prevents
small-pox, the following cases, extracted from the Sheffield Report, are of
importance as showing that recent vaccination of the most approved fashion will
not secure immunity from this disease. (See next page.)
1 Final Report, Royal Commission on Vaccination, Appendix vi., p.
3.
2 In nine of the inmates the age was not ascertained.
R&n. Di^<- N°- N—
tftLIed" Vaccination. Results of vaccination. J%^
41 Btightside - - 27 Mary H. - - 10 months
Vaccinated Five foveated cicatrices, two- Very slight, not
in infancy thirds square inch in area. pitted.
41 Brightside - - 41 Sarah C. - - 6 months
Vaccinated Four foveated cicatrices, one- Very slight, not
in infancy half square inch in area. pitted.
42 Brightside- - 102 Sarah Ann L. - 10 months Vaccinated
Four plain cicatrices, one- Very slight indeed,
in infancy half square inch in area. not pitted.
62 North Sheffield - 79 Ernest C. - - 9 months Vaccinated
Four foveated cicatrices, one- Very mild, one
in infancy half square inch in area. pit.
97 South Sheffield - 29 Gertrude 2 months Vaccinated
One plain cicatrix, one-eighth Slight, not pitted.
Hoskins M. - when square inch in area.
6 weeks old
150 Nether Hallam - 18 Frank S. - ' - 6 months Vaccinated
Four foveated cicatrices, two- Very slight, play-
when
thirds square inch in area. ed about all the
6 weeks
old
time, not pitted.
150 Nether Hallam - 57 Hedley V. H. - 8 months Vaccinated
Three foveated cicatrices, Very mild, not ill
in infancy one-third square inch in at all, not pitted,
area.
I ATM, SMALL-POX IN VACCINATED CHILDREN. 173
Kxamples of more absolute failure to protect could liardly be imagined than
these seven cases contracting •.mall-pox from a fortnight to seven or eight
months after vaccination of the most correct type. Altogether the -re were about
450 vaccinated cases under ten years of age at Sheffield in the 1887-88
epidemic, and yet a prominent defender of compulsory vaccination deliberately
maintained that " vaccinated children under ten years of age are . . . wholly
and entirely immune from small-pox, and cannot be infected."1
Since writing the above, it appears that the editor of the British Medical
Journal has somewhat shifted his ground, for in a recent article on "Vaccination
as a Branch of Preventive Medicine," he maintains that in certain epidemics
(referred to) " vaccinated children under ten have been almost immune from death
by small-pox,"2 which I venture to suggest is a considerable modification of his
original statement. It is a pity that Mr. Ernest Hart did not have an
opportunity of consulting Dr. John MacCombie's article on " Small-pox " in the
same volume (Allbutt's " System of Medicine," vol. ii.), for he would then have
discovered . the following figures (p. 221):—
Vaccinated.
Fatality
Age-periods. Cases.
Deaths. per cent.
Under 5 years ... ... 385 30
7'8
5-9 years............................. 1,468
59 4-0
It must also be presumed that Mr. Hart's attention has not been arrested by
the following experience of the
1 Letter ot Mr. Ernest Hart to the Times of August 31, 1894.
■ Allbutt's " System of Medicine/' vol. ii., p. 664. London. 1897.
Metropolitan Asylums Board* in the epidemic of 1870-72:—
Vaccinated.
Number Number of Fatility
Age-periods. admitted.
deaths. per cent.
Under 5 years ... ... 195 38 I9'5
5-10 years 786 60
76
These two tables prove that "vaccinated children" under five years of age (let
alone ten years) are not even "almost immune from death by small-pox."
What could be more emphatic than the following experience of Mr. T. Massey
Harding?2—"All practitioners are acquainted with cases disproving the immunity
of the vaccinated, such as the following :—I attended a man, aged 40, with
confluent small-pox, of which he died. He had been vaccinated twice, according
to his own statement. In the house were his sister, her husband, and two
children, all unvaccinated. I vaccinated them all, and it took effect. In three
weeks from the day of vaccination, the woman, Mrs. G., and one of her children
had small-pox, distinct, but slight."
Nor can it be truthfully said that epidemics originate with the unvaccinated,
for in a number of notable instances the first unvaccinated case is a long way
down the list. Thus, at Neuss, in Germany, from 1865-73, there were 247
cases of small-pox, all of
1 " Report of the Committee appointed on the 1st June, to collate and
report upon the Returns obtained from the several Hospitals of the
Managers, with regard to the cases of Small-pox treated therein." Pre
sented to, and adopted by, the Managers of the Metropolitan Asylum
District, at their meeting on the 13th July, 1872. P. 5 ; Table 2.
2 British Medical Journal, November 21, 1857, p. 974.
STATISTICS OF VACCINATED SMALL-POX. 175
llicin vaccinated; at Bromley, in 1881, 43 cases, all vaccinated ; and in the
1870-72 epidemic at Bonn, 1 he first unvaccinated case was forty-second on the
list.1
The following table shows the large proportion of vaccinated cases in some
well-vaccinated districts:—
Small-pox epidemics. Years. Attacks.2 Va"lnilt«d
of attacks
attacks. vaccinated.
liavaria3................................... ...
1S71 30,742 29,429 957
lierlin4
1871-72 20,391 17,038 83-6
Cologne4
1871-73 2,282 2,248 98-5
Ncuss4
1865-73 247 247 ioo-o
I,ondon Small-pox Hospital6 1852-67 13,581
10,661 78-5
Metropolitan Asylums Board j l8y(>86
SOj668 ^^ gro
1 lospitals 6 ... ... J
Uromley7
1881 43 43 ioo'O
Sunderland8 ... ... ...
1884 100 96 96^0
Sheffield
1887-88 7,066 5,891 83-4
Warrington ... ... ...
1892-93 674 601 89^2
Kirmingham................................................ 1893-94
2,945 2,616 88'8
Willenhall .....
1894 828 739 89-3
In an epidemic, it is not possible, on any theory of protection, for the
population to be vaccinated to any
1 " Beitrage zur Beurtheilung des Nutzens der Schutzpockenimpfung,"
p. 143. Berlin. 1888.
2 Cases in which there was a doubt about the raccinal condition of the
patient have been excluded.
a Second Report Royal Commission on Vaccination. Q. 1,489. 4 " Beitrage zur
Beurtheilung des Nutzens der Schutzpockenimpfung," pp. 152, 154, 168.
Berlin. 1888.
0 Report from the Select Committee on the Vaccination Act (1867) 1871,
1>- 237-
0 Third Report Royal Commission on Vaccination, Appendix, p. 204. Table L.
''Lancet, August 27, 1881, vol. ii., pp. 372, 373.
8 Lancet, February 23, 18S4, vol. i., pp. 363, 364.
lesser extent than the cases of small-pox, or it would show that small-pox
picked out the vaccinated for its victims. The figures for Bavaria and Cologne,
with 957 and 98-5 per cent, of the cases vaccinated respectively, hardly leave
any margin for the population to be vaccinated to a greater extent. Considering
that in these two instances the proportions approximate so closely, there is
every reason for scrutinising very carefully any estimate of the vaccination of
the population which differs largely from the ratio of the vaccinated cases of
small-pox.
Such estimates have been made for Sheffield by Dr. Barry, and for the houses
invaded by small-pox at Warrington, Dewsbury, and Leicester, by medical men
appointed by the Vaccination Commission. As, in the latter instances, there was
no opportunity for examination of these experts, it will be more satisfactory
if I confine myself to the case of Sheffield.
In his report on the Sheffield epidemic, Dr. Barry estimated that 97^9 per cent,
of the population was vaccinated. It was pointed out to him before the Royal
Commission, that the house-to-house inquiry, on which his estimate was based,
was taken after the epidemic had reached its height, during the course of which
a transfer had been taking place from the unvaccinated to the vaccinated class.
A new estimate was therefore made, which is included in the Report of the Royal
Commission, at 973 per cent.; but even this cannot be justified. In his
examination before the Royal Commission, Dr. Barry admitted that in the
Sheffield Union, the house-to-house inquiry was enumerated by men under the
supervision of the vaccination officers
Till': SHEFFIELD "CENSUS." 177
' '■ 2,389), and that its primary object was to secure, fur as possible, the
discovery of all unvaccinated iiiltlrcn (Q. 2,390). These were reported to the
vac-'M.ition officers, whose duty it was to take steps to ■ 'lire their
vaccination (Q. 2,391). The "census," Dr. I Liny informs us, was a "secondary
affair" (Q. 2,390). I In's inquiry, therefore, was instituted in order to hunt
up the unvaccinated, and it is obvious that a census < 1 inducted on these lines
could not have the slightest I net fusion to accuracy. It would have been the '.implcst
matter in the world for the householder to omit the mention of the unvaccinated,
and, as the inquiry lasted nearly six weeks, to evade the enumerators, who, in
the Sheffield Union, were not even supplied with the names of the occupiers.
Moreover, in 764 houses, information was altogether refused, and 1 1'8 per cent,
of the population, or over six times tlie "unvaccinated enumerated," were left
out of the calculation altogether. For these and other reasons, il is impossible
that the population could have been vaccinated to the extent that was claimed ;
and, therefore, the calculations that are based on this estimate are
misleading.
It has been shown that the unvaccinated may be exposed to small-pox without
taking the infection, and also that the most recent and efficient vaccination of
individuals will not prevent the complaint, and considering that such a large
proportion of sufferers are among the vaccinated, who, in most instances, start
and spread the epidemic, the statement so often promulgated that an
unvaccinated individual is a source of infection and a danger to
the community, is
erroneous. It has also been pointed out, that even if vaccination was a complete
protection against smallpox, this would be no argument for legislation ; for,
in the words of Dr. J. H. Bridges, " non-vaccinated people are not a source of
injury to their neighbours; for their neighbours can get themselves
vaccinated."1 It follows, therefore, that the law which was first passed on the
assumption that the unvaccinated are a danger to society—even if there were no
other evidence against vaccination—should be immediately abrogated.2
1 Positivist Review, vol. iv., p. 226. (November, 1896.)
2 If vaccination mitigates small-pox, as maintained by some, it is no
argument for compulsion. The medical officer of health to the City of
Birmingham (Report for 1893, p. 45) alleges that one of the causes of the
rapid spread of small-pox in the recent epidemic was due to "the mildness
and modification of the attacks in vaccinated persons, making it most
difficult in some cases to decide the nature of the illness, and causing it to
be mistaken for chicken-pox and other trivial affections, and arousing no
suspicion of its being small-pox until severer iorms of the disease subse
quently appeared in the same family."
CHAPTER VI.
THE MITIGATION THEORY.
When it was discovered, in the epidemic of 1817-19, that small-pox attacked such
a large number of the vaccinated, the theory of mitigation was promulgated. iMom
the cases detailed in the last chapter, it does not appear that small-pox was
very conspicuously mitigated by vaccination in the early years, nor does there
appear to have been any relation between the severity of the attack and the
length of time which hud elapsed since the operation. It will be profitable to
proceed to enquire whether the later experience shows results more favourable to
the mitigation theory. Dr. George Gregory has indicated the measure of the
modifying powers, which, in his opinion, may be attributed to vaccination. "
Vaccination," he says, " does not appear to lessen the violence, or shorten the
duration, of the first or eruptive stage of fever, which is generally as severe,
and even sometimes severer and longer in its duration than that of the casual
confluent small-pox. It does not appear in like manner to influence the </iiantity
of eruption upon the skin, so much, at least, as has been generally imagined. It
is true, that, in many cases of small-pox, subsequent to vaccination, the erup-lion
has been very scanty ; but, in a large number also, I have seen it very copious,
more particularly about the
face, breast, and upper extremities, and occasionally fully equal, in point of
quantity, to what is seen in the worst kinds of confluent or coherent natural
small-pox."1 The great power of vaccination, he thought, consisted in modifying
the progress of inflammation in the variolous eruption on the skin and in the
throat; but he added : " It is curious to observe that it does not always affect
the course of the disease, when the variolous poison fixes itself on other
parts, more particularly on the brain. It is, in this manner, that small-pox,
after vaccination, occasionally proves fatal."2 In a foot-note on p. 331, he
explains that "the eruption on the skin and throat is only one of the effects of
the poison. Another, at least equally important, both with reference to
pathology and practice, is that which is excited upon the brain and nervous
system ; the chief evidences of which are delirium, inflamed eyes, stupor or
restlessness, and disposition to erysipelas and gangrene."
There are several ways of testing the mitigation question, one of which would be
to compare the case-mortality or fatality of small-pox before and after the
introduction of vaccination. In the Appendix will be found a table taken from
Dr. Creighton's " History of Epidemics." It consists of censuses of small-pox
epidemics during the years 1721-30, the fatality ranging from 9/1 to 36-4 per
cent, there being in all 13,192 cases, with 2,264 deaths, or an average fatality
of 17*2 per cent.
The principal objection that has been raised to these
1 " Medico-Chirurgical Transactions," vol. xii., pp. 328, 329. (1S23.)
. 2/^., pp. 330, 331. , , ,„,
., ,. ,
jurin's statistics. iSi
statistics is, that in the censuses of small-pox epidemics passing under the
name of Jurin, which largely dominate the figures in Dr. Creighton's list,
Jurin is said to have " not knowingly set down any deaths under two years old as
due to small-pox, . . . and that some of his correspondents, in furnishing him
with statistics, followed the same rule."1
The ostensible grounds for this assertion are :—
1. That the Aynho census, to which I have referred
in a previous chapter (pp. 43, 44), contains no cases
under two years of age.
The Aynho census, a copy of which is to be found in the archives of the Royal
Society, was made by the rector of the parish, and the cases are given in the
order of time, just as they occurred over a period of some fifteen months, three
in one family, two in another, and so on. There is no suggestion of infants
being excluded, and the fact that there were only three aged two years, and four
aged three years, out of a total of 132, makes the absence of cases in infants
not only credible, but probable. The epidemic was mainly among young people and
adults, and was quite intelligible for a country place where epidemics took
place infrequently.
2. The other ground of objection is founded on an
argument used by Jurin in his letter to Dr. Cotes-
worth.2 " It is notorious, that great numbers, especially
'Article on "Small-pox and Vaccination," by John C. M'Vail, M.D., in Stevenson
and Murphy's " Treatise on Hygiene and Public Health," vol. ii., p. 399.
London. 1893.
" A Letter to the learned Caleb Cotesworth, M.D., p. 11. James Jurin, M.D.,
Secretary to the Royal Society. London. 1723.
of young children, die of other diseases, without ever having the small-pox,"
etc.
The statement that a number of young children died of other diseases, without
ever having the small-pox, has no reference to the censuses which were taken to
show the fatality-rate of natural small-pox as contrasted with the inoculated.
It was part of an argument to show that the real hazard of dying of small-pox in
London was greater than the Bills of Mortality showed, inasmuch as the excessive
London infantile mortality cut off an immense number from other causes (such as
convulsions, infantile diarrhoea, etc.) before small-pox could attack them. But
Jurin admits (p. 12) that in all probability some infants, " very young
children, or at most not above one or two years," went through the small-pox,
which is sufficient evidence that he had no intention of counting them out, or
ignoring them, in the percentages of fatalities to attacks. His argument, such
as it was, applied only to London, but there were no statistics for London in
the censuses, which are all from the provinces, many of them made by Nettleton
of Halifax, and none of them made, nor even controlled, by Jurin himself.
The incidence of small-pox in the eighteenth century, as pointed out in a former
chapter, was almost entirely on the young ; for instance, at Chester,1 in 1774,
of 1,385 cases, 202 died, or a fatality of 146 per cent., the ages at death
being as follows (p. 150; Tables II. and IV.):—
1 " Philosophical Transactions," vol. Ixviii., p. 151. (Dr. Haygarth's
Observations on the Population and Diseases of Chester in the year 1774.)
OPINION OF THE ROYAL COMMISSION. 183
Under 1 month........................... ... ... o
Between 1 and 3 months ... ........................ 3
„ 3 and 6 „ ......................... 4
., 6 and 12 „ .......................... 44
„ 1 and 2 years ............... ... 38
„ 2 and 3 „ ......................... 42
„ 3 and 5 ,.................................... 49
„ 5 and 10 „ ... ... ... 22
Over 10 years .............. ... ... ... o
TotaJ ........................ 202
The contention, therefore, that the last century fatality of 17 or 18 per cent,
is lower than it should be, because of the deliberate omission of young children
from the censuses, is groundless, and ought never to have been raised.1
Let us now see what is the fatality of small-pox since ;i large proportion of
the cases have been vaccinated. Dr. Collins and Mr. Picton2 quote the experience
of the Metropolitan Asylums Board's Hospitals, where, from 1870 to 1894, 60,855
cases were treated, with a fatality of 167 per cent., and among 50,668 of these
admissions, the vaccinated were 41,061, or 81 per cent.
During this period the figures have varied considerably. In the year 1896, the
fatality was 4-oi per cent.; whereas, from December 1, 1870, to February 3,
1 The Royal Commission say (section 53)—" It has been urged that the deaths of
those dying under two years of age were excluded from Jurin's ■,l:ilistics, and
that this must have led to the omission of many deaths, as l he mortality in
that class was high. The evidence relied on to show that nises under two years
of age were excluded certainly cannot be regarded icv establishing it."
'' Royal Commission on Vaccination, Dissentient Commissioners' Statement,
section 97.
1871, it was as high as 2O'8i per cent. This high fatality in the earlier years
may in part be due to the limited accommodation at the hospitals, when the
tendency would be to admit the more serious cases. In this epidemic (1870-72),
however, the fatality was high, for the Lancet of July 15, 1871 (vol. ii., p.
94), estimated the fatality of small-pox at 17-5 per cent. ; and hence, the
large proportion of vaccinated casesx does not appear to have diminished the
severity of the disease, as compared with the last century.
The other method of testing the question is to compare the fatality in the two
classes. Dr. Davies, the medical officer of health for Bristol, in the Bristol
Mercury of April 2, 1896, states the case thus: "The unvaccinated die at the
rate of thirty or forty deaths per hundred cases, the vaccinated at something
less than five per hundred cases." This agrees approximately with Mr. Ernest
Hart's figures2 in his summary of different towns during recent epidemics. The
claim is that vaccination mitigates small-pox in the bodies of those who have
taken the disease, and this is practically the whole case for the observance of
the operation ; and the evidence is chiefly to be derived from the reports of
medical officers of health and others in official position, from which the
following have been taken :—
1 In the epidemic of 1870-72, a total of 14,808 cases of small-pox were
admitted into the hospitals of the Metropolitan Asylums Board. Of these,
11,174, or 75-5 per cent., were in vaccinated persons.
2 British Medical Journal, March 2, 1895, vol. i., p. 487.
FATALITY STATISTICS. 185
Unvaccinated Fatalities—/Sj6-g6.
Report of Hospital or Medical y
c n»ith<i Fatality
Officer of Health. Vearf"
<-ase!" '«aths. per cent.
Ilighgate. ............. 1836-51 2,654
996 37-5
Ilighgate1 ... ... 1871 74
49 66'2
Dublin (Hardwickel Feb. 1871 to^ , „,
Hospital)2 .............. ) March 1872 J 7° 55
7 ^
llomertoij ....... 1871-77 1,243 570 45-9
Hampstead .......... 1876-78 847 397 46^9
Dublin (Cork Street) ... 1876-80 448 288 643
Kulham ... ... ... 1877-79 374
176 47'i
Deptford ...................... 1878-79 258
i2i 469
Sheffield ... ' ... 1887-88 1,173
392 33'4
Uirmingham ............... 1893-94 329 107
32-5
(Iloucester ... ... 1895-96 781
317 4C6
Hence, in these instances, the proportion of deaths to iittacks among the
unvaccinated is stated to have ranged from 78 to 32 per cent. Most of these
figures are, however, impossible, for the simple reason, that in the last
century, as already shown, before the introduction of vaccination, the average
fatality of small-pox was only about 17 or 18 per cent.
In making a critical examination of the fatality •statistics in the two classes,
it is obvious that their accuracy would depend on whether the statement us to
vaccination could be absolutely relied upon ; and secondly, on whether the two
classes were perfectly comparable in every respect; and to do this il is
necessary to say a word or two about the different types of small-pox, and also
the method of I'lassification.
Hritish Mfi/ifitt /onrnat, February 10, 1872, vol. i., p. 171. 'I'M., p. <>Sj,
June 22, 1872. These figures include four doubtful cases. I!',
A prominent feature in medical and official publications advocating
vaccination1 has been to paint the horrors of small-pox in its natural state in
the most vivid colours. I have already dwelt on the fact that, in the last
century, the average fatality of small-pox was only about 17 or 18 per cent, of
those attacked, and in many epidemics the proportion was much less. Different
forms of small-pox have been distinguished from the time of Rhases,2 and it may
be said that Sydenham's main success in his treatment of the disease was due to
the fact that he recognised a discrete and confluent variety, in the former of
which the patient, if left alone to Nature, invariably recovered.
The following quotations from Sydenham bear on this point:—" As it is palpable
to all the world, how-fatal that disease (small-pox) proves to many of all ages,
so it is most clear to me, from all the observations that I can possibly make,
that if no mischief be done, either by physician or nurse, it is the most slight
and safe of all other diseases." 3
Sydenham observes that in 1669 small-pox "appeared
1 See Mr. Ernest Hart's "Truth about Vaccination," pp. 2-8 (1880), and also
"Facts concerning Vaccination for Heads of Families," a tract "revised" by the
Local Government Board, and "issued with their sanction," in which it states (p.
4)—"The disease (small-pox) used to rage unchecked, killing a very large
proportion of those whom it attacked, and maiming, blinding, and disfiguring
those whose lives it spared."
3"A Treatise on the Small-pox and Measles." Translation from the original Arabic
by Dr. W. A. Greenhill, and printed for the Sydenham Society, 1848, pp. 71-73.
3 Letter to Mr. Robert Boyle, dated Pall Mall, April 2, 1688. The Works of
Thomas Sydenham, M.D. Translation from the Latin Edition of Dr. Greenhill, with
a life of the author, by R. G. Latham, M.D. Printed for the Sydenham Society,
1848, vol. i., pp. lxxii., lxxiii.
• vdkniiam's classification of small-pox. 187
111 -,omc few places, but in a mild and manageable lorm." '
" Now, the confluent small-pox is as much worse than I In: distinct, as the
plague is worse than the confluent."-
" As for the distinct sort, even if it can be seen beforehand, bed is so much
out of the question, that injunctions against it are superfluous. The scanty
number of the exanthemata makes matters safe either way." :i
" With few pustules, and those of the distinct sort, I In: treatment is
immaterial ; provided there is no gross <Tmr. The disease is a slight one. The
ignorance of 1 he physician, who aims at nothing so much as the promotion of
heat, can alone make it dangerous. I hingerous, too, it has been made ; since in
such cases 1 he doctor, though unconsciously, helps the disease."4
In referring to the treatment of small-pox, "all this applies to the confluent
small-pox only. With the distinct sort, they have nothing to do. Those who boast
about curing cases where the rash has been icanty, deceive themselves and
others. If they really wish to test their skill, let them take a confluent case
in a young subject who has drunk hard ; and not so far blunder as to fancy that,
in their easier practice, they have saved the lives of patients whom it would
have been a hard matter to have killed.""'
Other authorities testify to the mildness of some Inrms of the disease. Thus
Wagstaffc, in a letter to Dr.
1 "Medical Observations." Printed for the Sydenham Society, 1848, Mil. i., p.
160.
" Letter to Dr. Cole. JbiU., vol. ii., p. 58.
;l I It iit., p. 65. 4 Ibid., p. 71. "' Ibid., p.
79.
Freind, observes—"There is scarcely, I believe, so great a difference between
any two distempers in the world, as between the best and worst sort of
small-pox, in respect to the danger which attends them. ... So true is that
common observation, that there is one sort in which a nurse cannot kill, and
another which even a physician can never cure."1 Sir Richard Blackmore, in his
remarks on the treatment of small-pox, says :—" In the most favourable sort of
the distinct small-pox, which are few in number and mild in quality, Nature
herself, as I have before observed, is able to cure the distemper, and needs
not call the physician in aid."2 Isaac Massey, the apothecary to Christ's
Hospital, thus gives his experience:—"Here in the natural stnall-pox, hut one in
forty-nine died, and, I can assure the reader, that upon a strict review of
thirty years' business, and more, not one in forty small-pox patients of the
younger life have died, i.e., about five, and under eighteen."3 Mr. John Mudge,
a surgeon, of Plymouth, writing in 1777, says— "There is not perhaps a disease
to which the human race is exposed, that differs more from itself at different
times than the natural small-pox. We sometimes see this disorder so mild and
benign, as scarcely to expose the patient to more danger than a common cold ;
and at others, exasperated by a degree of malignity and
1A Letter to Dr. Freind showing the danger and uncertainty of inoculating the
Small-pox, pp. 9, 10. \V. Wagstaffe, M.D., F.R.S. London. 1722.
-"A Treatise upon the Small-pox," p. 42. Sir Richard Blackmore, M.D.,
F.R.C.T. London. 1723.
'"Remarks on Dr. Jurin's Last Yearly Account of the Success of Inoculation," p.
7. Isaac Massey. London. 1727.
CONFIRMED BY JENNER. 189
virulence, little, or perhaps not at all, inferior to the plague itself."1
The matter has also been alluded to by jenner. ()f course Jenner never dreamt in
the first ardour of his discovery, that the advocacy of vaccination would be
reduced to a mere plea for mitigation, and thus we obtain the following
interesting confirmation of the painstaking and carefully recorded experience of
Sydenham. " There are certainly more forms than one," he says, "without
considering the common variation between the confluent and distinct, in which
the small-pox appears in what is called the natural way.— .About seven years ago
a species of small-pox spread through many of the towns and villages of this
part of Gloucestershire: it was of so mild a nature, that a latal instance was
scarcely ever heard of, and consequently so little dreaded by the lower orders
of the community, that they scrupled not to hold the same intercourse with each
other as if no infectious disease had been present among them. I never saw nor
heard • if an instance of its being confluent."-
More recently also we have the corroboration of Mr. Marson, who says—"The
death-rate from distinct small-pox among the unvaccinated is only four per
c:i:iit., and even those four per cent, die of convulsions, <>r some other
disease to which children are liable."3
' " A Dissertation on the Inoculated Small-pox," pp. I, 2. John Mud^c,
Surgeon. London. 1777.
'"An Inquiry into the Causes and Effects of the }^arioltc Vaccina-" I
'\,\. Edward Jenner, M.I)., K.R.S. London. 1798.
'1,1. 4,,;i6, Report from the Select Comn.ittee on the Vaccination \ 1
(1S07). 1871.
And Dr. William Gayton,1 medical superintendent of the North-Western Fever
Hospital, has admitted that discrete small-pox is a comparatively mild disease
even in the unvaccinated.
Another variety of small-pox, viz., malignant or hajmorrhagic, is of a different
type. Regarding this, Dr. MacCombie2 states (i) That it is by no means rare ;
(2) that the majority of attacks occur in vaccinated persons ; and (3) that
recovery does not take place. This last statement accords with the experience of
Dr. Gayton, who informed the Royal Commission (O. 1,818), that malignant or
haemorrhagic small-pox was almost uniformly fatal whether the person had been
vaccinated or not. The following table, compiled from the hospital reports by
Mr. Wheeler,3 demonstrates this point conclusively :—
Malig nant Small-pox.
Vaccinated. Unvaccinated.
Years. Attack. Dea.h, ^W Attacks. DJh, FataH*
Homerton ... 1871-77 163 139
853 153 153 1000
Hampstead... 1S76-78 127 105
827 127 115 go'6
Fulham ... 1877-79 26 l8 (9
- 44 39 88'6
Deptford ... 1879 2I
2I 1000 jo 10 1000
DlSf°lk}l8768° '63 "3 6</3 '°3 93 9O-3 Total
... 500 396 79'2 437 410 938
1 Q. 1,816, Second Report, Royal Commission on Vaccination. '' Allbutt's
"System of Medicine," vol. ii., pp. 203, 204. London. 1S97..
3Third Report, Royal Commission on Vaccination, Appendix, p. 206 Table Q.).
VARIETIES OF SMALL-POX. 191
As vaccination apparently has no influence on this Conn of the disease, Dr.
Grieve, medical superintendent of the Hampstead Small-pox Hospital, was probably
correct when he stated that it was " but too common in people who had lived in
defiance of all sanitary laws, or who by intemperance have debilitated their
constitutions."1
Another particularly fatal, but rare variety, termed corymbose small-pox, has
been observed. This was described by Mr. Marson 2 as presenting" two or
three-patches or clusters about the size of the palm of a hand, upon which the
eruption is as thickly set as it possibly can be, while the skin around for some
distance is almost, if not entirely free. Mr. Marson gives the figures for 104
cases of this variety, which came under his observation : 29 were unvaccinated,
of these 13 or 44'8 per cent, died ; and 74 were vaccinated, of which 32 or 43'2
per cent. died. Thus, the fatality in the two classes of this variety of the
disease, is practically identical.
The only remaining type of the disease for us to consider is the confluent, and
from the above it will be evident that the huge difference in the rates of the
vaccinated and unvaccinated must take place in cases of this description. In
this variety of the disease, the pustules coalesce, so as to render the features
hardly recognisable, and it can easily be understood that marks of vaccination
may be and are readily obscured, so that
1 "An Analysis of 800 cases of Small-pox." The Lancet, March 18, 1S71, vol. i.,
p. 371.
2Article on "Small-pox," by Mr. J. F. Marson. Reynolds'" System c>[ Medicine,"
vol. i., p. 438. London. 1866.
it is impossible to determine from an examination of the arm whether they exist
or not.
This difficulty has been recognised by the leading authorities. Thus, Dr.
Gregory says—" Great difficulties were necessarily experienced in determining
who had been really vaccinated, of those who assumed to have undergone that
process. The cicatrix was our chief guide, but this often failed us, from the
swollen and pock-covered condition of the arm at the time of the patient's
admission."1 Dr. James B. Russell remarks— " Sometimes persons were said to be
vaccinated, but no marks could be seen, very frequently because of the abundance
of the eruption. In some of those cases which recovered, an inspection before
dismissal discovered vaccine marks, sometimes ' very good.' Those who died, or
who were not so examined, are placed in a separate column as ' said to be
vaccinated, but V.M. not visible.' I do not observe in the reports on smallpox,
as observed in London and Dublin, any allusion to this difficulty. Even the best
vaccine mark is readily obscured, or even hidden, by a copious eruption, and
unless such special means, as I have described, are adopted, it is impossible
accurately to ascertain the facts of small-pox in the vaccinated."2
Not only may the scars be obscured by eruption, but there is no doubt also that
they may wear out. Dr. George Gregory says—" The absence of a cicatrix is not
decisive against either the present or prior existence of vaccine energy in the
system, because in many cases,
1 " Medico Chirurgical Transactions," vol. xxii., p. 97. 1S39.
2 Glasgow Medical Journal, vol. v., p. 6 (November, 1872).
CLASSIFICATION OF SMALL-POX PATIENTS. 193
the specific inflammation is moderate, and the resulting ■.car wears out in the
progress of life, as other scars do which are not the result of a specific
poison."1 In his " Observations on the Variola Vaccines'' Mr. Robert Ceely, of
Aylesbury, says—" Inspection of many scars, caused by this lymph, shows that in
a few months little is to be learned in many subjects, with thin skins, of the
degree to which the vaccine influence has been exerted on them."2
A Committee appointed by the Epidemiological Society (Epidem. Soc. Trans., vol.
v., p. 153, 1885-86) recognised that " not every cicatrix which is once Ibveated
will always retain its condition of foveation, and, further, that not every
cicatrix will permanently exist." Dr. Savill in his report on the Warrington
outbreak has also called attention to the fact that vaccination scars tend to
become obliterated with age, and to alter in character with time.3
Let us now see what has been the practice with regard to the classification of
small - pox patients. Mr. Francis Vachcr, Medical Officer of Health for
Birkenhead, candidly observes—" The mere assertions of patients or their
friends, that they were vaccinated, counted for nothing, as about 80 per cent,
of the patients entered in the third column of the table ('unknown') were
reported as having been vaccinated in infancy."4 Mr. Marson informs
us—"Patients were
1 London Medical Gazette, vol. xxv., pp. 289, 290 (November 15, 1839).
'-'"Transactions of the Provincial Medical and Surgical Association/' vol.
viii., p. 416, foot-note. 1840.
:> Final Report, Royal Commission on Vaccination, Appendix v., p. 42 4 "Notes on
the Small-pox Epidemic at Birkenhead in 1877," p. 9.
never entered in the register as vaccinated, unless the account of the
vaccination was a tolerably clear one."1 And Dr. William Gayton, in the Homerton
Report for 1875, observes (p. 58)—"I have always classed as ' vaccinated' those
upon whom any mark supposed to result from vaccination has existed, and as '
unvac-cinated' when no scar presumably arising from the effects of vaccine lymph
could be discovered. Individuals are constantly seen who state that they have
been vaccinated, but upon whom no cicatrices of any description can be traced.
In a prognostic and statistic point of view it is better, and, I think,
necessary, to class them as unvaccinated."
The fallacies of this method of classification have been pointed out by Dr.
Rirdwood and Dr. Ricketts.
Dr. Birdwood, with an experience of twelve thousand cases of small-pox, stated,
before the Royal Commission, that in his opinion the evidence of primary
vaccination, collected in small-pox hospitals, should not be relied on.
Because—
"(1) On the outbreak of an epidemic there is necessarily much administrative
confusion, and many untrained observers. The early observations are incomplete
and faulty.
"(2) In the worst instances the eruption may be sufficient to, and does obscure
the scars.
" (3) The statement of parents as to primary vaccination, and of adult patients
as to re-vaccination, should be accepted even when scars are not seen.
1 " Medico-Chirurgical Transactions," vol. xxxvi., p. 374. 1853.
2 Sixth Report, Royal Commission on Vaccination. Q. 31,221.
DRS. UIRDWOOD AND RICKETTS' EVIDENCE. 195
"(4) Scars produced in infancy grow with the growth of the body ; as was pointed
out, I understand, by Sir James l'aget.
"(5) In such statistics insufficient allowance is made for other circumstances,
such as occupation, intemperance, and the existence of other diseases. An
altogether different death-rate might be anticipated if small-pox broke out in a
public school, or in the infirm and aged wards of a workhouse. A typhoid fever
patient, or an ill-fed baby, catching discrete small-pox and dying, would be
counted a death from small-pox, obviously neither vaccination nor its neglect
having anything to do with it.
"(6) The accurate observation and record of clinical details is one of the most
difficult duties required of medical men employed in hospitals for infectious
disease."
Dr. Ricketts says—"In some of the earlier statistics on vaccination only two
classes of cases were considered, viz., those vaccinated and those unvaccinated
; apparently the only evidence as to vaccination that was accepted being the
presence or absence of scars. An absolute reliance, however, ought not to be
placed on this evidence. There is no doubt that cases occur in which vaccination
has been successfully performed, although cicatrices are not present when the
attack of small-pox supervenes. There is a small class, too, but naturally a
very fatal class, in which the rash is too abundant over the upper part of the
arm for an assertion to be made that scars are absent." On Table
1 Report of the Metropolitan Asylums Board for 1893, p. 136.
H, pp. 144, 145, he gives twenty-six cases, with thirteen deaths, in which the
absence of scars could not be asserted because of the abundant eruption ; and in
twenty-five of these, the patient was stated to have been vaccinated.
Let us see how Dr. Ricketts' figures work out. On Table 11.c, pp. 185-188 of the
same report, there arc forty-two vaccinated deaths, and forty-four in which
there is "no evidence" as to cicatrices. On p. 138, he describes an
age-distribution he has made of the " no evidence" cases. He puts it in the form
of a diagram, and on comparing it with similar diagrams for the vaccinated and
for cases in which the vaccination cicatrix was " absent," he finds that the
diagram corresponds much more nearly with the former than the latter. There were
ninety-four deaths in which the vaccination cicatrix was " absent," but it will
be noticed that forty-four of these are in the first three years of life, in
which there are no cases or deaths in the other two classes. In all fairness
these should be therefore struck off; we then get fifty deaths in this class,
and if we add the " no evidence" deaths to the vaccinated (I am aware that I am
slightly overstating the case), we have eighty-six vaccinated deaths, and fifty
in which the cicatrix was " absent." Thus, over three years of age, there are,
if we include the " no evidence " cases with the vaccinated, 6y2 per cent, of
the deaths vaccinated.
But there are further allowances to be made, for on p. 134, Dr. Ricketts says of
his class, in which the vaccination cicatrix was " absent," that he is not able
to describe these cases as all " admittedly unvac-
SOURCES OF FALLACY. 197
cinated." Another source of fallacy is pointed out in the British Medical
Journal of October 23, 1880 (vol. ii., p. 672). The editor says—" It is probable
that a larger proportion of unvaccinatcd persons is to be found among the
ignorant, dirty, and wretched inhabitants of the slums of London, and very few
indeed among the educated and better fed members of society," And Dr. Gayton
admitted before the Royal Commission (Q. 1,843) tnat this would be likely to
operate detrimentally by way of raising the unvaccinated mortality. This
applies to all places vaccinated up to the usual average. When allowance is made
for these fallacies, it will be found that the proportion of deaths vaccinated
will not be very largely different from that of the vaccinated population, which
in London, from the amount of default that has taken place in recent years,
would not be very high.
It is only fair to mention that other reports agree in not assigning such a
large proportion of deaths to the unvaccinated. In the Glasgow Medical Journal
of November, 1872 (vol. v., p. 12), Dr. Russell classifies his cases according
to the eruption. He found that in discrete cases the fatality in both classes
was nil, and in confluent small-pox the fatality of the vaccinated exceeded
that of the unvaccinated. Thus, among seventy-one vaccinated confluent cases
there were forty-nine deaths, or a fatality of 6g per cent., and of one hundred
and sixteen unvaccinated confluent cases, sixty-four, or 55^2 per cent., died.
But the most striking figures come from Prussia, and they show that up to ten
years of age there is practically no difference in the fatality in
the two
classes. The following table gives the figures for Berlin ' in the 1871-72
epidemic:—
Vaccinated. Unvaccinnted.
Age. Cases. Deaths. "^ ^Ca^ Dea.hT^f
o- j 259 136 52-5 977 570 58-3
2- 5 J>244 437 35'' ',359 564 41 "5
6-10 737 163 22T 251 77 307
If the difference between 52 and 58 per cent, is all the mitigation that can be
fairly claimed on behalf of vaccination within a year of the operation, even the
most enthusiastic champions of vaccination will ;:gree that we must look to
other and more scientific methods for the extirpation of small-pox.
To recapitulate the facts briefly :—Figures have been put forward showing an
enormous difference in the rates of the vaccinated and unvaccinated. It has been
shown that these are open to suspicion, because the rates in the unvaccinated
considerably exceed those of the last century before vaccination was discovered.
When we come to analyse them, we find that the disparity obtains principally in
cases of confluent smallpox, in which, according to the leading authorities,
the vaccination marks are readily obscured ; and when it is remembered that it
has been the practice to classify the cases according to marks, whether
discernible or not, it is evident that the results have been largely fallacious.
Other sources of fallacy are the different conditions under which the two
classes labour, and also the age. Of course, when the different ages are
separated as
1 " Beitrage zur Beurtheilung des Nutzens der Schutzpockenimpfung," p. 168.
Berlin. 1888.
INVESTIGATION BY THE REGISTRAR-GENERAL. 199
in the reports of the Metropolitan Asylums Board, this objection would not hold,
but in the majority of instances, all ages are taken together, or separated only
into those under and over ten ; and considering that the unvaccinated more
largely consist of young infants, who normally have a high small-pox fatality,
this method naturally raises the rates for this class.
The Government returns of small-pox deaths would appear to be one way of
settling the question, but here we are met with the difficulty that in
death-certificates of cases of small-pox, medical men in a large proportion of
instances make no statement about the vaccination, although they have been
repeatedly urged to do so by the Registrar-General, and also by the medical
press. In England and Wales, in 1892-95, there were 2,931 deaths from small-pox,
of which 391, or 13-3 per cent., are reported in the vaccinated ; 596, or 2O'3
per cent., in the unvaccinated; whereas, in (,944, or 66'3 per cent, of the
whole, there is no statement as to whether the patient was vaccinated or not.
The following from the British Medical Journal of March 17, 1877 (vol. i., p.
330), appears to throw some light on the matter :—" It may not be generally
known that the Registrar-General, during the epidemic of smallpox in London in
1871-72, attempted to obtain more complete information as to the vaccination of
persons dying of small-pox than was furnished in medical certificates. Then, as
now, no information as to vaccination was given in a large proportion of
medical certificates.
" The Registrar-General, therefore, requested the local registrars, in cases
where the medical certificate was
silent on the point, to endeavour to ascertain from the informants of the deaths
(almost invariably relatives), and to insert in the Register, whether the
deceased had or had not been vaccinated.
"Information derived in this way certainly yielded results very similar to those
obtained by the anti-vaccinationists themselves; relatives almost invariably
asserted that the deceased had been vaccinated ; but, as inquiries of the
medical attendants in a large number of these ' not stated ' cases elicited the
fact that the deceased, the statements of relatives notwithstanding, bore no
marks of vaccination, registrars were subsequently instructed to insert in the
Register no facts as to vaccination unless certified under the hand of a
registered medical practitioner."
It need hardly be said that this inquiry of the Registrar-General is very
important. In these " not stated " deaths, the medical men presumably are unable
to decide the fact of vaccination. The difficulty no doubt is great, for as Dr.
Savill has pointed out in his report on the Warrington epidemic, " in nearly all
fatal cases the eruption is profuse and tends to hide the vaccination scars if
they exist."1 Dr. Birdwood, as I have shown, is also alive to the difficulty,
and recommends that the statements of parents as to primary vaccination should
be accepted. The relatives in the cases I am referring to almost invariably
asserted that the patients had been vaccinated, and thus I cannot help thinking
that the most important part of the case for vaccination has been given away,
for if in the recent
1 Final Report, Royal Commission on Vaccination, Appendix v., p. 34.
CLASSIFICATION BY MARKS. 2OI
epidemic (1892-95), we add the "not stated" cases to the vaccinated, nearly 80
per cent, of the total deaths from small-pox will be found in the vaccinated
class.
It seems a pity that the vaccinal condition of patients suffering from small-pox
has not more often been determined by reference to the vaccination register.
Dr. Birdwood informed the Royal Commission (O. 31,250-51) that the Metropolitan
Asylums Board used to forward a list of patients to the Local Government Board
for this purpose, but that he knew of no published results of their inquiries.
If the Local Government Board would undertake investigations of this nature,
they would doubtless receive the cordial co-operation of both parties in the
vaccination controversy, and the results would prove interesting, if not
instructive.
It has been urged that the protection afforded by vaccination is in proportion
to the number and the quality of the marks. In the first place, cicatrices
resulting from the same lymph of good quality vary considerably. They may be
smooth, striated, puckered, pitted, and so on; in fact, a French observer,
Decanteleu, has figured no less than seventy different varieties of scars.1 Dr.
Savill points out that " the foveation of vaccination scars does but follow the
same laws which govern other lesions involving only the superficial layers of
the skin;"2 and he figures the arm of a girl to show
1 Professor Crookshank's Evidence. Fourth Report, Royal Commission .hi
Vaccination. Q. 11,892.
"Final Report, Royal Commission on Vaccination, Appendix v., l>. 42.
the similarity of foveate texture in a scar resulting from a superficial burn on
the shoulder, and in some primary vaccination cicatrices. Thus, it would appear
that the texture of the vaccination cicatrix depends on the amount of the local
inflammation, on the method of performing the operation, on the age,
surroundings, and general health of the individual, and on other factors.
It is also worthy of notice that in classifying cases of small-pox according to
vaccination marks, different methods are adopted by different observers. Thus
Dr. Gayton informed the Royal Commission (Q. 1,700-06) that when he found one
good mark and three imperfect ones, he might class them as a case of two good
marks, or he would ignore the three imperfect marks, and class the case as one
of a single good mark. Of 10,403 cases of small-pox admitted to the hospitals of
the Metropolitan Asylums Board during 1870-84, Dr. Gayton1 classified 2,085, or
2O Per cent., as "vaccinated with good marks ;" whereas, at another hospital of
the same Board, during the years 1880-85, Dr. Sweeting2 placed only 39 out of
2,584, or i-5 per cent., in the category of " good vaccination." The Dissentient
Commissioners, Dr. Collins and Mr. Picton, observe (Section 129)—"It is evident
that such a difference indicates a wide margin for personal discrimination as to
what is and what is not 'good vaccination.'" It is, therefore, not altogether
surprising to learn, on the authority of Dr. M. D. Makuna, when medical
superintendent of the Fulham
' Second Report, Royal Commission on Vaccination, Appendix, p. 245. 2 Ibid.
Q. 3,689.
" GOOD " AND " BAD " MARKS. 2O3
Small-pox Hospital, that "what one will call an indifferent mark, another will
call fair, a third moderate, and a fourth bad, and so on, till the confusion is
worst confounded."1
The following testimonies appear to show that even " good vaccination " is far
from securing a perfect immunity against small-pox. Thus, Dr. J. J. Bigsby, in
an epidemic of small-pox at Newark, found that "some 1 >f the worst cases (of
small-pox) had remarkably good ■.cars."2 In the British Medical Journal of April
1, 1871, Ur. Atthill is reported to have stated that "he <lid not think that a
good mark insured protection more than an ill-defined one."s
Dr. B. Browning, medical officer of health to Rother-hithe, gives particulars of
469 cases of post-vaccinal small-pox, of which 100, or 2i"3 per cent., died.
"Many of these sufferers," he says, "showed good vaccine marks of the kind that
would be deemed worthy of an extra grant from the Government Inspector (at least
I used formerly to receive such ".rants for doing similar looking work), and yet
the)' look small-pox—some within six days, some within ,ix months, and some
within six years of their vaccination date."4 And lastly, I may quote the
valuable ustimony of Dr. John MacCombie, who, on June 12, 1 .S78, stated before
the Epidemiological Society that " the evidence afforded by the
cases admitted into
I Report of the Fulham Small-pox Hospital for the year 1878, pp. 11, 12.
" London Medical Gazette, Sept. 28, 1839, vol. xxv., p. 18.
II British Medical Journal, April I, 1871, vol. i., p. 352.
4 Transactions of the Society of Medical Officers of Health (Session 1SS1-82),
p. 29.
the Asylum Boards Hospitals goes to show that the good and bad marks are equally
protective against attacks of small-pox,"1 and he further remarks that "good
vaccination protects absolutely against no form of small-pox."2
In considering the theory that the protection is in proportion to the number of
marks, it may be mentioned that, if we are to be guided by jenner, "a single
cow-pox pustule is all that is necessary."3 But this, as well as other theories
promulgated by Jenner, has been discarded, and the orthodox number of marks at
the present time is four. It is not pretended that this theory has any
scientific basis, but it appears to rest mainly on certain figures compiled by
Mr. Marson,4 surgeon to the London Small-pox Hospital. The results he obtained
are given in the following tables :—
Cases. Deaths. »T
Unvaccinated ... ... 2,883 1,006 3489
Vaccinated (no scars) ... 259 102 39'38
Vaccinated (scars) ... 10,293 685 666
1 scar ............................... 2,584 357 1382
2 scars ... ... ... 3,138 242 771
3 scars ... ... ... 2 139 65 3'O4
4 scars ... ... ... 2,432 21 '86
1 Paper on "Comparison of Small-pox Statistics, Epidemics 1871 and 1876," by
John MacCombic, M.A., M.B., Medical Superintendent to the Deptford Small-pox
Hospital. Transactions of the Epidemiological Society (Sessions 1877-78 and
1878-79), vol. iv., part 2, p. 190.
''■Ibid., p. 192.
3 11 Further Observations on the Variolif VaccimE, or Cow-pox," p. 38,
London. 1799-
4 Pages 236, 237, Report from the Select Committee on the Vaccination
Act (1867). 1871.
MR. MARSON'S STATISTICS. 205
Indifferent scars. Good scars.
..... ■»• ^e., ^ath,"^? C^es. Death, W
1 1,530 328 21-44 1,054 29 275
.! 1,838 224 I2'I9 I,3OO 18 I 38
3 1,151 55 478 988 10 roi
4 1,179 2O '7° 1,253 1 08
I'olal ... 5,698 627 iroo 4,595 58 1 26
I" obtain the above figures, Mr. Marson deducted I' illis for
superadded disease, thus :—
Total Deaths Percentage of
(Uaths. .deducted, deaths deducted.
Unvaccinated ... ',043 yj 35
Vaccinated (scars)... 790 105 133
Indifferent scars. Good scars.
„„ „ Total Deaths Pefr^enSge Total Deaths
Pefr?n'?,g<;
Sc™- deaths. deducted, fj^ deaths, deducted. °<J^
1 353 25 7-1 34 5
147
2 252 28 hi 24 6 25'o
3 65 10 15-4 14 4
286
4 37 17 45 9 'I i° 909
Total ... 707 80 113 83 25 30'y
This shows that he deducted a larger proportion of deaths for the vaccinated
than for the unvaccinated, lor good scars than for indifferent scars, a larger
proportion for two scars than one scar, for three scars than two scars, and for
four scars than three scars, I he climax being reached with four good scars, in
which class, with eleven deaths altogether, he deducted Irn before making his
calculations, and these, forsooth, •ire the figures on which the notorious marks
theory l<ii|;dy depends !
Mr. P. M. Davidson, the medical officer of health to Congleton, has drawn
attention to the strange conclusions to which we should be driven were we to
accept some of the figures in Dr. Barry's Sheffield Report. Table cxiv. (p. 212)
shows the fatality and type of disease with one, two, three, and four or more
scars in cases treated at the Borough Hospital, Winter Street.
Under 20 years of ace. Above 20 years of age.
C^ion.tO Cases. Death,. Ł»g C^T^hs. »
No visible primary \
cicatrix, or 1 cica-r 22 o 00 73 13 178
trix only ... ...I
2 primary cicatrices 94 3 32 165 21
127
3 primary cicatrices 187 3 1 6 185 18 97
4 or more primaryl
, .
. . I 67 O
O-O 32 2 6 2
cicatrices ... ___ 1
With regard to the type of disease under twenty years of age, there was one
confluent case, and that had four marks. The only conclusion to be deduced from
these figures is, that under twenty years of age, no visible mark, or one mark
only, secures the greatest immunity from death and severe disease; whereas when
a person reaches the age of twenty and upwards, one-mark cases have the greatest
fatality, the fatality gradually diminishing with two, three, and four marks,
and thus twenty years must elapse before the influence of plurality of marks
comes into play. Dr. Barry surely did not intend us to believe that this was the
case, but it is unquestionably what his figures tend to show. Again in Table
CXV. (p. 214), Dr. Barry gives statistics for the Ecclesall Bierlow Union
Workhouse Hospital at all ages, as follows :—
mr. Davidson's cases. 207
Scars. Attacks. Deaths. Fatality
per cent.
1 or 2 14 7 500
3 or more 118 2 17
These percentages are seriously set forth to show the alarming difference in
fatality between one or two and three or more marks, Dr. Barry and those who
supplied him with the statistics apparently forgetting that the fatality he
gives for one or two marks is nearly three times the average fatality of the
unvaccinated in the Last century, and even much larger than the figures lie
himself gives for his own unvaccinated class, and if they show anything at all
they show that the one-mark vaccination which was fashionable during the first
half of the century was provocative of a fatal issue if attacked, and that most
of the private vaccination at the present time is in the same plight, and that
Mr. Krnest Hart is giving the best of advice when he says— " Better by far let
such applicants (for one or two small insertions) depart with their children
unvaccinated than place them in a state of false security."1
Mr. P. M. Davidson, besides criticising Dr. Barry's figures, has given us the
result of his own painstaking and valuable experience of a small outbreak he had
to deal with at Congleton, and the following has been extracted from a table he
gives of these cases, on l>. 27 of his report.2
1 AUbuH's " System of Medicine," vol. ii., p. 676. London. 1897. 1 Special
Report on the Recent Outbreak of Small-pox in Congleton.
Xo. Name.
Age. Results of
vaccination. Character
of small-pox.
1 George T. - 18 Five deeply pitted scars, one and one-
Semi-confluent, severe, numerous pits.
third square inch in
area.
j
2 Henry B. - 43 One superficial scar, one-third square
Discrete, very mild, no pitting; worked
inch in area. throughout
illness.
3 George W. - 26 Three scars (one deeply pitted, two
Semi-confluent, very few pits.
pitted), one and one-quarter square inch in area.
4 Emma B. - 40 Two superficial scars, two-thirds square
Discrete, very mild, no pitting; had only
inch in area. about twenty spots
; never in bed.
5 Annie S. - - 25 Four scars (two pitted, two
superficial), Discrete, very mild, no pitting.
one-half square inch in area.
6 Randel B. - 32 Four scars (three deeply pitted, one
Confluent, severe, pitted deeply, exten-
pitted), two-thirds square inch in area. sively, and permanently ; face
completely covered.
7 Harry B. - - 26 I Eight scars (two pitted, six
superficial), Confluent, pitted considerably.
one square inch in area. j
8 John P. - - 19 I Two deeply pitted scars,
one-third Confluent, extensively and permanently
j square inch in area. pitted.
9 Daniel C. - 27 Three scars (one pitted, two
superficial), Discrete, very mild, no pitting.
one-fifth square inch in area. I
10 James C. - - 20 Four scars (two deeply pitted,
one Discrete, some pitting.
pitted, one superficial), three-quarters square inch in area.
j 11 John C. - - 19 Four scars (two deeply pitted, one
pit- J Confluent, seveie, much pitted.
ted, one superficial), one square inch in area.
12 William T. - 25 Four pitted scars, one-third
square Discrete, a few slight pits.
inch in area. 1
13 Thomas S. - 55 Three scars (one deeply pitted, one
Semi-confluent, slightly pitted.
pitted, one superficial), one-third square inch in area.
14 Annie P. - - 18 Threescars(onedeeply pitted,two
super- Discrete, very mild, two or three pits.
; ficial), four-fifths square inch in area.
15 Mrs. C. - - 43 Two deeply pitted scars, three-quarters
Discrete, severe, slightly pitted.
square inch in area.
16 Margaret T. -| 40 I Four deeply pitted scars, three-quarters
Confluent, haemorrhagic, pitted exten-
| ' : square inch in
area. sively ; the most severe
case.
j 17 Sarah A. - - 27 One deeply pitted scar, one-third
square Discrete, very mild, no pitting; mildest !
inch in area. of all except Cases
2 and 4.
1______________________________________________
Thus five of the cases (Nos. 6, 7, 8, 11, and 16) were confluent, three
semi-confluent (Nos. 1, 3, and 13), and nine discrete (Nos. 2, 4, 5, 9, lo, 12,
14, 15, and 17). All the confluent cases, except No. 7, had well-pitted
vaccination scars. One of them (No. 7) had eight scars, three (Nos. 6, 11, and
16) had four scars, and the remaining one (No. 8) two scars ; the average number
of scars being four and one half, and the average superficial area three
quarters of a square inch.
Of the three semi-confluent cases, No. 1 had five scars, and this was the most
severe ; and the remaining two (Nos. 3 and 13) had three scars each ; the
average number of scars being three and two thirds, and the average superficial
area one square inch.
Of the nine discrete cases, three (Nos. 5, 10, and 12) had four scars, two (Nos.
9 and 14) three scars, two (Nos. 4 and 15) two scars, and the remaining two
(Nos. 2 and 17) one scar each ; the average number of scars being two and two
thirds, and the average superficial area one half of a square inch. The
following table gives a summary :—
Average number Average superficial area,
of scars. in square inches.
5 confluent cases ... ... 4^ ... f
3 semi-confluent cases ... 3| ... I
9 discrete cases ... ... 2-| ... \
Mr. Davidson adds (p. 15)—"Comment on this is superfluous, and I leave it to
anyone caring to consider the matter to judge for himself what he is to expect
from scars and superficial areas in this part of the country. If they teach
anything, it is that the more you have of them, and the larger and deeper they
are, the more severe will be your small-pox."
THK SHEFFIELD EXPERIENCE. 211
The best way to test the question is to compare the incidence of small-pox
following vaccination by public and private practitioners, for the public
vaccinators are bound by their regulations to work up to a certain standard. In
the Sheffield epidemic (1887-88J it was found that 358, or 70/4 per cent., of
the 451 vaccinated cases of small-pox under ten years of age had been
vaccinated by public vaccinators, who had only performed 63 per cent, of the
successful primary vaccinations for the ten-year period up to the epidemic;1
hence it follows that small-pox picked out the work of the public vaccinators,
whose skilful and successful performances had qualified each operator for a
Government grant. Again, Sheffield Park, North Sheffield, and West
Sheffield—the districts of the borough which were the most seriously afflicted
with small-pox—had the largest percentage of their successful primary
vaccinations, for the ten years previous to the epidemic, performed by public
vaccinators; whereas Ecclesall and Upper Hallam, with the smallest percentage,
came off the lightest of all the districts of Sheffield.
The large proportion of three or four-mark cases of small-pox in very
efficiently vaccinated towns, as in the case of Willenhall, strongly condemns
the theory. Of the 681 vaccinated persons attacked in which the number of scars
was known, 374, or 54P per cent., had four marks, and 536, or 787 per cent., had
three or four marks, while the one-mark cases only amounted to 24, or 3'5 per
cent, of the whole.
1 Report on an Epidemic of Small-pox at Sheffield (1887-88), pp. 185, 187 ;
Tables xcvii., xcix.
Before concluding the chapter, the opinion of Dr. George Gregory, the
distinguished predecessor of Mr. Marson at the London Small-pox Hospital, is
worth recording. In the twenty-fourth volume of the Mcdico-Chirurgical
Transactions (1841, pp. 23, 24), after detailing several cases, he says :—" It
follows, I think, from these cases, that the cicatrix cannot be relied on as
affording any certain test of the degree to which the constitution has imbibed
an anti-variolous influence."
Another authority (Dr. Fleetwood Churchill) observes :—" For some years I have
only made one (puncture), on account of the severe inflammation which sometimes
results from two or more, nor have I had any reason to suppose that my object
was not as completely attained."1
The more recent authorities also deprecate the " mark theory." Thus, Dr.
Birdwood observes that, in regard to primary vaccination, he advocates " the
production of one vaccine vesicle only;"2 and Dr. Ricketts writes— " Considering
that scars vary in size and in appearance in the course of years, and that
vaccinia must be regarded as a specific fever, it is not at first sight apparent
what the characteristics of the inoculation cicatrices have to do with the
amount of protection afforded. But, after all, it is a question of fact, which,
provided proper observations are made, ought to be, and can be settled in course
of time by such statistics."8
ll'The Diseases of Children," p. 821. Third edition. Kleetwood Churchill,
M.D. Dublin. 1870.
-Sixth Report, Royal Commission on Vaccination. (,). 31,22!. 3 Report of the
Metropolitan Asylums Board for 1893, p. 134.
DR. COUPLAND'S FIGURES. 213
Some observers, besides those already mentioned, obtained equivocal results. Dr.
Dalton1 gives the following experiences :—
Marks. Cases. Fatality per cent.
1 126 2'4
2 171 5"3
3 177 2-8
4 140 07
5 or more 93 2'2
Also Dr. Coupland,2 who gives the following for the Dewsbury epidemic:—
Ma'ks. Cases. Deaths.
Fatality per cent.
1 34 O OO
2 175
IO 57
3 210
o o'o
4 or more 42
1 2'4
There is thus very slender evidence to show that the protection depends upon the
number or character of marks, and the little that exists is mainly afforded by
the earlier statistics, such as Marson's, which it is obvious are inaccurately
founded.
From the foregoing facts it is evident that the mitigation attributed to
vaccination depends largely upon the elimination of cases from the vaccinated
lists, rather than to any real modification of the disease, and this is borne
out by the fact that the fatality of smallpox in 1871-72, when a large
proportion of the cases were admittedly vaccinated, was as great as the average
fatality of the last century.
1 " Small-pox in its Relation to Vaccination," p. 23. J. 11. C. Dalton,
M.A., M.D., B.C. (Reprinted from the Medical Chronicle, October, 1893.)
-Final Report, Royal Commission on Vaccination, Appendix iii., p. 11q.
CHAPTER VII.
RE-VACCINATION.
THE admission that re-vaccination is necessary, is a departure from the original
position taken up by the profession. It was not only Jenner who was so positive
about the lifelong protection afforded by vaccination, but his opinion has been
endorsed by the highest authorities at a later period. Sir John Simon says :— "
On the conclusion of this artificial disorder (vaccination), neither renewed
vaccination, nor inoculation with small-pox, nor the closest contact and
cohabitation with small-pox patients, will occasion him (the vaccinated person)
to betray any remnant of susceptibility to infection."1
When this theory, upon which all vaccination legislation was initiated and
justified, was discovered untenable, that of re-vaccination was introduced.
Instances of both mild and severe attacks of smallpox taking place at all
periods after re-vaccination are numerous. I propose to give a few of these. Mr.
Badcock, the celebrated small-pox cow-pox vaccin-ator, relates his own
personal experience: " Towards
1 " Papers relating to the History and Practice of Vaccination,'' p. xiv. 1857.
KAMA)RE OF TRIPLE VACCINATION. 21 5
the end of the year 1836, I suffered severely from a dangerous attack of
small-pox, which happened but ;i few months after re-vaccination."1 We also have
the experience of Mr. Justice Grantham :—"Pie impressed on the anti-vaccinators
the peril they were incurring to themselves and their neighbours by their
opposition to inoculation, and in support of his arguments as to the effect of
vaccination, stated that he, after having been twice inoculated, had an almost
miraculous recovery from an attack of small - pox, which, in its incipient
stages, was as bad as it could be."2
The following case shows the complete failure of three successful vaccinations
to prevent a severe attack of small-pox. It is recorded by Dr. T. C. Wallace in
the American Medical Times of March 1, 1862 (vol. iv., p. 122). The patient,
Charles Nichols, aged thirty-five, had an " extraordinarily severe" attack of
confluent small-pox, and Dr. Wallace observed that he had never seen anyone so
completely covered with pustules. The man had a large scar on the right arm,
resulting, he informed Dr. Wallace, from vaccination when a child, and a similar
one on the left arm, due to vaccination three years prior to attack. He was
again vaccinated on the 24th of December, 1861, the vesicle being " fully
formed, large, and well filled," the vaccination being accompanied by some
slight constitutional symptoms. He was attacked with small-pox
' "A Detail of Experiments confirming the power of Cow-pox, etc.," |i. 11.
John Badcock, Chemist. Brighton. 1845. * Sussex Daily News, April 9,
1896.
on the 8th of January, 1862, just fifteen days after the third
vaccination.
The British Medical Journal of December 7, 1872 (vol. ii., p. 643), reports a
meeting of the Medical Society of the College of Physicians in Ireland, when Dr.
Darby furnished statistics of small-pox cases treated in the Rathdown Union
Hospital ; thirteen of the cases were re-vaccinated, with one death. At the same
meeting, Dr. Grimshaw alluded to three re-vaccinated cases of small-pox admitted
to the Cork Street Hospital, one of which was fatal.
In a letter to the British Medical Journal of December 9, 1876 (vol. ii., p.
774), Mr. R. G. Kellett wrote that, during an epidemic at Bilston,
Staffordshire, in 1871-72, he re-vaccinated himself, his wife, and his two
servants. Although the vaccination took well in all, each in turn developed
small-pox, "certainly of a most abortive form, not more than a dozen spots or so
appearing on any of us, but still it was small-pox."
The same journal1 also reports some cases of smallpox, which came under the
observation of the Health Department of Brooklyn, the statistics being furnished
to the Brooklyn Eagle, by Dr. J. H. Raymond, the Health Commissioner. Among
these is that of a child, aged three, who died of small-pox notwithstanding that
she had been well vaccinated in infancy and once later.
In the Homerton Hospital Report for 1878 (pp. 23-25), Dr. Gayton gives six cases
of small-pox after re-vaccination, with the following particulars :—
1 British Medical Journal, May 20, 1882, vol. i., p. 749.
DR. GAYTON'S CASES. 217
1. "Kate King, aged twenty, admitted February 18,
1878, three imperfect marks; eruption very discrete;
was placed on 'Full Diet' February 22, 1878, and dis
charged March 14, 1878. The re-vaccination was
stated to have been performed five years ago, with
success. The patient did not remember upon which
arm it was done, therefore the cicatrices observed
may have been due to either the primary or the
secondary operation, as no others were visible."
2. "John Wist, aged twenty-seven, two good marks ;
admitted March 7, 1878, with discrete small - pox.
The patient reported that he had been vaccinated
three times in the course of his life; the first in
infancy, the operation succeeding; the second at the
time of joining the Metropolitan Police, at twenty-two
years of age, and that this took ' very slight;' the
third and last time, six months before becoming a
patient, by a medical man in Whitechapel, but without
effect. He was also positive that the two cicatrices
seen upon the left arm were the result of the primary
operation, as the sore left by the secondary one soon
healed up and left no marks."
3. " Samuel Fish, aged twenty-three, admitted March
21, 1878, three imperfect marks; eruption confluent,
general symptoms very severe. Discharged cured June
17, 1878. Was vaccinated in infancy, and again when
ten years old. The certificate of re-vaccination in this
case was produced, but it could not be satisfactorily
determined to which operation the cicatrices were to
l>e attributed."
4. "James Connelly, aged thirty-nine ; admitted
March 30, 1878, with five marks, three good and two
15
imperfect, the eruption being discrete. He was put on 'Full Diet' on April i,
and transferred April 13, 1878. The patient, an old soldier, stated that he was
re-vaccinated when in India about four years ago, and that the operation was
very successful. There were three well foveated cicatrices close together, the
extent of surface being about the size of a shilling."
5. " Ellen Clark, aged twenty-one, with one imperfect
mark, admitted April 10, 1878, with small-pox of the
haemorrhagic form, and died April 12, 1878, was said to
have been re-vaccinated, and arm to have been slightly
sore for three or four days, but no cicatrix, except the
one referred to, could be traced."
6. " E. Williams, aged three years, admitted April 25,
1878 ; eruption discrete. On April 27 had ordinary-
diet, and on May 18 discharged ; was stated by parents
to have been ' vaccinated when an infant,' one imperfect
mark being now visible as the result. Six weeks ago,
in consequence of small-pox having occurred in the
house, she was again vaccinated in four places, all of
which were attended, apparently, by some result. The
marks seen, reddish-brown in colour, were small in size,
and not indented."
In the Deptford Report for the period from April, 1878, to December, 1879, Dr.
John MacCombie details the following experience (pp. 7, 8) :—
1. "William W., cet. nineteen; admitted May 13,
1878. Three imperfect marks of primary vaccination ;
re-vaccinated cet. sixteen, two re-vaccination marks ;
discrete attack ; discharged June 10."
2. "Matilda B., cet. twenty; admitted May 31, 1878.
Two imperfect marks of primary vaccination ; re-
DR. MACCOMBIE'S CASES. 219
vaccinated cet. sixteen, three re-vaccination marks; discrete attack;
discharged June 20."
3. "Caroline P., cet. twenty-three; admitted July ir,
1878. Five imperfect marks of primary vaccination ;
re-vaccinated cet. ten and sixteen. She stated that she
had a ' sore arm' on both occasions, but there were no
re - vaccination marks ; discrete attack ; discharged
August 22."
4. "Emma S., at. twenty-one ; admitted July 25,
1878. Two good marks of primary vaccination; four
marks of re-vaccination performed at the age of nine
or ten ; discrete attack ; discharged August 31."
5. "Lucy H., cet. forty-two; admitted August 5, 1878.
Two imperfect marks of primary vaccination; re-
vaccinated cet. twelve ; one re - vaccination mark ;
discrete attack ; discharged August 22."
6. "Sarah H., cet. thirty-six; admitted August 13,
1878. Three imperfect marks of primary vaccination ;
three marks of re - vaccination performed at the age
of sixteen ; attack confluent ; discharged July 23,
1879."
7. "Fanny C, cet. thirty-three; admitted March 11,
1879. One imperfect mark of primary vaccination;
i'c -vaccinated at. twenty-one, on left arm in two places.
There were no re-vaccination marks, but patient stated
that her arm was sore, and that the medical man to
whom she showed it a week after the operation was
performed said 'it was doing all right.' She died of
Miick small-pox on March 14."
8. "Sarah P., <Bt. twenty-one; admitted April 18, 1879.
'>.iid to have been vaccinated in infancy, but there
h-itc no marks. Has three marks of re - vaccination
performed at the age of eighteen ; discrete attack ; discharged May
5."
9. "Fanny L., at. thirty-six; admitted October 13,
t 879. Three imperfect marks of primary vaccination ;
two marks of re-vaccination performed at the age ot
thirty-one; discrete attack; discharged November 8,
1879."
10. "James H., at. twenty-seven ; admitted Novem
ber 8, 1879. One good mark of primary vaccination ;
re-vaccinated <zt. fifteen. Stated that he had a ' sore
arm' after re-vaccination. No marks ; discrete attack ;
discharged December 12."
Elsewhere Dr. John MacCombie says—" For myself, I am inclined to believe that
small-pox after successful re-vaccination is not infrequent."1 Apparently an
extended experience has not modified his views, for quite recently he says —
"Some persons who have been successfully re-vaccinated do, however, contract
small-pox. Of such cases observed by me the time intervening between the
re-vaccination and the attack of small-pox varied from one to twenty-five years
; the average being ten years."2 And further on in the same work he makes
further admissions when he says " it is impossible in all cases to promise
immunity from attack or even from death after vaccination and re-vaccination."3
In the Homerton Hospital Report for 1881 (p. n), Dr. Collie gives details of
three cases after re-vaccination.
1 Transactions of the Epidemiological Society, vol. iv., part ii., p. 193.
Sessions 1877-78 and 1878-79.
-Allbutt's "System of Medicine," vol. ii., p. 207. London. 1897. 3 Ibid.,
p. 222.
DR. COLLIE'S CASES. 221
1. "Henry P., cst. nineteen, admitted November n.
Primary vaccination in infancy; re-vaccination six
years ago ; three marks on right arm, two on left, but
patient cannot differentiate them ; all imperfect. Trans
ferred to ' Atlas' December 7. Mild discrete attack.
(Admitted from City and sent in City ambulance.) "
2. " Emma P. (sister of above), <zt. twenty-two,
admitted November 26. Primary vaccination in in
fancy ; five, imperfect marks ; re-vaccination six years
ago; no marks, but said to have taken well; again
re - vaccinated on morning of November 5 (first
symptoms of small-pox on November 21), seems to
have taken well. Transferred to ' Atlas' December 7.
Mild discrete attack. (Admitted from City and sent in
City ambulance.)"
3. "Ada J., at. twelve, admitted December 12.
Primary vaccination in infancy; two imperfect and
doubtful marks; re-vaccination six months ago; patient
says it took well; one imperfect and doubtful mark.
Mild discrete attack. (Sent by Hampstead in Hamp-
stead ambulance.)"
These cases, together with those recorded by Dr. Gayton and Dr. MacCombie, have,
through the courtesy of the Clerk, Mr. Duncombe Mann, been copied verbatim from
the reports of the Metropolitan Asylums Board. I wish to commend them to those
who affirm that compulsory re - vaccination would effectually extinguish
small-pox.
The following cases of small - pox, within short periods of re-vaccination, are
given in the Sheffield Report.
!
/1 Vaccinated ; Three well-marked cicatrices, ; Alleged to have suffered
:
: ! in infancy- j
three-quarters square inch j fromsmall-poxin Dec-
139 Ecclesall - -65 iElizabeth A. H. 29 !
; in area. , ember, 1887; eruption
P^e-vaccinated j One cicatrix,one-sixth square I only on the right hand ;
1 i l'October,i887.j inch in
area. no spots anywhere else
(
: Vaccinated j Three good-class cicatrices, i Small-pox in February, in
infancy. I area over one square inch. 1888, very mild attack, j
Re-vaccinated! Two well-marked cicatrices, tenspots.didnotfeelill. Sept.,
1887. I one-third square inch in
j
; ;
area.
. j
I ; ! I Vaccinated Three
well-maiked large ci- j Mild attack of small-pox
j i 11 in infancy. catrices,
one and one-half! in November, 1887;
72 Noith Sheffield - j 45 William F. - 27 -i
j square inches in area. ■ not pitted.
j Re-vaccinated Two small cicatrices. I in 1886
(' Vaccinated j Threewell-marked cicatrices, j Extremely mild attack of |
' in infancy. three-quarters square inch : small-pox in October,
71 North Sheffield - 5 Sarah G. - 12 -
\ in area. 1887 ; not
pitted, ill
\ Re-vaccinated One cicatrix
one-sixth square fourteen days.
'- I ,
in 1884. inch in area
I I
I I / Vaccinated Four fairly
well-marked cica- , Verymildattackof small-
j I I in infancy. trices,
one-thirdsquareinch pox in 1888, about
I 101 South Sheffield - 8 ! Fanny C. - 7
-j! in area. twentyspots.no
pitting.
I i
! i Re-vaccinated One small cicatrix.
!
I I in 1885.
!
i I Vaccinated
Threewell-markeddeepcica- ; Severeattackofsmall-pox!
|i in infancy. trices,three-quarterssquare in December,
1887,
IOi South Sheffield ■ 3 I Joseph W. - 29
-: inch in area. j badly pitted.
j !Re-vaccinated Two well-marked cicatrices.
I li in 1882.
DR. DALTON'S CASES. , 22 3
In the Report of the Metropolitan Asylums Board for i8yo (pp. 55-57), we learn
that, during the year, twenty-six patients were admitted for small-pox, and two
of these died. The first, aged twenty-six, had been unsuccessfully vaccinated
at nine months of age, and successfully vaccinated when about ten years of age,
and the scars were obscured by the eruption. The other death was in a man aged
forty-four, who had been three times successfully vaccinated, once in infancy,
and again at seven and twenty-one years of age. Five of the twenty - six
patients were unvac-cinated, and none of these died.
Dr. Dalton,1 in his critical examination of 1,000 cases of small-pox, gives a
list of sixty-one persons taking the disease from one to forty years after
re-vaccination. Of these, seven, or 11*5 per cent, died, or a higher fatality
than that for his 1,000 cases (8-5 per cent.).
If any further evidence were required to demonstrate the futility of
re-vaccination, it is furnished by the Army and Navy Reports. Staff-Surgeon T.
J. Preston informed the Royal Commission (Q. 3,270) that in 1883 " three cases
occurred in the ' Audacious,1 which were contracted at Shanghai. All three men
had been successfully re-vaccirtated—one in 1880, one in 1881, and the third in
1882. The disease was of a very mild form, and the men were but slightly
marked."
On p. 63 of the " Statistical Report of the Health of the Navy for the year
1881," dated 1882, there is a reference to nine cases occurring on the "
Eclipse," on
1 " Small-pox in its Relation to Vaccination," p. 25. J. II. C. Dalton, M.A.,
M.D.,B.C. (Reprinted from the Medical Chronicle, October, 1893.)
the East Indies Station. "The first case, in the person of a leading seaman,
aged thirty-one, was contracted at Rangoon where small-pox had been lately
prevalent, and proved to be a severe case of the confluent form of the disease.
The patient had been re-vaccinated two years before. He was taken ill on the
19th April; there was a copious confluent eruption, with high fever and
delirium. On the arrival of the ship at Trincomalee, he was landed at a bungalow
on Sober Island, where he died on the next day, 28th April. On the 29th April, a
second case appeared, in the person of an able seaman, aged twenty - seven, who
was at once landed in the temporary hospital; in his case the eruption was also
confluent, and he died on the eleventh day of the disease. He is said to have
been successfully re-vaccinated four years previously." There were seven other
cases, several of which were severe, and all of them vaccinated and
re-vaccinated.1
With regard to the army, the tract2 before alluded to informs us that the men
are always re-vaccinated on entering the force, and it states (p. 7) that "
official experience in England and abroad has shown that soldiers who have been
re-vaccinated can live in cities intensely affected by small-pox without
themselves suffering to any appreciable degree from the disease."
Brigade-Surgeon Nash, when examined before the Royal Commission, also agreed
(Q. 3,559) that in the
1 Second Report, Royal Commission on Vaccination. Q. 3,284.
2 Facts concerning Vaccination for Heads of Families. (Revised by the
Local Government Board, and issued with their sanction.)
RE-VACCINATION IN THE ARMY. 225
iirmy vaccination and re-vaccination was as perfect as endeavours could make it,
and yet he handed in a list of 3,953 small-pox cases, with 391 deaths, for the
years 1860-88. In 1889, among the troops in Egypt, there were 42 cases of
small-pox, with 6 deaths. These, on the strength (3,431), give an attack-rate of
12,241, :md a death-rate of 1,749 per million ; the attack-rate lieing six times
that of Leicester, and five times lh.it of Keighley, and the death-rate fifteen
times I hat of Leicester and eight times that of Keighley in I he recent
epidemics in these notoriously unvaccinated towns.
The Army Medical Report for 1889 states (p. 190J:— "A detachment of the 1st
Battalion Welsh Regiment was stationed at Assouan during the latter part of 1888
and the early part of 1889 ; during that time an outbreak of small-pox occurred
among the native population, and the disease broke out among the troops ; two
cases also occurred on the voyage from Assouan to Cairo. Notwithstanding all
the precautions taken in Cairo, and due regard having been paid to vaccination
and re-vaccination, the disease kept on the increase, and in the month of May
presented signs of doing so still further. The Welsh regiment, which suffered
most, was in Kasr-el-Nil barracks, which are situated near a crowded 1
horoughfare and on the banks of a navigable river. It being more than probable
that the disease was derived from natives, the Welsh regiment, on the
recommendation of the Principal Medical Officer, was removed to Abbassiyeh,
where the situation is healthier and intercourse with the natives could be
prevented. Small-pox, the Principal Medical Officer, Deputy-Surgeon General
Jameson, remarks, is always more or less prevalent among the natives in Cairo,
and, indeed throughout Egypt, and as there exists no means of segregating
affected cases, it is certain that patients in various stages of the disease are
permitted to walk about, and to frequent bazaars and streets to the great danger
of the public."
If we take the figures over a long period, the results are the same.1 Thus, in
Egypt, in the fourteen years, 1882-95, there were 233 cases and 25 deaths from
small-pox among the troops, or an average annual attack-rate of 3,004, and a
death-rate of 322 per million. The Indian army, during the same period,
furnished 691 cases and 68 deaths, the rates being j6& and 76 per million
respectively ; while in Leicester the rates were only 204 and 13 per million
(446 cases and 29 deaths). I may mention that the comparison is unfair to
Leicester, for the army consists of picked men living at a comparatively
insusceptible period of life.
The following cases extracted from a report by Surgeon I. Boulger,2 of the Army
Medical Staff, relate to the small-pox which prevailed among the troops at Cairo
in 1885 :—
" Private A. W—, 2nd East Surrey Regiment, age twenty-three; service, three
years. Marks, three right (good). Re-vaccinated on enlistment; modified.
Admitted, 4th December, 1884 ; discharged, 8th January, 1885—thirty-six
days. This was a mild case;
1 See Appendix.
-' '' Report of a series of cases of small-pox which occurred amongst the
British troops in Cairo from January to October, 1885." Appendix to the Army
Medical Report for 1885, pp. 443-450.
RK-VACCINATED SMALL-POX IN CAIRO. 227
symptoms preceding eruption were well marked, such ;is lumbar pain, vomiting,
pyrexia ; but the eruption was scanty; discrete throughout ; slight secondary
lever ; no pitting."
" I'rivate F. A—, 2nd East Surrey, age twenty-three ; service, three and a
quarter years. Marks, one right (good), three left (fair). Re-vaccinated on
enlistment; modified. Admitted, 2nd February, 1885 ; discharged, 15th May,
1885—one hundred and three days. Patient had been under treatment in hospital
for a month with secondary syphilis, when symptoms of small-pox appeared. The
attack was most severe, of the confluent type. Convalescence was delayed by
large boils on legs, and for a long time he was in a very anaemic state. Skin
much pitted."
" Private J. K—, 2nd East Surrey, age twenty-eight ; service, five and a half
years. Marks, two right (good), one left (faint). Re-vaccinated on enlistment;
modified. Admitted, 2nd February, 18^5 ; discharged, 22nd March,
1885—forty-nine days. Was of the confluent variety. Temperature before eruption
appeared, 1030 l'"ahr. Patient very robust ; there was a large quantity of
eruption, and it went on to maturation, though without much secondary fever. No
complications ; throat was sore."
"Sapper J. H—, Royal Engineers, age twenty-five; service, three years. Marks,
two right (good). Re-vaccinated on enlistment ; modified. Admitted, 2nd
February, 1885 ; discharged, 22nd February, 1885— twenty - one days. Very mild ;
discrete ; eruption scanty, but went on to maturation ; no complications ; no
pitting ; desquamation rapidly completed."
" First-class Staff-Sergeant E. F—, Medical Staff Corps, age thirty-two;
service, fourteen years. Marks, two left (good) ; two right (fair).
Re-vaccinated, 18th August, 1870; failed. Re-vaccinated, 2nd March, 1876;
perfect. Admitted, 2nd February, 1885; discharged, 21st February, 1885—nineteen
days. Very mild case ; very little eruption, and it never went beyond the
vesicular stage ; had most severe initial symptoms. The lumbar pain was intense,
and twenty-four hours before eruption appeared, he had a well-marked attack of
dry pleurisy on the left side ; the friction sound was very marked, and the
temperature, 103° Fahr."
" Private F—, 2nd Royal Sussex, age twenty-two ; service, three years. Marks,
two right and two left (faint). Re-vaccinated, 2nd February, 1882; perfect.
Admitted, 22nd February, 1885 ; discharged, 13th March, 1885—eighty-two days.
Very severe; initial symptoms, vomiting, lumbar pain, pyrexia very marked;
eruption preceded by a scarlatinous prodromal rash over pubes, and at flexures
of joints. Eruption copious, confluent on face and forehead ; went on to
suppuration, but there was not much secondary fever. Large, soft crusts formed
on face when the pustules ruptured, and convalescence was long delayed owing to
the adherence of these crusts."
" Private P—, 2nd Royal Sussex, age twenty-one ; service, two years. Marks, two
left (fair). Re-vaccinated 24th May, 1883; modified. Admitted 21st March, 1885 ;
discharged, 4th May, 1885—forty-five days. Severe case. Eruption confluent, with
marked nervous symptoms ; eruption went on to pustulation ;
RE-VACCINATED SMALL-POX IN CAIRO. 229
secondary fever high ; extensive crusts formed on face ; dcsquamation was long
delayed ; slight pitting."
" Private C—, 2nd Royal Sussex, age twenty-three; service, four and a third
years. Marks, two left (good). Re-vaccinated, 2nd December, 1881 ; modified.
Admitted 24th March, 1885 ; discharged, 2nd May, 1885— forty days. Case of
average severity ; semi-confluent. Kruption plentiful, and went on to
pustulation. No complications ; desquamation slow."
" Lance - Corporal S—, 2nd Royal Sussex, age twenty - three ; service, three and
a quarter years. Marks, two right (good), four left (fair). Re-vaccinated, 1881
; modified. Admitted, 25th March, 1885 ; discharged, 21st April,
1885—twenty-eight days. Very mild case ; eruption scanty ; no secondary fever of
any consequence; pustules formed and soon dried up ; desquamation rapid."
"Private M—, 1st Yorkshire Regiment, age twenty; service, two years. Marks,
three right (good). Re-vaccinated on enlistment; modified. Admitted, 16th April,
1885 ; discharged, 16th May, 1885—thirty-one days. Case of average severity.
Eruption copious, but discrete ; went on to suppuration. No complications,
except severe sore throat."
" Private O—, 2nd Royal Sussex, age twenty; service, two years. Marks, three
left (good). Re-vaccinated, 25th August, 1883 ; modified. Admitted, 29th April,
1885 ; discharged, 5th June, 1885—thirty-eight days. Case of average severity;
initial symptoms severe. lCruption copious, but discrete ; went on to
pustulation ; not much secondary fever. No complications or pitting ;
desquamation tedious."
"Private A—, 2nd Royal Sussex, age twenty; service, two years. Marks, three
right (good). Re-vaccinated, 25th May, 1883; perfect. Admitted, nth May, 1885;
discharged, 22nd June, 1885—forty-three days. Case of average severity. Eruption
copious, but discrete ; went on to formation of pustules ; very little secondary
fever. No complications ; desquamation much prolonged."
" Private MacF—, 1st Gordon Highlanders, age twenty-six ; service, five and two
thirds years. Marks, three left (very faint). Re-vaccinated, 10th October, 1879
; modified. Admitted, 20th May, 1885 ; died 28th May, 1885—nine days." (Man
contracted smallpox while under treatment for syphilis at the hospital.)
"Private J—, 2nd Duke of Cornwall's Light Infantry, age twenty-four ; service,
four years. Marks, two left (good). Re-vaccinated on enlistment ; modified.
Admitted, 24th June, 1885 ; discharged, 21st July, 1885— twenty-five days. Very
mild case ; but the eruption went on to pustulation. Eruption scanty and
discrete everywhere; no secondary fever ; desquamation rapid."
" Private S—, 1st Royal West Kent, age twenty-two ; service, three years. Marks,
three left (good). Re-vaccinated, 1882 ; modified. Admitted, 27th June, 1885;
discharged, 12th August, 1885—forty - seven days." (Muscular pains, followed by
vomiting and rise of temperature. Copious discrete eruption all over body,
rapidly going on to pustulation ; desquamation tedious.)
"Private F—, 2nd Oxford Light Infantry, age twenty; service, two years. Marks,
two left (good). Re-vaccinated, July, 1883 ; perfect. Admitted 15th July, 1885
; discharged, 12th August, 1885—twenty nine
RE-VACCINATED SMALL-POX IN BERLIN. 231
days. Mild case ; usual initial symptoms, and which were well marked. Eruption
appeared on 17th; was scanty, and principally on forehead and face; discrete
everywhere. Papular became vesicular on 19th, and then proceeded no further, but
rapidly dessicated. No secondary fever. Case was complicated with slight sore
throat ; desquamation rapid."
" Lance-Corporal G—, Mounted Police, age twenty-six; service, six years. Marks,
four left (faint). Re-vaccinated, 25th September, 1879; modified. Admitted, 30th
July, 1885 ; died, 3rd August, 1885—five days." (Surgeon Boulger here gives
details of the case, which appeared to be of the haemorrhagic variety.)
In the 1870-72 epidemic at Berlin1 we have figures on a still larger scale.
There were 1,036 re-vaccinated cases of small-pox, and of these 162 are reported
to have died. This is a fatality of 156 per cent., or very little less than the
average fatality of small-pox during the last century in England, and over two
and a half times that of unvaccinated Leicester in the recent i epidemic.
■ A statement which is always quoted as indisputable I evidence of
the special protective power of re-vaccination, is the alleged immunity
of small-pox hospital attendants.
If re-vaccinated nurses do not take small-pox, as affirmed, abundant evidence
has been adduced to show that this is not the case with re-vaccinated soldiers ;
and hence it is clear that the nurses' immunity
1 " Zeitschrift des Koniglich Preussischen Statistischen Bureaux," p. 119.
ItiTlin. 1873.
(such as it is) is rather a function of being nurses than of being re -
vaccinated. Moreover, unre-vaccinated attendants have had a like immunity, as
shown by the experience of M. Colin at the Bicetre Hospital— an immunity, it may
be noted, which was not shared to so marked a degree by the re-vaccinated. He
found that out of nearly two hundred attendants on the hospital staff, almost
all of whom had been re-vaccinated under his own eyes, fifteen were attacked
with smallpox, with one death ; while among the forty doctors and chemists
attached to the establishment, and among the forty nuns who took care of the
patients night and day, and who lived in the centre of the hospital, none were
attacked, in spite of the fact that the greater number of the staff, and a large
number of the nuns neglected to get themselves re-vaccinated.1
Examples of immunity, even when strongly exposed to small-pox, have also been
observed in the un-vaccinated ; these have been alluded to in an earlier
chapter. The following personal experience, detailed in a letter, dated March
10, 1897, from one of the Managers of the Metropolitan Asylums Board, is a case
in point:—
" In answer to yours of the 2nd inst. I was elected as Manager to the
Metropolitan Asylums Board in March, 1892, and placed on the Small-pox Hospital
Ships Committee at once. This Committee meets at the Ships every fortnight,
except during holidays ; a surprise committee visits the Ships in the intervals
between the Committee meetings. I generally visit
1 La Variole, pp. 84, 114. Leon Colin. Paris. 1873.
IMMUNITY OF PLAGUE ATTENDANTS. 233
the wards, speak to the patients, examine the bed-cards to ascertain the
vaccinal state of the patients. The number of patients, according to the Annual
Reports, admitted to the ships from 1892 to 1896 inclusive is 4,952 ; and I have
no doubt that I have seen from 3,000 to 4,000 patients suffering from smallpox,
and some of these cases twice or thrice. My case is stronger than you put it. I
have not even been vaccinated, or had small-pox to my knowledge; the reason I
was not vaccinated, I understand, being I hat I was too delicate in my young-
days to be subjected to the operation."
Apparently small-pox is not the only zymotic disease in which an immunity of
hospital attendants has been observed, for Dr. James Cantlie, in his interesting
report on the recent outbreak of bubonic plague in I long Kong, specially
alludes to the fact that " no nurse, male or female, concerned in attendance at
the hospitals devoted to plague, contracted the disease." *
It is not quite manifest why persons frequently exposed to contagion should be
immune. M. Colin, a strong advocate of vaccination, felt called upon to :;ive
some explanation of the cases coming under his notice, and he suggested that a
certain tolerance was acquired by repeated exposures. Of course, this may nr may
not be true ; but whether the theory be .accepted or not, it is clear that some
other explanation of the alleged immunity of the hospital attendants, than the
one usually given, must be sought for t o meet all the facts of the case.
1 British Medical Journal, August 25, 1894, vol. ii., p. 425
Reference is often made to the German army. Sir Joseph (now Lord) Lister, at
the annual meeting of the British Association in 1896, is reported to have said
that small-pox " is absolutely unknown in the huge German army, in consequence
of the rule that every soldier is re-vaccinated on entering the service."1
In a letter to the Times of September 23, 1896, Mr. Trobridge pointed out that
the ordinance enforcing re-vaccination on all recruits, came into force on June
16, 1834, and that it provided for at least ten insertions being made in each
arm ; and he quoted the evidence of Dr. Arthur F. Hopkirk, who informed the
Royal Commission that he believed the law was always obeyed ; and those men who
refused were tied down and vaccinated by force (Q. 6,799).
The following are the figures for small-pox in the German army since 18252:—
Small-pox. I
Small-pox.
Year. Cases. Deaths.
Year. Cases. Deaths.
1825 ... ? 12 1836 ...
130 9
1826 ... ? 16 1837 ...
94 3
1827 ... ? 23 1838 ... in 7
1828 ... ? 35 1839
••• 89 2
1829 ... ? 33 1840
... 74 2
1830 ... ? 27 1841
... 59 3
1831 ... ? 108 1842
... 99 2
1832 ... ? 96 1843
... 167 3
1833 ... ? to8 1844
... 69 3
1834 ... 619 38 1845 ...
30 1
1835 ... 259 5 1846
... 30 1
1 The Times, September 17, 1896.
2 " Beitrage zur Beurtheilung der Nutzens der Schutzpockenimpfung,
pp. 23, 24. Berlin. 1888.
SMALL-POX IN THE GERMAN ARMY. 235
Small-pox.
Small-pox.
Year. Cases. Deaths.
Year. Cases. Deaths.
1847 ... 5 o 1868 ... 97 1
1848 ... 22 1 1 1869 ... 108 1
1849 ... 62 I : I87O1
... 41 O
1850 ... 176 1 ! 187071s ... 2,879 J&4 '
1851 ... 246 3 18713 ... 828 34
1852 ... 87 1 1872 ... 389 12
[853 ... 138 1 18734 ... 26 2
1854 ... 121 3 1873-746 ... 22 1
T855 ... 12 o 1874-75 ••• 2^ o
1856 ... 21 o 1875-76 ... 20 o
1857 ... 35 1 1876-77 ... 19 o
1858 ... 64 o 1877-78 ... 12 o
1859 ... 58 2 1878-79 ... 15 o
1860 ... 44 3 1879-80 ... 7 o
1861 ... 56 4 1880-81 ... 23 o
1862 ... 25 1 1881-82 ... 16 o
1863 ... 90 o 1882-83 ••• 9 °
1864 ... 120 1 1883-84 ... 7 o
1865 ... 69 1 1S84-85 ... 7 I6
1866 ... 91 8 1885-86 ... 6 o
1867 ... 188 2 J886-87 ••• 7 o
It will thus be seen that since the year 1834, there have been 7,505 cases and
291 deaths from small-pox in the German army, and hence Lord Lister's statement
is obviously inaccurate. On March 31, 1897, at a meeting presided over by
the Duke of Westminster for the
1 From January to June, 1870.
2 From July, 1870, to June, 1871.
3 From July to December, 1871.
4 From January to March, 1873.
5 From April 1, 1873, to March 31, 1874.
" The above death was in .1 man who was twice unsuccessfully re-vaccinated when
recruited.
purpose of raising a fund for a national memorial to Edward Jenner, Lord Lister
took occasion to modify his original statement. He excused his previous
utterance by saying that he had " quoted from memory after reading an authority
on the subject," and added that " if he had stated that ' fatal' small-pox was
absolutely unknown in the German army he should have been speaking the literal
truth."1 With an exception in 1884-85, it is quite true that there have been no
deaths from small-pox in the German army since 1874-75; but Lord Lister must be
aware that " in consequence" is usually held to imply an effect following on a
cause, and that it is scarcely clear, without further explanation, why we should
wait for half a century for the alleged effect of something which commenced to
operate as an alleged cause in 1834. In other words, Lord Lister in order to
make good his case, even as amended, should account for the small - pox deaths
in the German army since 1834, and more particularly the 210 deaths in 1870-72,
for whatever the vaccinal condition for some years subsequent to the enactment
in 1834, aU authorities agree that the German army was a thoroughly well re -
vaccinated body in 1870-72. The decline of small-pox and other zymotic diseases
in recent years in the German army is due no doubt, as Mr. Trobridge has
suggested, to the " great wave of sanitary reform which spread throughout the
newly-formed German Empire in 1872, and which has reduced the general death-rate
from 29 per 1,000 living in that year to 24 per 1,000 in 1887."
1 The Times, April 1, 1897.
SMALL-POX IN THE FRANCO-PRUSSIAN WAR. 237
Another statement which is frequently appealed to is, that during the
Franco-Prussian war, 23,469 died from small-pox in the French army, whereas the
German .mny only lost 263 from this disease, the difference being attributed to
want of re - vaccination in the h'rench army. In 1883 Dr. W. B. Carpenter refers
to the subject thus—"In Germany, vaccination is compulsory in children under a
year old ; and every man on his entrance into the army is re-vaccinated. In
France, on the other hand, vaccination is not compulsory, and re - vaccination
is not enforced on ■ irmy - recruits. During the Franco - German war of 1870-71
the total number of deaths from small-pox in the German army was 263, while in
the French army it was 23,469, or very nearly ninety times as great."1
On June 19, 1883, Sir Lyon, now Lord Playfair, triumphantly reproduced the
statistic with great effect in the House of Commons, in a speech which is
reputed to have influenced more votes than any speech ever made in Parliament.
Mr. Ernest Hart gives us the authority for the statement. " Total deaths from
small-pox in German army (where re-vaccination was rigorously enforced), 263 ;
in the French army (where re - vaccination was neglected), 23,469. Cf. Colin
: La Variole."2
, Now, there does not appear to be any authority for saying that re-vaccination
was not enforced in the French army, and exception must also be taken
to
1 A Letter to the Right Hon. Lyon Playfair, C.B., M.P., F.R.S., p. 8. William B.
Carpenter, C.B., M.D., F.R.S. London. 1883.
■ liritish Medical Journal, June 23, 1883, vol. i., p. 1217, foot-note.
the 23,469 French soldiers reported to have died of small-pox. Mr. Alexander
Wheeler followed up this statement as soon as it was uttered, and he received
assurances from the French War Office that there were no official medical
statistics taken out during the period of the war in 1870-71.
According to the " Wiener Medizinische Wochen-schrift,"1 this figure (23,469)
would appear to have been taken from a French source of information ; and Dr.
Hopkirk informed the Royal Commission that it had been recently confirmed from
Paris (Q. 1,543), that he believed the confirmation was official (Q. 1,654),
and, moreover, an "absolute fact" (Q. 6,774); but when he was confronted with
the French official records, in which it was stated that the medical statistics2
in 1871-72 were wanting (Q. 6,778-6,782), he was obliged to admit that he was
not aware of any figures on which the calculation was based (Q. 6,787).
It appears that the statistic rests on certain figures given by M. Colin for the
garrison at Paris. He estimated that there were about 1,600 small-pox deaths on
an effective strength of 170,000 men, indicating a small-pox mortality of '94
per cent.3 The number 23,469, it is said, was obtained by applying this ratio to
the whole army of France.4
When Dr. Carpenter found that the statement he had made was incorrect, he
most honourably retracted it
1 "Wiener Medizinische Wochenschrift," August 31, 1S72, p. 896.
2 See also " Rapport sur la Vaccine," p. 47. Proust. 1889.
3 " La Variole," p. 58. Leon Colin. Paris. 1873.
4Letter from Dr. Jeunhomme to Dr. Collins. Sixth Report, Royal Commission on
Vaccination, Appendix, p. 727, foot-note.
SMALL-POX IN THE FRANCO-PRUSSIAN WAR. 239
in the Daily News of August 7, 1883. He says, "I requested Earl Granville to
obtain what information he could on this point; and, after considerable delay, I
have received through Colonel Cameron (military attach^ to t he Embassy in
Paris) an explicit statement that the army medical returns of the Franco-German
war are so incomplete as not to supply the total for which I asked."
Mr. Ernest Hart,1 whom I have also mentioned as giving currency to the
statement, has reproduced the discredited statistic quite recently (1897). He
refers to " the following utterances of M. de Freycinet when Minister of War in
1890," and then quotes him as follows :—" One now sees, not only in France, but
in Algeria, in Tunis, and in Tonquin, the army protected by the strict
application of compulsory vaccination. . . . I cannot forget that, in 1870-71,
the German army, counting a million vaccinated and re-vaccinated men, only lost
459 men from small-pox in the two years, whereas our army, far less numerous,
had, from the same cause, a loss of 23,400 men whom the prescient application of
re - vaccination might have saved for the service of France." This "quotation
from a report by M. de Freycinet, dated June 16, 1882, is apparently taken from
the sixth volume of the Royal Commission evidence (Appendix, p. 727), which was
published subsequently to Mr. Hart's article, and Mr. Hart has omitted to notice
an asterisk at the end of the quotation ; this refers the reader to a footnote
containing a letter from Dr. Jeunhomme to Dr.
'Allbutt's "System of Medicine," vol. ii., p. 662. London. 1897.
Collins, in which Dr. Jeunhomme states that no official documents exist, and he
proceeds to explain how the statistics for the whole army have been arrived at
by calculation from the estimate given by M. Colin of the small-pox mortality of
the army in Paris.
Even if the 23,469 statistic were true, it would be absurd to compare the
small-pox mortality of the strong, resolute Germans, conscious of victory, with
that of the cowed, worn, starved, and discomfited French. As it happens, the
figure is a pure assumption; but no statement has probably ever been quoted with
more telling effect, or done such service to the cause of compulsory
vaccination.
CHAPTER VIII.
INFLUENCE OF SANITARY MEASURES ON THE INCIDENCE AND
MORTALITY OF SMALL-POX.
The influence of sanitation as regulating the attack and death-incidence of
small-pox has already been alluded to in various parts of this work, more
particularly in the third chapter, dealing with the causes of the decline of
the disease. Since that chapter was written, a resolution has been adopted by
the Jenner Society, signed by a large number of medical officers of health,
denying the sufficiency of sanitation as a preventive of small-pox-, and
affirming that " the only trustworthy protection at present known against
smallpox, alike for the individual and the community, is efficient vaccination
in infancy and subsequent re-vaccination, and that the only effective way of
stamping out epidemics of this disease lies in the free use of these agencies."
It is necessary, therefore, to deal with this important branch of the subject
more fully.
The views of the Royal Commission may be gathered by the following quotations
extracted from their Final Report.
"The question how far the behaviour of small-pox in the eighteenth century and
earlier was influenced by sanitary con-ilitions, is one rendered difficult by
the lack of exact information. We may distinguish between overcrowding as
one insanitary
condition and all other insanitary conditions, such as lack of cleanliness and
the like. A priori we should expect that a dense population, especially one of
great internal movement, and one in continual interchange with surrounding
populations, by offering greater facilities for the conveyance of contagion,
would lead to a greater amount of small-pox." (Section 78.)
"We might a priori expect the other acknowledged imperfect sanitary conditions
of the eighteenth century to increase the fatality of, and so to a corresponding
extent, the mortality from small-pox ; but there is no exact evidence to confirm
this supposition." (Section 78.)
" In general both the incidence of, and mortality from, smallpox seem to have
been far less affected by sanitary conditions than might a priori have been
expected." (Section 78.)
" Admitting a priori that crowded dwellings tend to increase the liability to
contagion, and so the prevalence of the disease, while other insanitary
conditions tend in addition to increase the fatality among those attacked, so
that insanitary conditions as a whole must tend to increase the mortality from
small-pox; no evidence is forthcoming which distinctly shows that the
dependence of the prevalence of, or the mortality from, small-pox, on the lack
of sanitary conditions, was a feature of the history of smallpox during the
eighteenth century." (Section 79.)
"Whatever may have been the sanitary improvements during the first quarter of
this century in England and some other countries, there seems no ground for
supposing that throughout Western Europe the period was marked by great changes
in the direction of improved sanitation. Indeed, in many countries down to a
recent period, in some it may perhaps be said even to the present time,
insanitary conditions have continued to prevail." (Section 81.)
" There is no proof that sanitary improvements were the main cause of the
decline of small-pox under discussion. And no adequate evidence is forthcoming
to show to what extent such improvements may be considered as a subsidiary
cause." (Section 82.)
"We have already pointed out that small-pox tends at times to become epidemic,
z'.e., to spread more readily than at other times.
VIEWS OP' THE ROYAL COMMISSION. 243,
The occurrence of the conditions, whatever they may be, which cause the disease
to be thus epidemic has of course no relation to the state of the population as
regards vaccination, even conceding to the full that it has a protective
effect. The only result of widespread vaccination, in a case where small - pox
became epidemic, could be to render the extent of the epidemic more limited, and
its fatality less than it would otherwise be." (Section 144)
" It is beyond doubt that an infectious disease like small-pox is, other things
being equal, more likely to spread in towns than in country districts, and more
likely to spread in crowded town districts than in others not so densely
populated ; so that we should expect a lessened proportion of overcrowded
dwellings, by diminishing the opportunities for contagion, to check the
prevalence of the disease and consequently to render its mortality less."
(Section 147.)
"We have already pointed out that on a priori grounds it is reasonable to think
that improved sanitary conditions would tend to diminish the fatality of, and so
to a corresponding extent the mortality from, small-pox. And there can be no
doubt that the period with which we are dealing has been characterised by an
improvement of this description. There has been better drainage, a supply of
purer water, and in other respects more wholesome conditions have prevailed."
(Section 151.)
"We do not mean to indicate an opinion that sanitary improvements have been
without an effect on small-pox mortality, but only that when all the changes
which have occurred are considered, it cannot be asserted that they afford an
adequate explanation of the diminished mortality from small-pox." (Section
153.)
"We fully recognise that sanitary improvements have had an effect in reducing
the mortality from small-pox as from the other diseases to which we have just
been referring." (Section 166.)
If these various quotations and fluctuating opinions are summed up, they amount
to this. The Commission state (144) that the occurrence of the conditions which
cause small-pox to be epidemic has no relation
to the state of the population as regards vaccination. They also imply (481J)
and admit (4941) that some other reason than vaccination must be sought for to
explain the decline of small-pox. They allow that overcrowding, which is
distinctly an insanitary condition, accentuates the disease (78, 79, 147). They
also admit that other insanitary conditions have some influence (78, 79, 151,
153, 166). They say that sanitary improvements act especially in the direction
of diminishing fatality (79, 151), although there is no proof that they are the
main cause (82), and that they cannot be asserted to form an adequate
explanation of the diminished mortality from small-pox (153).
I am not at all sure that those who favour the view that sanitary measures are
responsible for the diminution of small-pox will be disposed to quarrel with
these conclusions ; my own reading of the Report is that the Commissioners, in
their desire to state the case fairly, have been obliged, somewhat reluctantly,
to admit sufficient to seriously discredit the point of view for which they are
arguing". I do not know that it has ever been seriously maintained that the
amelioration of insanitary conditions is the only cause of the decline of
small-pox, as others have been suggested, to which I have alluded in my third
chapter, but that insanitary conditions are among the principal causes of the
prevalence and mortality of this complaint must, I think,
1 In Section 481 the Commissioners refer to the experience of Leicester; and in
Section 494 to the recent decline of small-pox in the Metropolis, and they
add—"We think it is impossible to attribute this change to vaccination."
OPINION OF LORD SHAFTESBURY. 245
be allowed. The purport of the present chapter is to supply further evidence
under this heading.
A prominent feature of small-pox is that it has been confined almost exclusively
to the lower stratas of society, or among those who live in the least favourable
sanitary conditions. In Austria, small-pox is called the " beggars' disease,"
and in this country it is largely spread by tramps, who not only live under
unhealthy circumstances, but are frequently deprived of the common necessaries
of life.
Mr. John Cross found that at Norwich, in 1819, the small-pox epidemic was
"confined, almost exclusively, to the very lowest orders of the people." x
In the Provincial Medical and Surgical Journal for December 22, 1852, in an
article entitled, "Report on Small-pox, as it occurred during three Epidemics in
the practice of the Canterbury Dispensary between the years 1837 and 1848," Mr.
Rigden says, concerning the third epidemic (p. 682), that "The most severe
cases, and the greatest number, existed, generally speaking, in the districts
most thickly populated by the lower orders, and most badly drained."
In the debate on the Compulsory Vaccination Bill of 1853, Lord Shaftesbury
confessed that it was perfectly correct " that the small-pox was chiefly
confined to the lowest class of the population, and he believed that with
improved lodging-houses the disease might be all but exterminated."2
1 "A History of the Variolous Epidemic which occurred in Norwich in the year
1819," p. 7. John Cross, M.R.C.S. London. 1820.
-Hansard's Parliamentary Debates. Third series, vol. cxxv., p. 1012.
A r\r\\ TO tK n
The Medical Times and Gazette of February n, 1871 (vol. i., p. 159), in
referring to mistakes in diagnosis, indicates very plainly the class of people
and the miserable environment of those who took small-pox in the 1871-72
epidemic, and observes: — "Medical men cannot be too cautious in such a matter;
but when it is considered that the diagnosis has often to be made under most
unfavourable circumstances, in dark corners of ill-lighted rooms, amidst the
discomforts of squalid surroundings, chattering women, and squalling children,
often by candle - light, and upon individuals where the dirt upon the skin is
apt to obscure otherwise distinct signs, while the patients are too stupid to
reply clearly to questions, the drift of which they are at a loss to comprehend,
one cannot altogether wonder at occasional occurrence of error."
Likewise at Birkenhead, in 1877, Mr. Francis Vacher, the Medical Officer of
Health, noted that " an overwhelming majority of the sufferers in this epidemic
(consisting of 603 cases of small-pox) were derived from the labouring class,
and the remainder—six only excepted—from the artizan class."1 The six
exceptions alluded to were two professional men, two clerks, an insurance
agent, and a shipbroker.
Dr. Savill,2 in his report on the Warrington epidemic for the Royal Commission,
has pointed out that all but eleven of the 455 infected houses were rated at
less than Ł16 per annum, and 406 of them at ŁS or lower;
1 "Notes on the Small-pox Epidemic at Birkenhead in 1877," p. 16. -Final Report,
Royal Commission on Vaccination, Appendix v., p. 87.
RESULTS OF SANITARY IMPROVEMENT. 247
and Dr. Coupland -1 found that at Dewsbury the incidence of the disease with
but few exceptions fell upon members of the working class community.
On the other hand, it has been observed that in industrial dwellings, where the
poor are aggregated under strict sanitary supervision, there has been a marked
immunity from small-pox. Thus Dr. South-wood Smith observed that " There has
been in the improved dwellings complete exemption from typhus, cholera, and it
may be added small-pox; yet it must I be admitted, that other forms of zymotic
disease— scarlet fever, measles, whooping-cough, and diarrhoea— have occurred,
though rarely, and these maladies have in no instance spread."2 Dr. Collins and
Mr. Picton also report that they learn from the secretary of the Improved
Industrial Dwellings Company that in 1880-82 there were but 2 deaths from small
- pox among more than 15,000 tenants, while there were 3,268 small-pox deaths in
those years in London with a population of 3,8oo,ooo.3
In the Fifth Annual Report of the Registrar-General, dated 1843, will be found
replies from Metropolitan Registrars relative to the sanitary state of their
districts. A number of these testify to the occurrence of small-pox and other
zymotic diseases in the poorest and most filthy parts of their districts, from
which I have taken the following :—
1 Final Report, Royal Commission on Vaccination, Appendix iii., p. 28.
a " Results of Sanitary Improvement," p. 17. Southwood Smith, M.D. London.
1854.
3 Royal Commission on Vaccination, Dissentient Commissioners'Statement, section
231.
248 INFLUENCE OF SANITARY MEASURES.
The Registrar of the north-east district of Chelsea remarked that the
crowded buildings in his district are more fatal to the first four
classes of cases (smallpox, measles, scarlatina, and whooping-cough) than to
any of the others (p. 486).
The Registrar of the Hanover Square district of St. George, Hanover
Square, reports (pp. 487, 488) that the districts which suffered most from
contagious and epidemic diseases were Oxford Buildings, Brown Street, Hart
Street, Toms Court, George Street, Grosvenor Market, Grosvenor Mews, and
Thomas Street. " Toms Court," he says, " contains eight houses;
inhabitants in a wretched state in many cases, partly from want of employ,
partly intemperance. Small-pox and epidemics have raged here."
The Registrar of the Rectory division of Marylebone stated (p. 498) that the
greatest number of deaths from small-pox, measles, and scarlet fever occurred in
York Court and Calmell Buildings. He further stated that York Court, Calmell
Buildings, and Gray's Buildings appeared to be the unhealthiest portions of the
district. He added that the drainage of York Court was bad, that of Calmell
Buildings " good; or rather middling ;" the inhabitants complained of the
inefficiency of the water supply, and the districts were anything
but cleanly. According to the previous year's census, the inhabitants of one
house ranged from fifteen to seventy, the greatest number known to sleep in one
room being eleven. He remarked that Calmell Buildings, which was principally
inhabited by the Irish poor, was a narrow court about twenty-two feet in
breadth, and the houses, three storeys high, were surrounded and overtopped by
INSANITARY CONDITIONS. 2/\<)
tin* adjacent buildings ; the drainage was carried on by ;i common sewer running
down the centre of the court, and the lower apartments, especially the kitchens,
which were underground, were damp and badly ventilated, light and air being
admitted through a grating on a level with the court. At all times, but
especially in warm weather, most offensive effluvia were perceptible i-verywhere.
According to the previous year's census, there were 944 inhabitants, and the
number of persons in one house varied from two to seventy (p. 499).
The Registrar of the St. Mary division of Marylebone stated (p. 501) that " the
few cases of small-pox which occur in my district are invariably amongst the
poor," but that the other zymotic diseases named were not confined
disproportionally to any parts or class of inhabitants.
The Registrar of the Gray's Inn Lane division of St. Pancras remarked that small
- pox, measles, and whooping-cough had been most prevalent in certain districts,
which included Battle Bridge, comprising Britannia, George, Charlotte, Field,
and Paradise Streets, with many small courts and places leading therefrom. He
stated that in the Battle Bridge district1 the condition was extremely bad, the
streets being unpaved and impassable, occasioned by quantities of rubbish and
filth thrown thereon. The water supply was generally very good, but drainage
very bad in many places, and great want of cleanliness universally.
1 The district known as Battle Bridge formerly occupied the site on which King's
Cross Station now stands.
17
He forwarded the accompanying statement, which bears upon the subject under
consideration (p. 506). " I beg to state," he says, " that I adopted the plan of
searching all the register books from November, 1837, to the present time. I
made columns, headed by the names of the several diseases, and as they appeared
in the books, placed the names of the streets in which deaths occurred ; this
plan gave me at once the means of ascertaining amongst what particular classes
the several diseases most prevail. I found between 50 and 60 cases of small-pox,
the whole of which, with two exceptions only, are confined to the occupants of
the lowest habitations ; between 15 and 20 cases of typhus, occurring only
amongst the lower classes ; 60 or 70 cases of measles, in the proportion of
about two to one amongst the lower classes ; of whooping-cough between 80 and
90, occurring in about the same proportion as the measles; of scarlatina between
70 and 80, which appeared to prevail without regard to circumstance or place ;
very few cases of diarrhoea, dysentery, cholera, and influenza, and those not
confined to any particular part. The population of my district is 22,149."
In the St. Anne division of the Strand the Registrar observes (p. 523)—"Of
small-pox in 1838 there were thirty-one cases; in 1839, none; in 1840, two; in
1841, five; and in 1842, eight. Of those in 1838, three were in Falconberg
Court, three in St. Anne's Court, and four in Crown Street. These are poor
places, and densely peopled ; in Falconberg Court and Crown Street there are
some Irish. The remaining cases arc dispersed over the parish."
The report of the Registrar of the Goswell Street
SALUTARY EFFECT OF OPEN SPACES. 25 I
division of Clerkenwell is of interest as illustrating the effect on small-pox
and other zymotic diseases of a good system of drainage, combined with abundant
open spaces. The Registrar found that there had been no epidemic prevalent in
his district since the commencement of registration (July 1, 1837). This is the
more remarkable as the opening years of registration were occupied with one of
the most disastrous small-pox epidemics of the present century. "The whole
district," he remarks, " with the exception of about a hundred houses, has been
built on since the year 1806; it is bounded on the south and west by spacious
streets ; on the north and east by two great roads, and through its centre runs
the high road to Islington. It contains three large squares, with the vast area
occupied by the New River-head. The whole district belongs to four great
proprietors, namely, the Marquis of Northampton, the New River Company, the
Brewers' Company, and the Skinners' Company, who secured by their building
leases as perfect a system of drainage as can probably be found in any part of
the Metropolis" (p. 527).
The Registrar of the north-west division of the City of London observed that at
"Christ's Hospital (occupied by eight hundred Blue-coat boys) there are not more
than one or two deaths in a year, the diet and hours being regular, and the
wards lofty and cleanly" (p. 542).
The Registrar of the St. Leonard's division of Shore-ditch, reported (p. 547)—"
The whole of my district has been particularly healthy during the last twelve
months, except in the winter of 1840 and 1841, when small-pox prevailed with
great fatality in New Court and Old Court, Hackney Road. They were the only
unhealthy parts of my district, the small-pox having been introduced into the
place by travelling gypsies and other vagrants occupying the huts in these
courts ; since which time they have been well cleansed and purified by the
parish authorities, and have since been in a very healthy state, and are well
supplied with water."
In the Church division of Bethnal Green the Registrar stated that the greatest
number of deaths in the unhealthy parts of his district took place from
smallpox, measles, scarlatina, whooping - cough, diarrhoea, influenza, and
typhus ; these places were entirely without drainage ; there was a great want
of cleanlinessi and with regard to the water supply there was but one hand-cock
to many houses. He observes that in many cases six persons occupied a room of
ten feet square by eight feet high (p. 551).
The Registrar of the Borough Road division of St. George, Southwark, observed
that there was scarcely a street or court in his district which had not been
visited by small-pox, measles, or whooping-cough. The supply of water was
plentiful, but drainage very deficient, cleanliness little attended to by a
great number, and there was extreme overcrowding (p. 580).
The Registrar of the Kennington district of Lambeth stated that small-pox was
most rife in Wandsworth Road, Spring Place, and the poor streets of South
Lambeth. The water supply was good, but drainage bad and the district dirty, and
in winter frequently inundated. The neighbourhood was also thickly populated,
from three to five persons sleeping in a room. In Hamilton Street in the
Wandsworth Road was a
filthy open ditch called the Corporation Common Sewer, which the Registrar
considered to be very unhealthy (pp. 586, 587).
The Report of the Registrar-General on the state of the public health in
different parts of England and Wales, during the year 1856, shows how the minds
of otherwise sensible people may overlook facts and be unconsciously warped by
the vaccination dogma. The Registrar of Bury South ascribes the entire absence
of small-pox "to the attention paid to vaccination," and the freedom from other
zymotic diseases " to the great improvement which has taken place in the last
ten years in the sewering, paving, and cleansing the streets, and to the
regulations under the Improvement Bill for common lodging-houses."1
In the Twentieth Annual Report of the Registrar-General, it is stated (p. xxiv.)
that " the deplorable neglect of sanitary measures, and the extent to which the
lives of the poor people of Dudley are sacrificed, . may be inferred from this
one appalling fact: 'smallpox was fatal in fifty-one cases.' " The
Twenty-second Report (p. xxiv.) states that " In the South Western division,
Wilts, Dorset, and Devon suffered an unusually high rate of mortality ;
scarlatina, diphtheria, and small - pox have proved fatal in many cases. '
Sanitary arrangements are far from good in many houses,' not only of Abbotsbury,
where three deaths occurred in one house over drains in the worst possible
condition, but it is to be feared in many other parts of these great counties."
1 Nineteenth Annual Report of the Registrar-General, p. xxxiv.
In 1864 the Registrar of the St. Helen's sub-district of Prescot writes to
the Registrar - General thus :— " The deaths exceed the average considerably.
The mortality has been greatest amongst children in consequence of the
prevalence of scarlatina and small-pox. One hundred and twenty deaths occurred
from scarlatina, and twenty-four from small-pox. Small-pox is most prevalent in
that part of the town noted for its defective sanitary arrangements, and
inhabited principally by the Irish. In this portion of St. Helen's, the evils
arising from want oi~ sewers, unpaved streets, small and unhealthy dwellings,
are still further increased by the crowding of several families in one house,
and an entire absence, apparently, of all ideas of cleanliness."1
In 1855, or about two years after vaccination was made compulsory, we have the
following notable words from Dr. Southwood Smith :—" Overcrowding, for example,
we can prevent ; the accumulation of filth in towns and houses we can prevent;
the supply of light, air, and water, together with the several other appliances
included in the all-comprehensive word Cleanliness, we can secure. To the extent
to which it is in our power to do this, it is in our power to prevent epidemics.
The human family have now lived together in communities more than six thousand
years, yet they have not learnt to make their habitations clean. At last we are
beginning to learn the lesson. When we shall have mastered it, we shall have
conquered epidemics."2
1 Twenty-seventh Annual Report of the Registrar-General, p. lxiv.
'A Two Lectures delivered at Edinburgh in November, 1855, entitled, " Epidemics
considered with relation to their common nature, and to climate and
civilisation," p. 23.
HOW SMALL-POX IS PROPAGATED. 25$
In 1871, during the great small-pox epidemic, several important testimonies crop
up in favour of the view that small-pox is controllable by sanitary measures.
Mr. Henry Carr, in a letter to the Times of February 9, 1871, under the heading,
"How small-pox is propagated," writes—■" I pray your insertion of the following
report of one visit of inspection among the habitations of the poor in
Westminster :—St. James's Court, St. Ann's Street. This is a blind court, no
thoroughfare and no through ventilation ; the entrance a narrow archway, three
feet wide ; the houses, two rooms each, opposite; the space between the opposite
houses not more than five feet; at the end of the court a dead wall, dust-heap,
etc. No back windows or doors. Only one closet for the whole court, and that at
times in most foul condition. At present in this court there are sixteen
families—sixty-five persons." Then follows a minute description of insanitary
horrors, coupled with abounding small-pox as the natural result. From a later
issue of the Times (February 15, 1871) it appeared that the authorities
inspected St. James's Court, and that the whole court was condemned as unfit for
human habitation.
In the Lancet of January 14, 1871 (vol. i., p. 6^), under the heading of "
Small-pox in Belfast," is the following :—" From a circular lately issued by
the Poor-Law Commissioners of Ireland relative to the spread of small-pox in
Belfast, we find that seventy-nine cases have occurred there, resulting in nine
deaths since March, 1870. The Commissioners point out to the Guardians of the
Belfast Union that, when the disease had been imported into other parts of
Ireland, it has
either not spread or quickly died out, and that its breaking out into an
epidemic at Belfast is probably owing to two causes—namely, the dangerous
sanitary condition of parts of the town, and the very defective state of the
vaccination."
In the same volume, under the date March 18, is an article by Dr. Grieve,
medical superintendent to the Hampstead Small-pox Hospital. In some concluding
remarks Dr. Grieve observes (p. 372)—" Bad as this epidemic when upon us may
appear to be, let us hope that it will bear fruits of good result. Already under
its pressure our sanitary reformers are on the move ; and the report of the
Sanitary Commission just comes in time. It is to be hoped that this epidemic of
small-pox will be the last of its kind ; that it will prove to be, as it were,
the boundary-stone placed to mark the place where the old rule of complete local
self-mismanagement was replaced by that of a proper centralisation under a
competent head ; and that the reign of confusion, in which Boards of Guardians,
Vestries, Local Boards, and other intractable bodies have to be coaxed and
wheedled into doing their duty, is fast drawing to an end. We look forward with
pleasurable anticipation to that time when under the firm rule of a Minister of
Public Health, sanitary measures will be judiciously and vigorously enforced,
and zymotic diseases—small-pox among the number— will be driven out of our
island as effectually as St. Patrick banished reptiles from Ireland."
Even from the writings of so pronounced a vaccine propagandist as Mr. Ernest
Hart is the following admission regarding an epidemic of small-pox at Douglas,
DR. FARR'S TESTIMONY. 257
Isle of Man, in 1877:—"The disease spread very rapidly, especially in the filthy
purlieus of the old town, until, between July 8, 1877, and March n, 1878, no
less than 257 cases occurred."1 It is true that Mr. Ernest Hart observes that
there was no system of compulsory vaccination in the Isle of Man, and thus a
number of the sufferers may well have been among the un-vaccinated, which only
shows from what class the unvaccinated are usually drawn, and how absolutely
unfair it is to compare their small-pox incidence and mortality with that of the
better fed, better housed, and more cleanly vaccinated population.
One of the greatest sanitary reformers, Dr. William Farr, has said that "healthy
sanitary condition as to food, drink, and cleanliness of person, house, and
city, stands first in importance ; after it, but subordinately, come quarantine,
vaccination, and other preventives, as means of subduing mortality ; for the
mere exclusion of one out of many diseases appears to be taken advantage of by
those other diseases, just as the extirpation of one weed makes way for other
kinds of weeds in a foul garden."2
Another eminent sanitarian, Sir Edwin Chadwick, maintained "that cases of
small-pox, of typhus, and of others of the ordinary epidemics, occur in the
greatest proportion, on common conditions of foul air, from stagnant
putrefaction, from bad house drainage, from sewers of deposit, from
excrement-sodden sites, from filthy street surfaces, from impure water, and from
over-
1 British Medical Journal, July 17, 1880, vol. ii., p. 78.
2 Supplement to the Thirty-fifth Annual Report of the Registrar-General
(1875), p. xli.
crowding in foul houses. That the entire removal of such conditions by complete
sanitation and by improved dwellings is the effectual preventive of diseases of
those species, and of ordinary as well as of extraordinary epidemic
visitations."1
The two following statements, printed within about six months of each other, if
taken together, almost entirely concede the case. The British Medical Journal
stated that " all sanitarians are agreed that insanitary conditions greatly
favour the spread of small-pox,"2 and Dr. W. B. Carpenter admitted "that in the
general mitigation of the type of this disease (small-pox), and in the enormous
reduction in its mortality which have taken place during the last hundred years,
the improved sanitary condition of our population (evinced by a reduction in the
general death-rate) has had a large share."3
Another authority, Dr. August Hirsch, maintained that " small-pox, as well as
typhus, takes up its abode most readily in those places where the noxious
influences due to neglected hygiene make themselves most felt."4
With reference to sanitation in Europe generally, the reader who is interested
in the subject may with advan-
1 Printed copy of address on "Prevention of Epidemics," pp. 22, 23.
Delivered by Mr. Edwin Chadwick, C.B., at Brighton Health Congress,
December 14, 1881.
2 British Medical Journal, October 21, 1882, vol. ii., p. 801.
3 The Nineteenth Century, April, 1882, p. 527.
4 " Handbook of Geographical and Historical Pathology," vol. i., p. 481,
by Dr. August Hirsch. Translation by Dr. Charles Creighton. London.
1883.
BERLIN PREVIOUS TO 1872. 259
tage consult a work by Dr. T. M. Legge on the Public Health in European
Capitals.1
It is claimed by Dr. Edwardes, Dr. Charles Drysdale, and Mr. Ernest Hart, with
endless reiteration, that the notable reduction of small-pox in Germany during
the last two decades is due to vaccination and compulsory re-vaccination. On
page 38 Dr. Legge observes that, prior to 1872, the drainage in Berlin was of
the most primitive description ; privies were in nearly every house ; open
drains, badly built, and with insufficient fall, ran through many of the
streets, and discharged their contents into the Spree, the pollution of which
became well-nigh intolerable. On page 10 he informs us that between 1871 and
1892 the Corporation of Berlin spent on buildings connected with public health,
including waterworks, drainage, sewage farms, hospitals, asylums, abattoirs,
disinfecting stations, night shelter, infirmary, and public baths, nearly
.Ł9,500,000, or, on an average, about ,Ł450,000 a-year. This large outlay
appears to have been judiciously expended, for on page 41 Dr. Legge says that,
since the introduction of the drainage works, the total mortality has declined
from 329 per 1,000 in 1875 to 20'2 in 1892, and he also points out the enormous
reduction in the mortality from typhoid fever during the period under review.
From the foregoing it is evident that neglect of sanitary measures is very
largely responsible for the prevalence and mortality of small-pox as well as of
other zymotic diseases. As the late Sir B. W. Richardson
1 " Public Health in European Capitals." Thomas Morison Legge, M.A., M.D.
(Oxon.), D.P.H. London. 1896.
most aptly puts it—"If by some magic spell, England could wake up to-morrow
clean, she would wake up pure also in spirit and godly in the comprehensiveness
of goodness. Cleanliness covers the whole field of sanitary labour. It is the
beginning and the end. Practised in its entirety it would banish all disease
from the world."
Another cause of the lessened fatality of small-pox is that better methods of
treatment are now in vogue than those which prevailed formerly. Anyone reading
the pages of Sydenham cannot fail to have been struck with the distressing
results of the treatment practised in his time. This was known as the hot
regimen. The patient was put to bed, the blankets were piled up over him, every
breath of fresh air and all light was carefully excluded from his room, and he
was plied with hot cordials.
This distinguished medical reformer protests against this treatment, and says—"
We must take especial care, lest the ebullition rise too high. This it may do
under the weight of blankets, under the over-heated state of the air in the
apartment of the patient, or under the use oi heating medicines and cordials;" 1
" From the use of your vaunted cordials, and from your hot treatment," he says,
" the pustules may be crowded together and rendered confluent."2 Again he
observes—"Had they (pustules) been left to their own pace they would merely have
been discrete, and the chances would have been better."''
1 "Medical Observations." The Works of Thomas Sydenham, M.D. Translation from
the Latin edition of Dr. Greenhill, with a life of the author, by R. G. Lathom,
M.D., vol. i., p. 134. Printed for the Syden ham Society. 1848.
-Ibid., p. 135. ■' Ibid., p. 139.
sydenham's treatment ok small-pox. 261
In speaking of his own more rational method of treatment :—" This is the true
and genuine method of treating this sort of small-pox, and however much it may
be opposed by the great and unfounded prejudice of the partisans of an opposite
practice, it is the method which will prevail when I am dead. I will not deny
that many have been treated on a different principle, and that under such
treatment they have recovered. On the other hand, it must be confessed that many
have died under it. And this, when we consider that the disease of the distinct
sort is in no wise dangerous of itself, is a sad reflection."1
Sydenham must have felt saddened at the prevailing ignorance when he wrote — "
Considering the practices that obtain, both amongst learned and ignorant
physicians, it had been happy for mankind, that either the art of physic had
never been exercised, or the notion of malignity never stumbled upon."2
Sydenham was greatly in advance of his age,3 and consequently was subjected to
the unmeasured opprobrium of his contemporaries.
1 " Medical Observations," vol. i., p. 142. Printed for the Sydenham
Society. 1848.
2 Letter to Mr. Robert Boyle, vol. i., p. lxxii.
■* Sydenham's writings are full of appeals to his colleagues to trust more to
Nature in the cure of disease. "Frequently, however, it is less from the
character of the morbific virus than from the effects of unskilful treatment
that such seventy has occurred. We often attend too little to the intentions of
Nature in the cure of disease, and set up on insufficient grounds some different
method of cure. From this arises a perturbation of the whole bodily economy,
and, this being upset, a melancholy state of things, worse than that of the
original disease, is induced." (Vol. i., p. 98.)
In referring to the pleasant sensations produced among his patients by
" To crown my misfortunes," he observes, " it has sometimes happened that, after
the standers-by had rejected my advice throughout the whole disease, I have
still been held answerable for the loss of the patient; and this has happened
after I have talked myself hoarse against the heating treatment of the friends
and nurses. For reasons like this, I have often thought that it would be better
for me never to undertake a case of small-pox, than to oppose the insuperable
prejudices of the 6'i iroWoi."1
In spite of the teachings of Sydenham, these barbarous methods of treatment
continued to prevail, for in the eighteenth century we find much the same state
the cool regimen, he observes—"This has often made me draw a difference between
the deceptions of reason (so-called) and the realities of our senses; from
whence I infer that—provided that they be not absolutely unreasonable, and
deadly—much more than is usually given should be allowed to the appetites and
sensations of the patients themselves. These are better than the treacherous
rules of art. E.g., a fever-patient ardently longs for cooling drinks freely
bestowed. Art denies them. Art has a theory of its own. Art has an end and aim
of its own. Art assumes that cool liquors are adverse to its doctrines; and so
starves an appetite, giving a cordial instead. The same patient loathes all
food, unless accompanied by diluent drinks. Art — the art of nurses and
lookers-on— contends that he must eat. After a long languor, he probably asks
for something absurd, or prejudicial, and asks earnestly. Art is again in the
way, and threatens death in case of disobedience—unless, indeed, the artist be
wise enough to remember Hippocrates:—More bad than good, whether food or drink,
if palatable, is preferable to more good than bad, if unpalatable. ... A man of
moderate medical practice, but of diligent observation, will freely own, that
many patients who have spurned physic and followed their own inventions, have
been the better for .doing so." (Vol. ii., pp. 67, 68.)
1 Letter to Dr. Cole. The Works of Thomas Sydenham, vol. ii., p. 66.
A PARALLEL. 263
of things recorded. Buchan,1 in his " Domestic Medicine," remarks on the
practice of confining the patient too soon to bed and plying him with warm
cordials and sudorific medicines, thereby increasing the number of pustules and
tending to make them become confluent. " The good women," he says, " as soon as
they see the small-pox begin to appear, commonly ply their tender charge with
cordials, saffron, and marigold-teas, wine, punch, and even brandy itself. All
these are given with a view, as they term it, to throw out the eruption from the
heart." Buchan also comments on the practice of crowding patients together,
which reminds us of the disgraceful state of things which prevailed at the
Gloucester Hospital in the recent epidemic. He says—" Laying several children
who have the small-pox in the same bed, has many ill consequences. They ought,
if possible, never to be in the same chamber, as the perspiration, the heat, the
smell, etc., all tend to augment the fever, and to heighten the disease. It is
common among the poor to see two or three children lying in the same bed, with
such a load of pustules that even their skins stick together. One can hardly
view a scene of this kind without being sickened by the sight. But how must the
effluvia affect the poor patients, many of whom perish by this usage?"
In a foot-note he remarks—" This observation is likewise applicable to
hospitals, workhouses, etc., where numbers of children happen to have the
small-pox at the same time. I have seen about forty children cooped
'"Domestic Medicine," pp. 241-244. William Buchan, M.D. Tenth edition.
London. 1788.
up in one apartment all the while they had this disease, without any of them
being admitted to breathe the fresh air. No one can be at a loss to see the
impropriety of such conduct. It ought to be a rule, not only in hospitals for
the small-pox, but likewise for other diseases, that no patient should be within
sight or hearing of another. This is a matter to which too little regard is
paid. In most hospitals and infirmaries, the sick, the dying, and the dead are
often to be seen in the same apartment." On the other hand, Buchan had seen poor
women travelling in the depth of winter, and carrying their children afflicted
with small-pox along with them, and had frequently observed others begging by
the wayside, with infants in their arms covered with the pustules; yet, he says,
" I could never learn that one of these children died by this sort of
treatment." He also observes—" A very dirty custom prevails amongst the lower
class of people, of allowing children in the smallpox to keep on the same linen
during the whole period of that loathsome disease. This is done lest they should
catch cold; but it has many ill consequences. The linen becomes hard by the
moisture which it absorbs, and frets the tender skin. It likewise occasions a
bad smell, which is very pernicious both to the patient and those about him;
besides, the filth and sordes which adhere to the linen being resorbed, or taken
up again into the body, greatly augment the disease."
Writing in the early part of the present century, Mr. John Cross,l in his
history of the Norwich small-pox
1 " A History of the Variolous Epidemic which occurred in Norwich in the year
1819," pp. it, 12. London. 1820.
THE EFFECTS OF FRESH AIR. 26$
epidemic, stated that the disease was often aggravated and made to assume its
worst characters by the most injudicious treatment. This was as follows:—"At the
commencement, to set the object before a large fire, and supply it plentifully
with saffron and brandy to bring out the eruption; during the whole of the next
stage, to keep it in bed covered with flannel, and even the bed-curtains pinned
together to prevent a breath of air; to allow no change of linen for ten or more
days, until the eruption had turned; and to regard the best symptom to be a
costive state of the bowels during the whole course of the disease."
The effect of fresh air—which the current practice excluded—in the treatment of
small-pox is illustrated by the following singular incident. In 1731 a fire took
place at Blandford, in Dorset. This was so violent and rapid that few had time
to save much, and many could save nothing. " The calamity," we are informed, "
was heightened by the small-pox raging in about sixty families; none of the sick
perished in the flames, but were removed under hedges in the fields, gardens,
and under the arches of the bridge, and but one died ;—a strong argument for the
cool regimen." 1
I should here like to quote the words of a lady who has probably done as much
for the mitigation of disease and human suffering as any person now living. I
refer to Miss Florence Nightingale, and the axiom I wish to impress is contained
in the following notable words:— " The very first canon of nursing, the first
and the last
1 "The History and Antiquities of the County of Dorset," vol. i., p. 76. John
Hutchins, M.A. London. 1774.
thing upon which a nurse's attention must be fixed, the first essential to the
patient, without which all the rest you can do for him is as nothing, with which
I had almost said you may leave all the rest alone, is this: to keep the air he
breathes as pure as the external air, without chilling him" x
There cannot be the shadow of a doubt that the displacement of the obsolete and
deadly methods described by Sydenham and others, by the fresh air and judicious
nursing which accompany the modern treatment of small-pox, and in which Miss
Florence Nightingale was such a distinguished pioneer, have had a potent
influence on its mitigation in recent years, although, for some occult reason,
vaccination (which, by the way, has been sensibly diminishing) has managed to
obtain all the credit.
One word with reference to the blindness produced by small-pox. We have always
been taught to believe, and statistics are ingenuously arranged to show, that
the diminution has been brought about by vaccination. Apparently this is not so.
One of the greatest authorities on small-pox informs us—"As to corneal
ulceration, this affection is probably not a part of small-pox, but is
accidentally associated with it. It occurs late in the disease, both in the
vaccinated and the unvaccinated, the prevention of permanent eye mischief
resulting more from altered methods of treatment, improved nursing, and hospital
hygiene, than from vaccination."2
1 " Notes on Nursing," p. 8. Florence Nightingale. London. 1876.
2 Dr. Birdwood's Evidence. Sixth Report, Royal Commission on
Vac
cination. Q. 31,146.
CHAPTER IX.
THE INJURIOUS RESULTS OF VACCINATION.
VACCINATION has been advocated and its enforcement recommended not only as an
absolute protection against small-pox, but as a safe and even benign operation,
and attended with no more danger than "the scratch of a pin," or, as a well -
known authority would have us believe, " it is not more harmful than piercing
the ears to place rings in them."1
In his petition to the House of Commons (1802), Jenncr claimed that cow-pox
"admits of being inoculated on the human frame with the most perfect ease and
safety, and is attended with the singularly beneficial effect of rendering
through life the persons so inoculated perfectly secure from the infection of
the small-pox."2
In the Report on Small-pox and Vaccination3 prepared by the Committee of the
Epidemiological Society, the report, it may be added, on which the first
compulsory Act of Parliament was based, it is stated (p. 4)—" We are ourselves
satisfied, and it is the concurrent and unanimous testimony of nearly two
thousand
1 "A Manual of Animal Vaccination," p. 153. E. Warlomont. Trans
lation by Dr. Harries. London. 1885.
2 Baron's " Life of Jenner," vol. i., p. 490.
3 Parliamentary Paper 434. Ordered by the House of Commons to be
printed, 3rd May, 1853.
medical men, with whom, as we have already stated, we have been in
correspondence, that vaccination is a perfectly safe and efficient prophylactic
against this disease."
Sir John Simon has identified himself with this position when he says that
against the "vast gain" by vaccination " there is no loss to count. Of the
various alleged drawbacks to such great advantages the present state of medical
knowledge recognises no single trace."1 Again he says—" I must say that I
believe it to be utterly impossible, except under circumstances of gross and
punishable misconduct, for any other infection than that of cow-pox to be
communicated in what pretends to be the performance of vaccination." 2
Elsewhere, Sir John candidly gives it as his opinion that, " If Government
could not reasonably guarantee that it gave pure vaccine lymph, it should not
force the public to accept it."s
Now, if it can be shown that there is no such thing known or obtainable as pure
lymph, setting on one side the question of its supposed protective value,
compulsory vaccination is totally unjustifiable.
Let us see what precautions the Government take to secure the purity pf lymph.
Mr. Farn, of the National Vaccine Establishment, when under examination before
the Royal Commission, furnished some interesting details, as follows :—
Q. 4,130. You are not a medical man, are you?—No.
1 " Papers relating to the History and Practice of Vaccination," p. lxvii. 1857.
" Ibid., p. lxiii.
3 Report from the Select Committee on the Vaccination Act (1867), 1871. Q.
3,458-
SOME DAMAGING ADMISSIONS. 269
Q- 4;I33- Have you made any special study of microbes ?—No.
O. 4,154. With such (microscopic) power as you are able to employ would you be
able to recognise or distinguish any micro-organisms which might be present
?—No, I should not.
O. 4,155. Have any micro-organisms been identified, or stated to have been
identified, for such a disease as erysipelas and so on?—I am afraid you are
going rather out of my depth as a non-medical man.
Q. 4,159. Is there any disease within your experience whose cause you can
identify with such microscopical power as you employ ?— Not that I am aware of.
Q. 4,173. Having regard to what you have told us, do you think it would be
possible, from the microscopical examination you made, to guarantee that any
lymph was pure ?— No ; I should not undertake to say whether it would be a
guarantee that the lymph was pure. I do not know that you could do it.
Q. 4,200. Are we to understand that, as a matter of fact, you have ever
guaranteed lymph ?—No.
It seems, therefore, that there is no such thing known or obtainable as pure
vaccine lymph, and it is very significant that as long ago as 1883 the Grocers'
Company, by reason of the numerous disasters following vaccination, offered a
prize of .Ł1,000 for the discover)' of any vaccine contagium cultivated
apart from an
animal body, but up to the present time the award has not been made. The matter
has, however, been settled beyond all dispute by the Royal Commission itself.
They say :—" It is established that lymph contains organisms, and may contain
those which under certain circumstances would be productive of erysipelas "
(Section 410).
With regard to the dangers attending vaccination, in the official tract,
entitled,"Facts concerning Vaccination for Heads of Families," is the following
(p. 3):— " As to the alleged injury from vaccination, all competent authorities
are agreed that, with due care in the performance of the operation, no risk of
any injurious effects from it need be feared."
That vaccination produces injurious results of a definite kind can be shown from
a very early period in the history of vaccination. The disease cow-pox itself,
as Dr. Edward Ballard has pointed out, is one that is not to be " trifled" with.
In describing the complaint in milkers, Jenner says :—" The system becomes
affected—the pulse is quickened ; and shiver-ings, with general lassitude and
pains about the loins and limbs, with vomiting, come on. The head is painful,
and the patient is now and then even affected with delirium. These symptoms,
varying in their degrees of violence, generally continue from one day to three
or four, leaving ulcerated sores about the hands, which, from the sensibility of
the parts, are very troublesome, and commonly heal slowly, frequently becoming
phagedenic, like those from whence they sprung."1 And,
1 " An Inquiry into the Causes and Effects of the Variolw Vacant," p. 5.
London. 1798.
IMPLANTING THE SEEDS OF A DISEASE. 271
in referring to the case of Sarah Wynne, he remarks:— " She caught the complaint
from the cows, and was affected with it (cow-pox) in so violent a degree that
she was incapable of doing any work for the space of ten days."
Again, in the case of Thomas Edinburgh, described by Dr. Pearson:—" He was so
lame from the eruption on the palm of the hands as to leave his employ, in order
to be for some time in a public hospital. . . . According to the patient's
description, the disease was uncommonly painful and of long continuance."2
That vaccination is, indeed, a serious matter has been fully recognised by the
late Dr. Ballard,3 one of Her Majesty's Inspectors of Vaccination. " Medical men
and parents alike should drive from their minds the idea so prevalent, that
vaccination is but a trivial operation at the most. . . . They should keep in
mind that in the act of vaccination they are not merely imparting a protection,
not merely performing a sort of magic rite, but that they are engaged, in very
truth, in implanting the seeds of a disease'.' The results have been described
by the Royal Commission as follows:—" The introduction into the system of even a
mild virus, however carefully performed, is necessarily attended by the
production of local inflammation and
1 Taken from Jenner's original paper, which was forwarded to the
Council of the Royal Society, and afterwards returned to him. See
Crookshank's " History and Pathology of Vaccination," vol. i., p 275.
2 " An Inquiry concerning the History of the Cow-pox," p. 15. London.
1798.
3 " On Vaccination : its Value and Alleged Dangers," p. 362. A Prize
Kssay. London. 1868.
of febrile illness" (Section 409). Elsewhere in the Report the Commissioners
affirm that " it is not open to doubt that there have been cases in which injury
and death have resulted from vaccination" (Section 399), and that the admission
that some risk attaches to the operation is one "which must without hesitation
be made" (Section 379).
Sir James Paget wrote in 1863 :—" The progress of the vaccine or variolous
infection of the blood shows us that a permanent morbid condition of that fluid
is established by the action of these specific poisons upon it. And although
this condition may, so far at least as it protects the individual from any
further attack of the same disease, be regarded as exercising a beneficial
influence upon the economy, yet it is not the less to be looked upon as a morbid
state. In forming an estimate of the persistent changes produced in the blood
by these and similar infectious diseases, we must not lose sight of the
influence which the tissues, themselves altered by the inoculation, exercise
upon the blood. They will necessarily re-act upon it, so as to assist materially
in preserving a permanent morbid, though beneficial condition."1 It is not
altogether clear how a permanent morbid condition of this vital fluid can be
beneficial to the animal economy, but it is worthy of notice that one of our
greatest living English surgeons has put it on record that the principle of
inoculation involves an unhealthy as distinguished from a healthy state of the
system.
1 " Lectures on Surgical Pathology," pp. 39, 40, foot-note. James Paget,
K.R.S. London. 1863.
SYMPTOMS ACCOMPANYING VACCINATION. 273
The general symptoms accompanying vaccination have been given in some detail by
Dr. Acland in his valuable contribution on vaccinal injuries to Allbutt's
"System of Medicine." Dr. Acland says:—"These are commonly unimportant;
sometimes a slight rise of temperature is noted about the third day after
inoculation ; this may be followed by remissions, and the pyrexia, if any
occur, reaches its maximum generally before the eighth day. These slight
disturbances are often the only evidence of a general diffusion of the virus,
although eruptions such as erythema, roseola, or urticaria may accompany even
the mildest and most favourable cases of vaccination. These rashes, which may
develop early in children who are unusually susceptible to the vaccine virus,
may occur within four or five days of inoculation, or they may develop during
the period of maturity and subsidence of the pocks; they have no special
significance, and, as a rule, are not harmful except in so far as they produce
irritation and consequent restlessness. Amongst the more usual complications
which occur at or about the period of the full development of the pocks are
those which are common in all the acute exanthems: they consist in headache (in
adults and in elder children), lassitude, irritability, sleeplessness,
disturbances of the digestive system—such as anorexia, vomiting, catarrhal
diarrhoea ; and possibly, during the onset of the vaccinal fever, rigors may
occur in adults and in the re-vaccinated, and convulsions in children. In
relation to these indications of a general infection in some instances there
will be evidence of a corresponding disturbance of the circulatory or
respiratory apparatus, as shown by increased
rapidity of pulse and respiration, bronchial catarrh, or slight temporary
albuminuria." 1
I wish especially to draw attention to the possibility of convulsions in
children supervening on vaccination, to which Dr. Acland has alluded; and
although it is difficult to prove in all cases that this condition is the direct
result of vaccination, the occurrence, and that not unfre-quently after
vaccination, has led to a belief that they are often in some way related to the
operation. (See fatal cases in Appendix ix. to Final Report of the Royal
Commission, more epecially Nos. vi., lv., cii., clviii., clxx., 45, 119, 123,
E.G. (p. 334), 216, and 223.)
Another result of ordinary vaccination is enlargement of glands, sometimes
giving rise to an abscess in the armpit. According to Dr. Louis Frank, "
Adenitis is quite a common complication of an otherwise normal course of
vaccination, and needs but a passing mention." 2 As this condition appears to
be of such frequent occurrence, one would like to feel a little more certain
that scrofulous affections do not sometimes arise in this way, as they are
admitted to do in connection with glandular enlargement associated with other
diseases such as measles.
Although it appears to be thought by many that injurious results from
vaccination are only of comparatively modern occurrence, a study of the older
writings on vaccination proves that this is very far from being the case.
In the year 1800 some cases of injury with one
1 Allbutt's " System of Medicine," pp. 562, 563. London.
1897.
2 Journal ofCutaneous and Genito-Urinary Diseases, New York,
April,
1895, vol. xiii., p. 144.
THE CLAPHAM CASES. 275
death were reported as having taken place in Thunderbolt Alley, Clapham.x
According to the narrative, the parents of some of the children were " much
prejudiced, full of invective, and refused to converse reasonably." In a report
signed by certain medical men, the symptoms produced were extensive erysipelas
rapidly spreading from the inoculated parts, accompanied in many instances by
considerable constitutional disturbance, and followed in most by an immediate
ulcerative process, and in some cases even a tendency to gangrene. Then, as now,
vaccination had its apologists. On this occasion Dr. Lettsom, a leading London
physician, undertook the office. " The disease," he said, " was not the
cow-pock, but morbid ulceration, originating from the purulent matter formed
under the scab or dried pustule of the cow-pock."
Mr. B. Maddock, of Nottingham,2 in bringing forward cases of injury, wrote that
he would be sorry to excite prejudices against the introduction of vaccination
as a substitute for small-pox inoculation, but he had to lament that its
advantages were somewhat overrated when it was said, on respectable authority,
that it was a disease free from danger. " It is a great misfortune," he said, "
that proselytes to new systems do not always carefully examine into opinions
handed down from high authority, but give them implicit credit; and it is
equally unfortunate, that, in the recommendation of any new doctrine, the
unfavourable symptoms are too
1 London Medical Review and Magazine, January, 1801, vol. v., pp. 276-289.
'* Medical and Physical Journal, February, 1801, vol. v., p. 161.
frequently placed in the background, and only the more pleasing ones exposed to
public view."
In November, 1805, the editors of the Medical and Chirurgical Review,1 in
referring to cases of injury recorded in the minutes of the Vaccine-pock
Institution, observe:—"This case, with others to be found in these reports,
serves to show that constitutional affection makes an essential part of the
vaccina as well as of variolous inoculation ; it proves also that the disorder
is occasionally severe, contrary to what some have -asserted."
Dr. Robert Willan, a supporter of vaccination, in an early work on the subject,
also noticed that the results of the new inoculation were occasionally severe.
He writes:—" There may also be a few in which the inoculation excites a new mode
of action, terminating in erysipelas, phaged,enic ulcer, or other morbid
appearances not necessarily connected with the specific disease. Several of
these anomalies or exceptions to the general rule have occurred, but certainly
not so often as was expected by those who considered the subject, from the
first, dispassionately, nor have they been in sufficient number to form any
serious objection to the practice founded on Dr. Jenner's discovery."2
On December 15, i8o6,the Royal College of Surgeons3
1 Medical and Chirurgical Review, vol. xii., p. Ixxvii., footnote.
2" On Vaccine Inoculation," pp. 20, 21. Robert Willan, M.D. London. 1806.
3 Report of the Royal College of Physicians of London on Vaccination, with an
Appendix, containing the opinions of the Royal Colleges of Physicians of
Edinburgh and Dublin; and of the Royal Colleges of Surgeons of London, of
Dublin, and of Edinburgh, pp. 10, 11. Ordered to be printed, 8th July, 1807.
THE COLLEGE OF SURGEONS' REPORT. 277
addressed a letter to their members on the subject of vaccination, among other
questions asking them for the number of vaccinations they had performed, and for
information about any injurious results in their practice. The replies, when
summarised, showed that out of 164,381 vaccinated there were 66 cases of skin
eruptions and 24 cases of inflammation of the arm, of which 3 proved fatal. The
College reported that in the Metropolis vaccination was on the decrease, and
they assigned the following reasons :—
(1) Imperfect vaccination.
(2) Instances of small-pox after vaccination.
(3) Supposed bad consequences.
(4) Publications against the practice.
(5) Popular prejudices.
Sir John Simon, in his classic " Papers relating to the History and Practice of
Vaccination," while printing the College of Physicians' report, which was
strongly favourable to vaccination, omitted any reference to the appendix
containing the report of the Royal College of Surgeons.
In 1808 Dr. Richard Reece wrote—"Even if the cow-pox did afford a certain
security against small-pox infection, as Dr. Jenner has represented it, it would
still remain a question whether the human race would really be benefited by its
universal adoption, since the cutaneous eruptions that have followed have in
many instances proved more fulsome than even small-pox itself. That those
eruptions do occur after cow infection must be allowed by its most strenuous
advocates, being perfectly novel, of a nature unknown before the
introduction of vaccination, and peculiar to those who have been vaccinated, and
often so inveterate as more than to counterbalance the trivial advantages that
we were first led to expect from its introduction." Again he says—"It must be
allowed that the local inflammation excited by the inoculation with this
matter, is of a very unfavourable nature, and often ends in a deep sloughing,
frequently producing such an adhesion of the muscles of the arm, as very much to
confine its motions; and some instances have occurred of the mortification
spreading, so as to destroy the life of the child ; an instance of which
happened in St. George's Fields. The child was inoculated at the Cow-pox
Institution, Salisbury Square, Fleet Street; the inflammation of the arm
exceeded its usual boundary ; on the sixth day mortification ensued, which
proved fatal to the child."1 In the Medical Observer11 for September, 1810, Dr.
Charles Maclean gives a list of sixty cases of vaccinal injuries, with the names
and addresses of ten medical men, including two professors of anatomy, whose
families had suffered from vaccination. In the London Medical Gazette for
December 21, 1833, Mr. Charles Fluder reported that " Five children were
recently vaccinated from the arm of a healthy child, which had been vaccinated
about a week previously. Each of these children became the subject of much
constitutional disturbance almost immediately ; their arms were enormously
swollen and cedematous; one
1 See Article on "Cow-pox," in "A Practical ] dictionary of Domestic
Medicine." Richard Reece, M.D. London. 1808. ''■Medical Observer, vol.
viii., pp. 195-197.
"THE LANCET" IN 1854. 279
child had convulsions ; in two of them abscesses formed ; and in all there was
an alarming degree of febrile excitement."1
The Lancet for July 15, 1854 (vol. ii., p. 35), remarks in a leading article :—"
There is a belief—it may be denounced as a prejudice, but it is not the less a
deeply-rooted conviction, and one not confined to the poor or the ignorant—that
if the vaccine disease may be transmitted by inoculation, other diseases less
beneficial may be propagated in the.same manner, and by the same operation.
Many a parent of high and low degree dates constitutional disease in her
offspring to vaccination with ' bad matter.' Who shall say that this etiological
conclusion is always false?" In the number for October 28, 1854 (vol. ii., p.
360), it is stated :—" The poor are told that they must carry their children to
be vaccinated by medical men who may be strangers to them. They apprehend—and
the apprehension is not altogether unfounded, or unshared by the educated
classes—that the vaccine matter employed may carry with it the seeds of other
diseases not less loathsome than the one it is intended to prevent." On November
11, 1854 (vol. ii., p. 404), it says :—" So widely extended is the dread, that
along with the prophylactic remedy something else may be inoculated, lest the
germ of future diseases may be planted, that few medical practitioners would
care to vaccinate their own children from a source of the purity of which they
were not well assured."
In 1869 Dr. Felix von Niemeyer writes:—"It cannot be denied that it
(vaccination) sometimes endangers life,
1 London Medical Gazette, vol. xiii., pp. 440, 441.
and in other cases leaves permanent impairment of health, especially cutaneous
eruptions, and other scrofulous affections."1
In 1880 Dr. Benjamin Bell writes as follows :—" Every man," he says, " who has
seen much of the kind of persons who apply to dispensaries and vaccine
institutions must have an impression, perhaps indefinite, but still reasonable,
that hereditary disease may be communicated by the channel of vaccination.
Children are brought very properly to such institutions, manifesting distinct
indications of syphilitic and scrofulous disease. Are these indications always
recognised ? And is lymph never taken from the arms of such children? My own
belief is, that many mothers speak correctly when they tell us that their child
was poisoned when it took the cow-pock. I have seen such cases, and their
existence cannot be doubted since the publication of Mr. Jonathan Hutchinson's
valuable series of cases."2
In 1880 a Select Committee of the Legislative Assembly of the Colony of Victoria
was appointed to inquire into the subject of vaccination. After recording the
"conflicting and contradictory" testimonies of medical men examined by them with
regard to length of time vaccination protects, the requisite number of marks,
etc., the Committee came to the conclusion that " Greater unanimity prevailed on
the question of the communication of extraneous diseases, such as syphilis and
scrofula by vaccination; although some of the
1 Dr. Felix von Niemeyer's "Text-Book of Practical Medicine," vol. ii., p. 557.
Translation by George H. Humphreys, M.D., and Charles E. Hackley, M.D. New
York. 1869.
^Edinburgh Medical Journal, May, 1880, vol. xxv., p. 976.
witnesses maintained that there would be no liability to such transmission
unless blood were drawn during the operation. Dr. Beaney and Dr. Sparling,
however mentioned instances, that came under their observation, of syphilis and
erysipelas being communicated to children from purely colourless vaccine matter
which contained no trace of blood." 1
That the disease—cow-pox in itself—is sufficient to cause death to a weakly
child, is shown by the fatality due to calf lymph recorded by Dr. Farrar, in the
British Medical Journal of October 13, 1894 (v°l- "■> P- 807). After describing
the case, Dr. Farrar says:—" I consider her death to have been due to a
constitutional malaise, induced by vaccinia in a poorly nourished child." Dr.
Farrar very rightly publishes the case as a warning to vaccinators to avoid
vaccinating weakly children; and if it be dangerous to vaccinate weakly
children, it is surely so in the case of the newly-born ; and yet this
objectionable practice is in vogue in workhouses, and moreover, it is
encouraged by the Local Government Board, as will be seen from the following
letter.
" Local Government Board, Whitehall, S.W., " 27th January, 1881.
" Sir,—I am directed by the Local Government Board to state that their attention
has been called, in connection with the state of vaccination and the present
prevalence of small-pox in the Metropolis, to the large proportion of children
who, having been born in workhouses, are discharged with their mothers before
1 Report lroni the Select Committee upon Vaccination Law, together with the
Proceedings of the Committee, Minutes of Evidence, and Appendices. Ordered by
the Legislative Assembly to be printed, 24th March, 1881.
being vaccinated, and many of whom escape vaccination altogether because the
vaccination officer has no means of tracing them.
" i. The Board are desirous of being informed as regards the several workhouses
and poor law infirmaries in the Metropolis, how many children were born in each
during the year 1880, and how many of those so born were discharged before being
vaccinated or before the vaccination has been ascertained to be successful, and
I am to request that you will have the goodness to furnish the Board with this
information as respects any such poor law establishments under the control of
the Guardians.
" 2. I am at the same time to state that some Boards of Guardians have passed a
resolution requiring the medical officer, subject to the exercise of his
judgment as to making exception in particular cases, to secure the vaccination
of all children born in the workhouse as soon as possible after birth, and it
has been found practicable as a rule to vaccinate the children when six days old
and to inspect the results on the thirteenth day, as the mothers in such cases
rarely leave the workhouse within a fortnight after their confinement. The Board
would be glad to learn whether the Guardians have directed the adoption of this
practice.
" 3. The Board also request that they may be informed whether a specific fee is
paid to the medical officer of each workhouse or infirmary for every vaccination
or re-vaccination successfully performed by him.
" I am, Sir,
"Your obedient Servant,
"John Lambert, Secretary."
The following is a case in point. At an inquest held on December 8, 1882, on the
body of Lilian Ada Williams, born in St. Pancras Workhouse, and vaccinated on
the seventh day after birth, the jury found "that the death was caused by
suppurating meningitis, following ulceration of vaccine vesicles on the arm,
and they were of opinion from the results of the post-mortem examination that
the vaccination of the child ought to have been postponed."
VACCINATION OF YOUNG INFANTS. 283
Such instances are by no means rare, as disclosed in Appendix ix. to Final
Report of the Royal Commission, one of the most flagrant cases there reported
being a fatal one of pyaemia in a " puny and probably syphilitic " seven months
child weighing 4.1bs. 2ozs., and vaccinated when less than two days after birth.
(No. cxxi.)
With regard to the most suitable age for vaccination, the profession does not
appear to be altogether unanimous. The following from one of the leading
authorities of the last century, with reference to the best age for inoculation,
may possibly be of interest in guiding us at the present day. Dr. Percival, in
citing arguments against the inoculation of children in early infancy, remarked
that " Nature, weak and feeble as she then is, can scarcely struggle with the
diseases to which she is ordinarily exposed ; it is therefore equally cruel and
unjust, to add to the number with which she is already oppressed."r It is also
interesting to notice that in a communication from the Government of Norway)
appended to Sir John Simon's " Papers," it is stated:— " Experience has taught
us that in the great majority of cases vaccination may be performed without
danger in the earliest infancy; but the experience of the ("ommittee, as well as
that of several other medical men, has also shown, on many occasions, that
infants, ;iflcr vaccination, do not unfrequently become sickly in various ways.
As it hardly ever happens that the first: case of epidemic small-pox occurs in a
child, the
1 Article on the "Arguments against the Inoculation of Children in Karly
Infancy," by Thomas Percival, M.D., F.R.S. Gentleman's Magazine, vol. xxxviii.,
p. 162. London. 1768.
Committee (particularly on account of the difficulty of control), in their
proposal for a new law on vaccination, have not hesitated to recommend
deferring it until school-time begins."1
The Vaccination Commissioners are not quite so accommodating, but their
recommendations are in the same direction, and it is certainly rather
significant that after forty-two years with a compulsory age-limit of three
months the Commission recommend extending the time to six months. The reasons
they give are unassailable. " Looking at the circumstance that the tenure of
life in children of a very early age is frail, and that where a disease
supervenes upon vaccination the ability to battle against it may determine
whether the result is fatal or not, or to what degree injurious, we should a
priori think that the chances of death or injury from such a cause would be
less, looking at the matter as a whole, when the age of the child was more
advanced." (Section 438.) And they further think that, provided the children
coming within the range of the present compulsory law could be vaccinated on the
occasion of the introduction of small-pox into the district, the "age might be
advantageously extended to one year from the date of birth, and that the number
of cases in which death was, whether correctly or not, attributed to vaccination
would then much diminish." (Section 440.)
Vaccine Generalisee.
This name has been given to a widely-spread eruption of vaccine vesicles on
different parts of the body, the
1" Papers relating to the History and Practice of Vaccination,"
Appendix, p. 187. 1857.
VACCINE GENERALISES. 285
lesions being identical in character with the typical vesicle, and containing an
inoculable fluid. Some of these are doubtless cases of auto-inoculation from the
original sore, but the remainder are examples of true, specific generalised
cow-pox eruption. A case is related by Dr. Martin, of Boston, in the Medical
Record^ of April 15, 1882, where there were four hundred clearly defined,
perfectly circular, invariably umbilicated vesicles. According to Dr. Prince A.
Morrow, numerous examples of generalised eruption have been recorded by
experienced vaccinators, and we also have it on his authority that "French
vaccination literature, especially, abounds in cases of this character." 2
In this country, apparently, the complication is not so common, but a few cases
are given in Appendix ix. to Final Report of the Royal Commission. (See Nos.
li., clxii., cxciv., 109, 173, and 214.) Anyone wishing to see how serious this
disease may really be will do well to consult the coloured drawing of the fatal
case figured by Dr. Acland in the Transactions of the Clinical Society.3 (No.
214 of Vaccination Commission Cases.)
Skin Diseases.
Of the various diseases alleged to be induced by vaccination, skin disease takes
an important place. How common is the mother's remark that the child never had
a blemish until it was vaccinated! And,
1 Medical Record, vol. xxi., p. 393. New York.
2Journal of Cutaneous and Venereal Diseases, vol. i., p. 173. New York, March,
1883.
3 Transactions of the Clinical Society, vol. xxvi., p. 114. London. 1893.
according to Dr. Robert Lee,1 it appears that there is some foundation for
the allegation. He found, from an experience of three thousand cases of skin
disease treated at Great Ormond Street Hospital, that in three hundred, or 10
per cent, the mothers attributed the rash to vaccination, and Dr. Lee thought
that we were not justified in pooh-poohing the notion; and there can be but very
little doubt that Dr. Lee is correct in his surmise, and for this reason, viz.,
that a secondary rash, as in syphilis, is not unfrequently part and parcel of
the disease cow-pox. Mr. Robert Ceely, in describing the casual disease in
milkers, says:—" Papular, vesicular,and bulbous eruptions, are occasionally seen
attendant on casual cow-pox, especially in young persons of sanguine temperament
and florid complexion, at the height or after the decline of the disease. They
are generally of the same character as those known to attend the inoculated
disease."2 Again, in writing about the inoculated disease when primary lymph is
used —" about this stage of the areola, especially on children, small
supernumerary vaccine vesicles in miniature often appear within its limits,
sometimes on the shoulder, and still more rarely on the face and body. The
well-known papular, vesicular, and bulbous eruptions, occurring in such subjects
are frequently observed."3
With regard to cutaneous affections, the Vaccination Commissioners say (Section
418)—"It is to be freely admitted that vaccinia, like varicella, does
occasionally
1 Sixth Report, Royal Commission on Vaccination, pp. 564, 565.
2 The Transactions of the Provincial Medical and Surgical Association,
vol. viii., p. 337. 1840.
3Ibid., p. 346.
SKIN ERUPTIONS. 287
Cause an irritable condition of the skin, which may last long."
1 The complication of skin disease, and that not un-^requently, was noticed very
early in the history of \iaccination. Thus, Mr. Thomas Wainwright, in the
Medical and Physical Journal {ox November, 1805 (vol. xiv., p. 435), in
reviewing a vaccination experience of tiree thousand cases, observes that
"Various kinds of obstinate cutaneous eruptions are not unfrequently consequent
to the vaccination of young children ; but they tery rarely take place in those
who have the cow-pock at the age of ten years, or at any later period." We also
have it on the authority of Dr. Robert Willan that " during the progress of the
vesicle some disorder takes place in the constitution, and there is frequently
on the arms and back a papulous eruption resembling some forms of the lichen and
strophulus." x
Mr. Ross, in a paper read before the Medical Society of London, on February 7,
1857, drew the attention of the profession to the occurrence of secondary
eruptions following vaccination. These generally appear after the eighth day. "
No experience," Mr. Ross concludes, " on this matter can be worth much that is
limited to an observation of the pock on the eighth day,2 as is the ordinary
practice in public institutions. Hence I do not regard as of any weight the
objections of those gentlemen who, with such an experience, have denied
1 " On Vaccine Inoculation," p. 10. Robert Willan, M.D., London. 1806.
- See also remarks by Dr. Hugh Thomson at the Birmingham meeting of the British
Medical Association, British Medical Journal, November 29, 1890, vol. ii., p.
1231.
the existence of a special secondary eruption. Being Public Vaccinator for an
extensive district, I vaccinatd a considerable number of children every week, at
th? present time, yet from never watching the cases afteb the eighth day, I
rarely hear of instances of secondary eruption ; but I have not the slightest
doubt that I should discover them, as frequently as heretofore, if I followed
the cases up as I did when I was conducting these investigations. I think that I
have now adducejd evidence sufficient, if not to convince absolutely, at least
to induce a strong presumption in the mind of an un\-biased man, that vaccinia,
under certain circumstances^ is followed by a secondary eruption, special in its
nature, though various in forms, which observes fixed periods of evolution, and
is an integral part of the original affection." 1
A considerable discussion followed the paper, and, in reply, Mr. Ross observed
that the " external character of the eruptions differed, but in their nature he
believed they were specific—in fact, sui generis; that they were directly caused
by the vaccination, and were evolved by the actions going on in the economy,
though it might be difficult to explain those actions."2 Dr. Louis Frank has
testified that " the skin diseases attributed to vaccination are exceedingly
numerous," and he adds, " there can hardly be any doubt in the minds of those
who have had great experience in vaccination that there exists an intricate
connection between vaccination and cutaneous eruptions as a sequel thereof."3
Dr. William C. Cutler,
1 Lancet, February 14, 1857, vol. i., p. 166.
2 The Medical Circular, February II, 1857, vol. x., p. 68.
3Journal of Ctitaneous and Genito- Urinary Diseases, April, 1895, vol. xiii., p.
142.
MR. HUTCHINSON'S OPINION. 289
in discussing the various forms of injury incident to vaccination, remarks that
" vaccine roseola or lichen is so often met with in the practice of all
physicians that it hardly needs to be mentioned in this connection."x Indeed,
Mr. Jonathan Hutchinson has probably not overstated the case, when he says that
" the wonder is not that vaccination should sometimes produce an exanthem, but
that it should ever be without one."2
Dr. P. A. Morrow, in alluding to the frequency of vaccinal eruptions, quotes the
experience of Behrend, who only observed them six times in three hundred
successive cases, and says—" From the unusually large number of cases reported
in the various medical journals within the last few years, I should judge that
the proportion was much greater."3 He remarks that, preceding and accompanying
erythematous eruptions, there may be slight febrile reaction, headache, malaise,
and other evidences of constitutional disturbance. Dr. Acland has also testified
that vaccinal eruptions are " often attended with much irritation, considerable
general disturbance, and some pyrexia."4 Now, if these eruptions are an integral
part of the vaccine disease, and often attended with constitutional disturbance
and much irritation, even if they are usually characterised by a temporary
duration, as stated by Dr. Acland, I
1 Annual Report of the Health Department of the City of
Baltimore, for
the year 1883, p. 62.
2 " Lectures on Clinical Surgery," vol. i., p. 18. Jonathan
Hutchinson,
F.R.C.S., London. 1879.
3'Journal of Cutaneous and Venereal Diseases, vol. i., p. 176. New York,
March, 1883.
4Allbutt's "System of Medicine," vol. ii., p. 564. London. 1897.
cannot help thinking that all this offers a somewhat serious objection to the
practice of vaccination.
Occasionally these eruptive disorders may prove more virulent. Thus, Professor
Hardy, of Paris, at the International Medical Congress held in London in 1881,
related an unpleasant reminiscence of which he was the subject in 1870. Three
days after being re-vaccinated he was attacked by an intense urticaria,
developed on the skin and in the bronchial mucous membrane, in the latter
situation exciting attacks of suffocation so serious as to put his life in
danger.1 We have it on the high authority of Drs. Colcott Fox and Louis Frank
that this complication of vaccination (urticaria) is not at all uncommon.2
With regard to eczema, there can be but little doubt that quite a large number
of cases are attributable to vaccination. In an article on "Vaccinal Skin
Eruptions" Dr. George Thin says—"All practitioners of any experience must be
able to recall cases in which obstinate eczema in infants has first shown itself
after vaccination, and other ailments of a general character are probably
sometimes produced by the effect of the vaccine virus on the system in delicate
persons. During the late epidemic of small-pox in London I had occasion to meet
with several cases in which patients attributed a temporary condition of
depressed health to re-vaccination.3
The following gives the age - distribution of eczema cases during the first year
of life coming under the care
1 Transactions of the Seventh Session of the International
Medical
Congress, vol. iii., p. 158. London. 1881.
2 British Medical Journal, November 29, 1890, vol. ii., p.
1235; and
Journal of Cutaneous and Genito-Urinary Diseases, April, 1895, vol. xiii.,
p. 145.
3Edinburgh Medical Journal, December, 1881, vol. xxvii., pp. 52J, 524.
EXPERIENCE OF DR. COLCOTT FOX. 291
of Dr. Colcott Fox1 at the Paddington Green Children's Hospital:—
Cases. Cases.
o - 1 month ... 33 6-7 months ... 10
1-2 months ... 22 7-8 months ... 4
2-3 months ... 25 8-9 months ... 23
3 - 4 months ... 39 9 - 10 months ... 1
4 - 5 months ... 23 10-11 months ... 1
5 - 6 months ... 7 11 -12 months ... 3
The large proportion under three months of age seems to afford ground for
believing that vaccination is not to be held responsible for the majority of
cases of infantile eczema. At the same time, as Dr. Acland2 says, it must be
noted that there is definite increase in the numbers in the fourth and in the
ninth months, at periods when the irritation of vaccination and teething
respectively might be expected to come into play. For cases recorded in Appendix
ix. to the Commissioners' Final Report, see Nos. xcix., cxi., 14, 15, 25, 95,
98, 101, B. S. and J. W. (p. 282), 120, 130, 140 (three cases), 192, B. R. (p.
389), 225, A. H. and A. G. (p. 444).
A disease of the skin which has been especially referred to by the Vaccination
Commissioners is impetigo con-tagiosa. The frequent occurrence of this malady
after vaccination has been remarked on by the late Dr. Tilbury Fox3 and others.
An extensive epidemic of impetigo contagiosa was occasioned by vaccination in
the Isle of Riigen* in 1885 ; 79 children were vaccinated on
1 liritish Medical Journal, November 29, 1890, vol. ii., p. 1235. -Allbutt's
"System of Medicine," vol. ii., p. 580. London. 1897. :) British Medical
Journal, May 21, 1864, vol. i., p. 553. 4O. 9,797-9,834, Third Report, Royal
Commission on Vaccination.
June II with humanised thymos-lymph obtained from a Government establishment at
Stettin ; all, with three exceptions, were attacked with impetigo contagiosa,
and, by infection, the disease was spread to 320 out of a population of 5,000
inhabitants. A Commission of Inquiry was appointed by the German Government, who
reported that they were unanimously of opinion that the outbreak of the disease
had been a direct consequence of vaccination.1
Skin eruptions from vaccination are not unfrequently complicated with intense
irritation. A case of this nature is recorded by Mr. Jonathan Hutchinson.2 The
patient (aged 13) was vaccinated when nine months old, and the eruption began
within a fortnight, and had been increasing ever since (twelve years). Mr.
Hutchinson was told that the patient would sometimes lay awake most of the night
scratching herself. Weather and seasons made no difference, and " the eruption
itched intolerably and incessantly." Mr. Hutchinson adds that the vaccine
eruption and that of varicella appear to be alike in their proneness to evoke
prurigo. " No year," he says, " passes but brings before me fresh examples of
the causation referred to."
■'Extensive outbreaks are also reported by Protze (see " Viertelgahres-schrift
fur Dermatologie und Syphilis," vol. xx., pp. 478,479, Vienna, 1888); by
Melichar in Allgemeine Wiener Medizinische Zeitung, December 10, 1889, vol.
xxxiv., pp. 581, 582; by Perron, Pourquier, and others. See also Nos. ex., 9,
12, 19, 20, 29, 82, 129, 180, M.C.B. (p. 368), 196, and 230 in Appendix ix. to
Final Report of the Royal Commission on Vaccination, and cases at St. Pancras
Workhouse in 1890-91, reported in Archives of Surgery, vol. iii., pp.
206-215. January, 1892.
2 Archives of Surgery, October, 1889, vol. i., pp. 161-162. Jonathan Hutchinson,
LL.D., F.R.S.
M. RICORD ON VACCINATION. 293
Syphilis.
With regard to the communication of syphilis by vaccination, Professor Ricord
declared in a lecture at the Hotel Dieu that "if it be true that vaccination can
transmit syphilis, then vaccination is done for. For who, pray, will run the
risk of being affected with the great to escape the small pox."x
These ominous words from the greatest authority on the subject of syphilis may
well have occasioned dismay among the promoters of vaccination, and thus we find
that medical literature was, and up to quite recent times has been, full of
denials of the possibility of such an occurrence. The official tract before
referred to informs us (p. 4) that " The fear that a foul disease may be
implanted by vaccination is an unfounded one. Such mischief could only happen
through the most gross and culpable carelessness on the part of the vaccinator.
. . . The alleged injury arising from vaccination is, indeed, disproved by all
medical experience'"1
To illustrate the sceptical attitude of the medical press on this subject, the
British Medical Journal of December 21, 1861 (vol. ii., p. 666), in referring to
a report in an Italian medical journal of children syphilised by vaccination at
Rivalta, heads the article "An Absurd Tale," and says in conclusion— " We need
hardly add, that our main object in referring to this matter is not so much to
warn the profession
1 Lecture delivered at the Hotel Dieu. Translation by Dr. Heron Watson,
Edinburgh Medical Journal, vol. vii., p. 859. (March, 1862.)
3 "Facts concerning Vaccination for Heads of Families." (Revised by the Local
Government Board, and issued with their sanction.)
against such a tale, as to enable our brethren to give an answer concerning it
to those of the ignorant public who may be frightened by it. It is unfortunately
true that there are only too many strangely-minded people who will be glad to
make capital against vaccination out of such a tale."
But, in spite of all denials in the past, the matter has now been placed beyond
dispute by the leading authorities on this subject.
Mr. James G. Beaney, of Melbourne, in his work on "Constitutional Syphilis,"
says — "And I at once announce at the outset my firm belief that syphilis is in
very many instances communicated by means of ' child's vaccine lymph.' This
opinion I have deliberately formed, and as firmly defend. The evidences of such
being the case have, in my practice, been numerous and well-pronounced; so
distinct, indeed, that no doubt whatever could exist as to the nature of the
eruptions, and the certainty of transmission."1
M. Fournier, Professor of the Faculty of Medicine of Paris, in discussing the
subject, remarks—" From that which precedes, it results in the first instance,
and quite clearly, that in a general way a real and serious danger is contained
in vaccination. But that danger, surely, is quite of a nature to evoke our
solicitude for a number of reasons. For (i) every individual is destined to
undergo, one or several times in his life, the vaccine inoculation. The danger
then of vaccinal syphilis is encountered by all the world once or several times
in the course of existence; (2) the excessive and ever-
1" Constitutional Syphilis," p. 373. James George Beaney, M.D., F.R.C.S.
Melbourne. 1880.
MR. BRUDENELL CARTER'S OPINION. 295
increasing diffusion of syphilis in modern societies will only increase
numerically the risks of that danger; (3) the syphilis which attacks subjects
quite young (that is to say, which invades the organism at the usual age at
which vaccination is practised) is particularly grave, everyone knows it, and
grave to the extent of terminating it in a fatal manner on many occasions."1
Dr. Edward Ballard, in his " Prize Essay" (p. 344), informs us that "the thing
has happened over and over again in cases which may now be counted by hundreds;
so that this disposes for ever of the cry of' impossible,' " and therefore Dr.
Charles Drysdale was probably not very wide of the mark when he said—"I think
there can be no doubt in the minds of instructed and unprejudiced medical men
that syphilis has occasionally been rather widely propagated by means of
vaccination."2
One of the most serious charges which has ever, probably, been made against
vaccination was made by Mr. Brudenell Carter, the well - known oculist. He
says—" I think that syphilitic contamination by vaccine lymph is by no means an
unusual occurrence, and that it is very generally overlooked because people do
not know either when or where to look for it. I think that a large proportion of
the cases of apparently inherited syphilis are in reality vaccinal; and that the
syphilis in these cases does not show itself until the age of from eight to ten
years ; by which time the relation between cause and effect is apt to be lost
sight of."3
1 " Lecons sur la Syphilis Vaccinale," pp. 17, 18. Alfred Fournier. I'aris.
1889.
- Medital Press and Circular, March 8, 1876, vol. i., p. 194.
:l Mr. Carter's statement was communicated to the North London Medical Society
by Dr. Kesteven in a Paper read on May 8, 1877. Medical Examiner, May 24, 1877,
vol. ii., p. 409.
The following is a list of alleged cases of vaccino-syphilis which have been
reported from time to time :—
Alleged Cases of Vaccino-Syphilis.
Year. Place. No.
Authority and Reference.
1814 Udine 30 Marcolini. " Annali Universali
di
Medicina," vol. xxix., pp. 146-150, Milan, January, 1824.
1821 Cremona 40 Cerioli. See "Revue Medicale Fran-
chise et Etrangere," vol. iii., pp. 54, 55, Paris, September, 1845.
1830 Frederiksborg 7 Ewertzen. " Notizen aus dem Gebiete
derNaturund Heilkunde" (Froriep's Notizen), vol. xxxiv., p. 303, September,
1832.
1841 j Cremona 64 Cerioli. Ibid.
1843 Quers (Haute- About Alies. " La Revue Medicale Fran-
Saone) 30 9aise et Etrangere." vol. i., pp. 29-
33, January 15, 1865.
1845 Constantine 3 See Layet. Traite pratique de la Vac-
cination Animate, p. 70, Paris, 1889.
1849 Piedmont 2 Viani. " Gazette Medicale de Paris,"
3S., vol. iv., p. 874, November 10, 1849.
1849 Coblentz 19 Wegeler. "MedicinischeZeitung,"vol.
xix., p. 69, 70, Berlin, April 3, 1850.
1852 Freienfels (Ober- 8 Hiibner's Cases. See "Aerztliches
franken) Intelligenz-Blatt," vol. i., pp. 166-
168, Munich, May 27, 1854 ; also "Gazette Hebdomadaire de Mede-cine et de
Chirurgie," 1 S., vol. ii., pp. 176-178, Paris, March 9, 1855.
1852 Paris 4 Auzias-Turenne. See "Bulletin de
1'Academie Imperiale de Medecine," iS., vol. xxx., p. 467, 1864-65.
1855 Lyons 1 Rodet. See " Bulletin de
1'Aca-
demie Imperiale de Medecine," 1S.,
i vol. xxx., pp. 466, 467, 1864-65.
'855-71 Czomad (near 34 Glatter. See Bonn's " Handbuch der
I Pesth) Vaccination," p. 322, Leipzig, 1875.
1856 Lupara 34 Marone. See "Lancet," May 31,
1862, vol. i., pp. 567, 568; also Lancereaux on " Syphilis," p. 641.
1858 Cherbourg__ 2 Lecoq. " Gazette des Hopitaux," vol.
______________________ xi., p. 598, Paris, December 24,1859.
ALLEGED CASES OF VACCINO-SYPHILIS. 297
Y»mr. Place.
No. Authority and Reference.
lK(to Rufina (near 14 Galligo. "Gazette
Hebdomadairede
Florence) Medecine et de Chirurgie,"
1S., vol.
vii., pp. 519, 520, August 10, i860.
1 NO 1 Rivalta 46 Coggiola. See
Cerise in " L'Union
Medicale," 2S., vol. xii., pp. 259-264, Paris, November 9, 1861 ; also " Gazette
Hebdomadaire de Medecine etde Chirurgie," 1S., vol. viii., PP- 779-782,
December 6, 1861 ; and "Lancet," November 16, 1861, vol. ii., pp. 485, 486.
1861-2 Paris 1
Trousseau. See Depaul, "Bulletin
de l'Academie Imperiale de Medecine," iS., vol. xxx., pp. 144-145, 1864-65.
1862 Torre de' Busi 5 Adelasio. " Gazzetta
Medica Italiana
Lombardia," 5 S., vol. iv., pp. 158-
161, Milan, May 1, 1865.
1S63 Paris I
Chassaignac. " Bulletin de la Societe
de Chirurgie de Paris," 2S., vol.
iv., p. 361. 1864. For drawing
of case by R. Druitt, see Trans.
Obstet. Soc. Lond. for 1863, vol.
v., p. 196, 197.
1S63 Paris 1 Devergie. " Bulletin de
l'Academie
Imperiale de Medecine," 1 S., vol.
xxviii., pp. 664-669, 1862-63.
1863 Paris I Herard. Ibid., pp. 1189, 1190.
1863 Beziers 1 Sebastian. " Gazette des
Hopitaux,"
vol. xvi., p. 493, October 22, 1864;
also " Gazette Hebdomadaire de
Medecine et de Chirurgie," 2S.,
vol. ii., p. 41, January 20, 1865.
1863 Bergamo 2 Adelasio. " Gazette des H6pitaux,"
vol. xvi., p. 494, October 22, 1864.
France 2 or 3 Auzias-Turenne. Bulletin de l'Aca-
demie Imperiale de Medecine, iS., vol. xxx., pp. 322, 323, 1864-65.
Paris I 1 Laroyenne. Ibid., pp. 470, 471.
[865 Paris 12 or Depaul. Ibid., vol. xxxii., pp.
1048-
more 1056, 1866-67. 1866 Argenta (Fer- 27
Gamberini. " Gazette des Hopitaux,"
rara) vol. xxi., p. 505, November, 1869.
1866 Rosheim 10 Schuh. See Depaul in " Bulletin de
l'Academie Imperialede Medecine,"
iS., vol. xxxii., pp. 1058-1061,
_______________________ 1866-67.___________________
Year. Place.
No. Authority and Reference.
1866 Auray (Morbi- 50 or Depaul.
Ibid., pp. 201-224 and
j han)
more
1033-1038.
1866 j Florida | 52
Fu(}ua. See Joseph Jones' " Medi-
| cal and Surgical Memoirs," p. 472,
I New Orleans,
1890.
1866 Cardeillac (Lot) j 13 Depaul.
See "Bulletin de l'Aca-
| demielmp^rialede Medecine," IS.,
I vol. xxxii., pp. 1039-1043, 1866-67.
1869 Prussia 1 1
Verfasser. See Kobner in "Archiv
I fiir Dermatologie und Syphilis,"
I vol. iii., p. 159, Prague, 1871.
1869 Paris 1
Guerin. "Bulletin de l'Academie
{
Imperiale de Medecine," j S., vol.
i xxxiv, p.
512, 1869.
Syra (Greece) 2 Zallonis. See
Depaul, Ibid., pp.
1017, 1018.
Villemarechal 1 Vicherat.
Ibid., pp. 1103-1106.
1869 Schleinitz and St. 35 Kocevar.
"Allgemeine Wiener Medi-
Veit (Styria) zinische Zeitung," vol.
xv., pp.
266-268, May 24, 1870.
1869
2 Kobner. "Archiv fiir Dermatologie
and und Syphilis,"
vol. iii. p. 133,
1870 1871.
1875 I New York 1 Taylor. "Archives of
Dermatology,"
vol. ii., pp. 203-209, New York, April, 1876.
1876 i Lebus (Prussia) 15 Appendix to Report of German Vac-
I cination Commission, 1884. See
Q. 9,961, Third Report, Royal
I Commission on Vaccination.
1880 Algiers 58 Journal D'Hygiene, vol.
vi., pp. 399,
400, Paris, August 25, 1881.
; France 1 More. "Bulletin de
l'Academie de
Medecine," 2 S., vol. xiii., p. 1240, 1884.
1885 I Turin 35 Layet. Traite
pratique de la Vac-
| cination Animale, p. 74, Paris, 1889.
1889 J Marseilles j 1 Perrin. " Annales de
Dermatologie
'. et de
Syphiligraphie," 3S., vol. i.,
pp. 654-657, Paris, 1890.
1889 j Oise 5 Hervieux. "
Bulletin de I'Academie
de Medecine," 3S., vol. xxii., pp. 116-125. 1889.
1889 j Motte-aux-Bois ' 43 Hervieux. Ibid., pp. 230, 496, 517.
1891 I Germany ! 1 Rosenthal. "Deutsche
Medicinische
Wochenschrift," vol. 18, p. 121,
Leipzig and Berlin, February 11,
_________________________________ 1892._____________________________
DR. JAMES WHITEHEAD'S CASES. 299
Tims we have a total of over 700, without including Knglish cases to be
mentioned hereafter.
The cases which first attracted serious attention to 1 lie subject in this
country are those of Dr. James Whitchead.1 He made a systematic examination of
children brought to the Hospital, and 1,435 out of 1,717 were found to have been
vaccinated. In a considerable number of instances the mothers blamed vaccination
as the cause of the disease from which the children suffered, and in thirty-four
cases Dr. Whitehead thought that the evidence appeared to be sufficiently
convincing to warrant the belief that a taint had been communicated ; in
fourteen he considered the disease to be of true syphilitic character, as shown
by the symptoms and by the mode of its derivation ; and in the remaining twenty,
although the history was less clear, the symptoms so precisely resembled
constitutional syphilis that the treatment employed was that commonly used in
syphilitic disease, and was in most cases attended with satisfactory results. In
the four following cases, described by Dr. Whitehead, the local vaccine vesicles
developed into sores, and thus, in these instances at any rate, there can be but
very little doubt that the syphilitic symptoms were actually produced by
vaccination.
Case 2.—An infant, aged nine months, of a bad habit of body. Copper-coloured
blotches appeared after vaccination. When seen, there was a mixed eruption on
the face and scalp and extreme irritability of the
1 Third Report of the Clinical Hospital, Manchester. James Whitehead, M.I).
London. 1859.
whole surface ; the vaccinated spots remained unhealed at the end of five
months, presenting a well-formed rupia with excavation. The father and mother
are described as apparently healthy.
Case ii.—An infant, aged eleven weeks, of medium habit of body. When seen, there
were two deep ulcers with hardened bases where the vaccine vesicles were formed
three weeks previously ; copper-coloured roseola on the nates and chin, sallow
complexion, mucous tubercles round the anus, eruptions and intertrigo behind the
ears, coryza, atrophy, and dysentery. The history of the case is that roseola
appeared from twelve to fourteen days after the vaccination, at the age of two
months; the mucous tubercles nine weeks after, while under treatment, and
atrophy four months after. Father said to be healthy; mother feeble, but
apparently free from taint.
Case 36.—An infant, aged seven and a half months, of good habit of body. After
the subsidence of the vaccination, the vesicles degenerated into ulcers,
surrounded by erythema. When seen, there were erythematous blotches of a copper
colour on the chest and neck, eczema auris, arthritis of the left elbow joint,
and syphilitic pallor. Father said to be healthy; mother apparently healthy.
Case 57.—A child, aged three years and three months, of good habit of body. She
was healthy up to the time of vaccination, three months previously. The three
vaccinated spots degenerated into three deep ulcerations with hardened bases,
which remained open for two months. When seen, there were all over the trunk and
limbs flat herpetic-like crusts, with large erythematous
MR. HUTCHINSON'S CASES. 301
areolse of copper tint, most numerous on the thighs; the cicatrices of the
first-formed patches being of a deep copper colour. The patient suffered from
great prostration, inappetence, eneuresis, and dysuria, erythema of the vulva
without discharge, chronic blepharitis, photophobia, and syphilitic pallor. The
first symptoms were ulceration of the vaccinated spots with copper-coloured
blotches. Father and mother apparently healthy.
Mr. Jonathan Hutchinson, on April 25, 1871, made his first communication to the
Royal Medical and Chirurgical Society on the subject. Twelve persons (mostly
young adults) were successfully vaccinated with lymph from a healthy-looking
infant. In all except two, indurated chancres developed in the vaccination
scars.
Shortly afterwards, Mr. Waren Tay, one of Mr. Hutchinson's colleagues, came
across another series of cases. Two children of the same family, aged four years
and sixteen months respectively, had been vaccinated seven weeks before they
came to be treated for skin eruption ; the vaccination spots were unhealed and
indurated at the base. By means of the vaccination register, twenty-four others
vaccinated with the same lymph were traced. It was found that nine children,
counting the two previously mentioned, had unquestionable symptoms of
constitutional syphilis, and there were suspicious symptoms in six others, a
certain number entirely escaping. It is important to note that nothing had
occurred to excite the vaccinator's suspicions, none of the children having
been taken back to him on account of the unhealthy condition of the arm. Two of
the patients, however, had been under medical
care, but in not a single instance had the real nature of the disease been
suspected.
Mr. Hutchinson's third series consisted of one case only. The patient, aged
forty-six, came under his care at the Moorfields Eye Hospital for acute iritis.
He had been vaccinated three months previously, and the vaccination spots were
the seat of chancrous induration. Mr. Hutchinson called on the vaccinator, who
said he had never seen such sores as were displayed on this man's arm, but had
not, *however, suspected the real nature of the disease. About twelve other
persons were vaccinated at the same time, and from the same child, and with the
exception of a little trouble in the healing of the sores in one or two of the
patients, they had shown nothing peculiar.
In the fourth series, the patient was a woman aged forty-six. Neither the
patient nor the surgeon who vaccinated her had suspected she had been
syphilised. The fifth series was brought under Mr. Hutchinson's notice by Mr.
Waren Tay in April, 1876. A mother and her two children, one an infant and the
other a child of two, were found to be suffering from secondary syphilis. The
children were vaccinated in September, 1875, and their vaccination sores had
reopened and for a long time remained unhealed. The mother had contracted a
sore on her nipple from the younger child, and her symptoms were two months
behind those of the children. The husband subsequently contracted syphilis from
his wife.
Mr. Hutchinson also relates a case of vaccino-syphilis he had seen in a lady
recently arrived from India. The vaccination did not take, but a
little spot like a
MR. MAKUNAS "INQUIRY." 303
mosquito-bite resulted; this healed, and six weeks afterwards a sore formed.
When seen by Mr. Hutchin-son she had two indurated and dusky chancres on the
arm, and was covered with a syphilitic eruption.
When we consider that in a number of these cases the nature of the complaint had
been unsuspected (in some, even by the medical men) until they had come under
the care of Mr. Hutchinson or Mr. Waren Tay, it seems more than probable that a
large number of cases of vaccino-syphilis remain unrecognised as such, and never
come to light at all.
In 1883 questions were addressed to medical men on the subject of vaccination.
Among others, it was asked, " What diseases have you, in your experience, known
to be conveyed or occasioned or intensified by vaccination ? " Three hundred and
eighty-four replies were received, and they are published in Mr. M. D. Makuna's
"Transactions of the Vaccination Inquiry." The following testimonies have been
extracted relative to the occurrence of syphilis after vaccination :—
5. " Syphilis once only." 18. "I have only seen one case of syphilis which I
attributed
to vaccination from a syphilitic infant." 25. "A certain amount of syphilis, in
rare instances." 40. '' I have known syphilis in aggravated forms .... to follow
very speedily the operation."
51. "I only remember one case in my practice in whom syphilis
was intensified."
52. " I have seen one case of syphilis apparently conveyed."
64. " I have known syphilis .... occasioned by it."
93. "I have seen syphilis more than once."
96. " Syphilis once with an incrustated rash."
112. "Syphilis."
114. "Syphilis .... having previously been dormant."
120. "I remember one case of syphilis" (intensified by vaccination).
130. "Syphilis."
139 and 140. "Syphilis in two cases."
162. " Occasionally in rare instances it has appeared to convey
syphilitic .... disease..................... I cannot recall any
such cases in my experience as absolutely proved, although I have had my
suspicions aroused."
164. " I cannot quite assent that I have seen syphilis conveyed by vaccination,
but I firmly believe I have seen three or four such cases."
175. "One case of death from syphilis in a boy about two years old, who was
found afterwards to have been vaccinated from a child born with symptoms of
syphilis."
190. Had seen syphilis in other medical men's practice.
192. Had seen syphilis "perhaps once."
211. "Syphilis and death occasioned."
231. " Three cases of syphilis." (Notes of cases lost.)
238. " I have also on two occasions seen among children in London what I thought
to be syphilitic eczema, which yielded to mercury."
262. " I have seen syphilis .... produced by vaccination."
271. "Syphilis conveyed twice, once by primary, and once by re-vaccination."
274. " Syphilis " (conveyed).
277. " Only one case in which syphilis was suspected."
281. "Very rarely syphilis conveyed by impure vaccination."
282. " I have seen one child die of syphilis, I believe from
vaccination."
288. "When a student I have seen syphilis conveyed, but have
not details of cases."
291. Two cases, one of which doubtful. (Notes of cases given.) 299. " One
case at St. George's Hospital, when I was a pupil
twenty years ago, in a young woman, of syphilis." 318. " Secondary or probably
tertiary syphilitic symptoms." 326. " I have known two cases where there were
good grounds
for supposing syphilis was conveyed by vaccination." 331. "Syphilis once." 340.
" I remember a case of syphilitic sores on the arms of a boy
from vaccination, five years ago." 353. " One case of syphilis."
383. " I have known lymph taken from a syphilitic or scrofulous
child communicating analogous disease to the children vaccinated with it."
384. " One case of syphilis."
Quite recently, and before the Royal Commission ("Sixth Report, pp. 218, 219),
Mr. E. Ward mentioned three cases which had come to his knowledge, two in the
practice of Mr. Holmes, of Leeds, in 1871, and the third a very sad case in a
young woman of twenty-two. She was vaccinated in 1888, and about four or five
weeks afterwards the points of vaccination became indurated. This was followed
by the usual phenomena of syphilis, and the case terminated two years
afterwards by death with cerebral symptoms.
For further British cases, see the following:—
Alleged Cases of Vaccino-Syfihilis.
t
Year. Place.
No. Authority and Reference.
1839 1 Whitehead.
" On the Transmission
from Parent to Offspring of some Forms of Disease and of Morbid Taints and
Tendencies," pp. 174-176. 1851.
1843 I Bodmin 2 Haydon. Medical Times
and Gazette,
March 29, 1862, vol. i., p. 316.
1863 Glasgow 1 Buchanan. Glasgow
Medical Journal,
April, 1865, vol. xiii., pp. 60-65.
London 3 Nayler. '' A Practical and
Theoreti-
cal Treatise on the Diseases of the Skin," p. 279-281. London, 1866.
1866 London 1 Drysdale.1 British
Medical Journal,
April 25, 1868, vol. i., p. 396.
1866 London 1 Pollock. Lancet,
April 21, 1866,
vol. i., p. 424.
1870 I London 1 Smith. Transactions
of the Clinical
Society, vol. iv., pp. 53-59. 1871.
1872 Belfast 1 Scott. Medical
Press and Circular,
January 29, 1873, vol. i., pp. 84,
: 85-
1873 ; London 1 Hulke. Medical Times
and Gazette,
\ February 8, 1873, vol. i., p.
153.
1883 i London 1 Collins.1
Transactions of the Vac-
cination Inquiry, p. 63. 1883.
For some time after the publication of Mr. Hutchin-son's cases, although the
communicability of syphilis by vaccination was admitted, it was stated that this
could only take place if the blood of the vaccinifer was taken with the lymph.
In this connection it may be mentioned that a committee consisting of Dr.
Bristowe, Professor Humphry, Mr. Hutchinson, and Dr. Ballard, in reporting
1 These cases are also alluded to in the list on pp. 303-305, and are numbered
18 and 291 respectively.
ALL LYMPH CONTAINS BLOOD CELLS. 307
on a well-known case,1 said—"It is conclusively proved that it is possible for
syphilis to be communicated in vaccination from a vaccine vesicle on a
syphilitic person,, notwithstanding that the operation be performed with, the
utmost care to avoid the admixture with blood."
All lymph, however, contains blood cells, and this apparently was known as long
ago as 1862. Dr. Heron Watson writes—" There is no vaccine matter, however
carefully removed from the vesicle, which, on microscopic investigation, will
not be found to contain blood corpuscles."2 This has been corroborated by Drs.
Barthelemy3 and Husband,* the latter's statement before the Royal Commission
being accepted as final. Thus the Commissioners say (section 430)—"The evidence
given by Dr. Husband, of the Vaccine Institution of Edinburgh, established the
fact that all lymph, however pellucid, really docs contain blood cells."
There is nothing necessarily in the appearance of the vaccine vesicle to lead
one to suspect syphilis; and Dr. Ballard informs us that " The perfect character
of the: vesicle is no guarantee that it will not furnish both vaccine and
syphilitic virus:"5
Again, a vaccinifer may exhibit no signs of the disease.
1 See Supplement, containing the Report of the Medical Officer, to the Twelfth
Annual Report of the Local Government Board, pp. 46-51,. 1882-83, and for
subsequent history of case Allbutt's "System of Medicine," vol. ii., p. 608.
London. 1897.
''■Edinburgh Medical Journal, vol. vii., p. 859, foot-note. March, 1862.
3See "Leconssur la Syphilis Vaccinale," pp. n 2-114, foot-note. Alfred
Fournier. Paris. 1889.
4 Sixth Report, Royal Commission on Vaccination. Q. 27,327-9.
5 " On Vaccination : Its Value and Alleged Dangers." A Prize Essay.
P. 345. London. 1S68.
Mr. Hutchinson, referring to a discussion on the subject, before the British
Medical Association at Birmingham, in which he had taken part, observes—" In
reference to the possibility of conveying syphilis from a vaccinifer who did not
reveal the taint by any visible symptoms or any degree of cachexia, I felt bound
in honesty to say-that I felt sure of it. No surgeon in his senses would ever
vaccinate from a child which showed obvious symptoms. The fact is, however, that
a certain number of syphilitic infants look perfectly healthy whilst yet very
efficiently contagious. There is no use, and much danger, in denying this
important clinical fact." l
He then mentions that the child from which the lymph was taken to vaccinate his
first series of cases, only revealed a little sore; this was seen by several
medical men, including Sir John Simon, who questioned whether it could be
considered proof of taint. In the second series, the vaccinifer did not present
a single visible symptom, and Mr. Hutchinson concludes that " It is absurd to
assert that inherited syphilis is always to be detected, and it is a cruel
injustice to imply that all accidents have been the result of carelessness,"
indeed in a large number of cases, the vaccinifer has presented no trace of
syphilitic disease. This brings us face to face with the terrible thought that
there may be some relationship between the two diseases—cow-pox and syphilis.
In the first chapter of this volume, I have alluded to the misleading name of
variola vaccines or small-pox of the cow, given to the disease by Jenner. It
is this misleading
1 Archives of Surgery, October, 1890, vol. ii., p. 104. Jonathan Hutchinson,
LL.D., F.R.S.
TRAMMELS OF JENNERIAN PATHOLOGY. 309
name that has been, and is, even at the present time, largely responsible for
the misunderstanding of the cardinal symptoms of cow-pox, and this has been
pointed out by none more forcibly than by the great Dr. Gregory:— "The more I
reflect on the phenomena of small-pox after vaccination, the more convinced I am
that, so long as the notion of the identity of cow-pox and small-pox thus
obstinately prevails in our minds, so long will all just views of vaccine
pathology be embarrassed." *
In a letter to Stewart, of Kelso, Dr. Gregory writes— " I have never yet
addressed anyone in writing on the subject, and I now write to you upon it,
because I see that you have considered it well—that you have thrown off the
trammels of Jennerian pathology, and think for yourself. Observe, I say,
fennerian pathology, not Jennerian practice. I feel assured you do not view
vaccination as a kind of small-pox. The term variolce vaccince was incorrect in
pathology. Cow - pock is a something that alters the human blood, and indisposes
it to take small-pox. But it is not small-pox. A coating of gold secures our
salt spoons from the action of chlorine; but gold is not chlorine. Small-pox,
after vaccination, is not on a par with double small-pox."2 The disease that
cow-pox most resembles is not small-pox, but syphilis. This view of the analogy
of cow-pox with syphilis was held by Auzias-Turenne, and in this country it has
been advocated by Dr. Creighton. Auzias-Turenne says—" Between syphilis
1 London Medical Gazette, vol. xxix., p. 193 (October 29, 1841).
a'' An Investigation of the Present Unsatisfactory and Defective State of
Vaccination," pp. 106, 107. Thomas Brown, formerly Medical Practitioner in
Musselburgh. Edinburgh. 1842.
and cow-pox the analogy may be a long way followed up. The inoculation of
cow-pox—a malady with a fixed virus sufficiently well-named pox of the cow
(verole de vache)—may, for example, give rise to polymorphic vaccinides, and
sometimes to disseminated pathognomonic vesico-pustules, just as the contagion
of the mucous patch, symptom of a malady with an equally fixed virus, gives rise
to various secondary eruptions, and sometimes to the appearance of disseminated
mucous patches. But, happily for the vaccinated, cow-pox passes through a rapid
evolution, and does not leave virulent remains for so long a time or so
frequently as syphilis."1
The difficulty of distinguishing some cases of cow-pox from syphilis has been
recognised by the best authorities. Mr. George Berry, ophthalmic surgeon to the
Royal Infirmary, Edinburgh, in a communication on cow-pox of the eye-lids, says
that the main interest in these cases "consists in the possibility of the
inoculation taking place at all, and in the differential diagnosis between
vaccinia and a primary syphilitic sore." 2
Dr. Seaton has also alluded to this difficulty: "Among the sources of fallacy
against which we have to be on our guard in cases in which syphilis has been
said to have been produced by vaccination, one is an erroneous diagnosis.
Persons talk very glibly about sores being syphilitic, and eruptions being
syphilitic, as though the characters of syphilitic sores and syphilitic
eruptions were so made out that there could never be any mistake
1 " History and Pathology of Vaccination," vol. ii., p. 552. Edgar SI.
■Crookshank, M.B. London. 1889.
^British Medical Journal, June 28, 1890, vol. i., pp. 1483, 1484.
SYMPTOMS OF NATURAL COW-POX. 311
about them. Yet such mistakes are daily being made by practitioners in general,
and are occasionally made by the very highest authorities. About four years ago
one of those amongst us most conversant with syphilis, Mr. I Icnry Lee,
announced to the Medico-Chirurgical Society that he had a case under his care in
which a syphilitic chancre had been produced on the arm of a child by
vaccination. The case was seen by many members of the profession, some of whom
agreed with Mr. Lee, while others saw nothing but a sore arm, the result of a
degenerated vaccine vesicle. The subsequent progress of the case quite satisfied
Mr. Lee that he had been mistaken in his diagnosis, as he publicly
acknowledged."x
The accounts of cow-pox in milkers and in the early removes from the cow
describe it as consisting of corroding, hard, and painful sores with small
disposition to heal, accompanied by enlargement of the neighbouring, lymphatic
glands. There appeared also considerable constitutional disturbance and
secondary eruptions. A contagious disease presenting these characteristics
cannot be very far removed from syphilis, and there seems nothing improbable in
the suggestion that cases of so-called vaccinal syphilis are merely the
reversion of cow-pox to a former type. What is known as the Leeds case is an
instance in point.
Emily Maud Child was vaccinated on March 26, 1889, and died at the Leeds
Infirmary on July 1 of the same year. At the inquest on July 10, four members of
the infirmary staff—Messrs. M'Gill, Ward, Littlevvood, and
1 " Handbook of Vaccination," p. 322. Edward C. Seaton, M.U. London. 1868.
Dr. Barrs—gave evidence that the child died from vac-cino-syphilis, and the
verdict of the jury was that she " died from syphilis acquired at or from
vaccination." The case was shortly afterwards made the subject of inquiry by Dr.
Ballard, one of the medical inspectors of the Local Government Board, and his
conclusions were as stated in Parliament by the President of the Local
Government Board, Mr. Ritchie, who used the following words:—" An inquiry has
been made by an Inspector of the Board with regard to the case. His conclusions
are not the same as those arrived at at the inquest. He states that the child in
question was the only sufferer from subsequent syphilis among all the children
he reached and whom he saw that had been vaccinated with the same or any other
lymph in the whole course of the vaccinator's March vaccinations; and further,
that the entire family to which the alleged vaccinifer belonged were, as far as
he could discover by examination of them, free from any syphilitic taint or
suspicion of such taint. The Report of the Inspector will be at the disposal of
the Royal Commission on Vaccination."1
This implies that the child died from hereditary syphilis, and I would direct my
readers' attention to the following from Mr. E. Ward's evidence before the Royal
Commission :—
Q. 23,688. (Dr. Collins). Did you examine the two elder children, the brother
and sister of Emily Maud C. ?—Yes, on several occasions.
1 Hansard's Parliamentary Debates. Third series, vol. cccxli., pp. 1330,
1331. February 27, 1890.
THE LEEDS CASE. 313
• >. 23,689. Did you find them "stunted in growth"?— No, they struck me, the
girl particularly, as being remarkably fine children.
< >. 23,690. Did you find the central upper permanent incisors of Eva, the
eldest child, notched in the characteristic syphilitic manner?— I do not think
it was at all characteristic of syphilis; and I do not think Mr. * Hutchinson
thinks so.
(J. 23,691. (Chairman). Do you know what was referred to as the
"notching"?—Yes, perfectly.
Q. 23,692. (Dr. Collins). Did you get any history of " prolonged snuffles " in
the second child, the boy ?—No, that is nothing; when I saw the boy he was a
little stuffy in the nostrils, but so many children are that— nothing that I
should attach any importance to—it was long after any snuffles found in the
ordinary course even of congenital syphilis would have disappeared.
Q. 23,701. Would it be true to say that the family was in any sense a "
syphilitic family " ?— I should say certainly not.
The words within quotation marks were presumably quoted by the Chairman and by
Dr. Collins from Dr. Jiallard's report to the Local Government Board, and hence
there can be no possible doubt of the nature of this report.
The matter would probably have been left at this stage were it not that a Royal
Commission was then
sitting. An independent enquiry was, therefore, made by Dr. Barlow on behalf of
this body, and he reported that there was no evidence of syphilis in either
parent of the child, no evidence of inherited or acquired syphilis in either of
the two elder children, nor did the history of the third (deceased) child
suggest to him that it was the subject of inherited syphilis. Mr. Hutchinson has
also testified to the fact that there is no evidence of syphilis in any of the
family. It may be mentioned that Dr. Ballard's report containing this accusation
was refused to the parents,1 but handed over to the Royal Commission, who, for
some reason or other, have omitted to publish it in their reports. The
conclusion of the Commissioners on the case is that it " may probably be classed
with a few others as examples of gangrene and blood poisoning, the direct result
of vaccination, which are not to be explained by supposing the introduction of
any syphilitic or other poison." (Section 427.) Considering that the case was
taken for syphilis by the four members of the infirmary staff, and also by Dr.
Ballard, it appears that symptoms presenting all the characteristic phenomena
of syphilis can be produced by the vaccine disease itself.
Mr. Hutchinson, in alluding to this and other similar cases, says, " Lastly, the
question has to be entertained whether the cases are examples of syphilis in any
form. To many I am aware it will seem undue scepticism to doubt this. When
such symptoms as snuffles, thrush,
1 Hansard's Parliamentary Debates. Third series, vol. cccliii., p. 881. May 22,
1891.
RELATIONSHIP OF COW-POX TO SYPHILIS. 315
the eruption on the genitals in infancy are mentioned, not a few will hold that
the suspicion is rendered very strong, if not actually proven. In the same way,
nodes on the head, bubo in the armpit, phageda^nic sores, abscesses and
eruptions on the genitals occurring in connection with a vaccination sore which
has gone wrong, will be held by many as conclusive proofs that% syphilis has
been introduced. I cannot but freely admit that they bring with them much
suspicion, and that this suspicion is strengthened by the fact that well -
experienced surgeons, who saw these various symptoms and examined them
carefully, thought that they could be none other than syphilis. Further, there
is the fact that two of the infants were thought to have been much benefited by
mercurial treatment."1 Mr. Hutchinson also observed that if syphilis were
conclusively proved in any one he would admit it in the others.
On the next page is a list of cases presenting features similar to the Leeds
case; in some the symptoms were not so well marked as in others, but the cases
may all be said to come under the same category.
1 Archives of Surgery, vol. i., pp. 114, 115. October, 1889.
Authority. Number.
Reference. !
Taylor and Fyson I Sixth Report, R.C.V., pp. 196- |
198.
Lucas 1 Guy's Hospital
Reports, 3 S., j
vol. xxvii., pp. 31-37. 1884.
Hutchinson 1 Illustrations of Clinical
Surgery,
vol. i., p. 141. plate xxv. fig. 3. London, 1878.
Hutchinson (Dr. K.'s case) 1 Archives of Surgery, vol. i., pp.
98-104, October, 18S9. |
Hutchinson (Dr. W.'s case) 1 Ibid., pp. 193, 194, Jan., 1890.
Hutchinson (Dr. H.'s cases) Several Ibid., pp. 194, 195.
Hutchinson 1 Ibid., pp. 197, 198.
Hutchinson 1 Ibid.,vol. ii.,pp. 23,24.
July,1890.
Hutchinson I Ibid., pp. 213-215, Jan.,
1891.
Parsons Several British Medical Journal,
Nov-
ember 29, 1890, vol. ii., p.
j 1233-
Local Government Board, 5 Appendix ix. to Final Report,
Nos. xix., xlii., lix., R.C.V.
lx., xciv. Royal Commission on Vac- 23 or Appendix ix. to Final
Report,
cination, Nos. 11, 21, more R.C.V.
35.39.113.139.Hi.162,
167, 169, 175, 177, 183,
199, 202, 204, 206, 207 ,
208, 241, 258, 326, 416.
It might have been anticipated that some further light would have been thrown on
cases of this description by Dr. Acland in his article in Allbutt's " System of
Medicine," but he contents himself by quoting the opinion of the Royal
Commission that the relationship of cow-pox to syphilis "is a point of
speculative, almost it might be said of transcendental pathology," and, although
he admits that Nos. 109, 113, 207, and 416, in Appendix ix. to the Final Report
of the Royal Commission, are similar to the Leeds case and others described by
Mr. Hutchinson, he apparently has nothing
CALF LYMPH AND VACCINO-SYPHILIS. 317
further to add, for he remarks that " it would not be possible here to enter
into these cases in detail." 1
If it be a fact, as maintained by Dr. Creighton, that the phenomena of
vaccino-syphilis so-called, are due to the inherent, though mostly dormant
natural history characters of cow-pox itself, we should expect the same
appearances to take place occasionally in cases of calf lymph; and in this
connection the experience recorded by Mr. Hutchinson in the Archives for
January, 1891 (pp. 213-215), is of interest. He particularises a case of
vaccination with calf lymph presenting certain symptoms simulating syphilis.
The child was born of healthy parents in July, 1890; was perfectly healthy at
birth; was vaccinated at three months of age with Renner's calf lymph, at the
same time as several others who did well; on the eighth day, only one place
seemed to have taken, but later on all three looked satisfactory; at the end of
three weeks, the arm was inflamed, and there were large black scabs with pus at
their edges; a week later a large slough comprised all the vaccination sores and
passed deeply almost to the bone, and there was also a pustule on the nose, and
three nodes on the skull.
Mr. Hutchinson compares this case with another he had described in an earlier
number of the Archives (October, 1889, p. 110). These two cases resembled one
another, in that in both the infant was perfectly healthy up to the time of
vaccination; the lymph used was not taken from the human subject, the skin
around the vaccination sores passed into gangrene, with at the time
1 Allbutt's " System of Medicine," vol. ii., p. 604. London. 1S97.
a large glandular swelling in the arm-pit. There were also periosteal swellings
of considerable size on the skull bones, suspicious sores on the skin; and both
patients appeared to be much benefited by mercurial treatment
Mr. Hutchinson says—" It is obvious that these two cases give mutual support to
the belief that no accidental contamination of the calf-lymph by syphilitic
secretions occurred. This was a suggestion which, although there was not the
slightest evidence in its support, it was difficult to wholly exclude in an
isolated case. It is, however, improbable in the highest degree that such an
accident should occur in two cases, and in each should be followed by precisely
similar results.
" There remains then the question: Were these infants the subjects of a latent
inherited taint which vaccination roused into activity? In neither case was
there the slightest evidence that either parent had suffered from syphilis, and
in neither had the infant prior to vaccination shown any symptoms. In one case
the child was a first-born, but in the other there was a healthy elder child.
" The final supposition is that it is possible for vaccination independently of
any syphilis, whether implanted or hereditary, to evoke symptoms which have
hitherto been regarded as peculiar to the latter malady, and which are
apparently greatly benefited by specific treatment. On this point we must hold
our minds open to the reception of further evidence."
A case perfectly parallel with the above-mentioned and the Leeds case was that
described by Dr. Frederick Taylor and Mr. Edmund Fyson before the Royal
Commission (Sixth Report, pp. 196-198). Every possible
DISASTERS IN THE AMERICAN CIVIL WAR. 319
precaution appears to have been taken. The infant was in good health. Dr.
Renner's calf lymph had been used, and the needle with which the child was
vaccinated had never been employed before. Gangrene of the pocks ensued, and
also gangrenous spots in other parts, and (lie case terminated fatally.
When it is said that vaccino-syphilis is rare, it must be remembered that these
and other cases similar have only recently been published, and until further
information is forthcoming, it would be hazardous to assert t hat a general
introduction of calf lymph would rid us of the danger of vaccino-syphilis ;
indeed, it remains to be proved that by the repeated transmission through the
bovine species, cow-pox will not again acquire much of its old character. Before
the Royal Commission, Dr. Cory gave his experience of 32,002 vaccinations
performed at the calf lymph station ; 323 cases returned for complaint, 260 of
which had sore arms,1 and Dr. Cory gave it as his impression that you got more
sore arms after using calf lymph than from the humanised variety. This
experience has been borne out by other competent observers.
Before concluding the evidence under the heading of " Syphilis," I wish to
allude to the disastrous consequences of vaccination in the American Civil War
(1861-65), in which some hundreds of men were affected with a disease presenting
all the characters of syphilis. The facts are related by Dr. Joseph Jones, and
the conditions described were truly frightful. The sym-
1 In this class of cases there was unwillingness of the sore to heal, and some
induration. Q. 4,377 and Q. 4,380.
ptoms included phagedenic ulcers, with indurated and everted edges, secondary
skin affections, ulcerated throats, loss of hair, and other phenomena
distinctive of syphilis. In some cases the gangrenous ulcers caused extensive
destruction of tissue, exposing arteries, nerves, and bones, in many cases
necessitating amputations.
Dr. J. T. Gilmore, in a letter to Professor F. Eve, referring to three hundred
cases in the Georgia brigades, remarked—" The cases presented the appearances
that are familiar to those of us who were connected with the Confederate
army—large rupia-looking sores, sometimes only one; generally several on the arm
in which the virus was inserted. In a number of cases these sores extended, or
rather appeared on the forearm, and in two cases that I saw, they appeared on
the lower extremities. The men suffered severely from nocturnal rheumatism.
Several cases had, to all appearances, syphilitic roseola. I saw enough of the
trouble to convince me thoroughly that the virus owed its impurity to a
syphilitic contamination."1
Dr. James Bolton testified that "on careful inspection the ulcers presented the
various appearances of genuine chancre. In some instances there was the
elevated, cartilaginous, well-cut edge surrounding the indolent, greenish ulcer;
in others there was a burrowing ulcer, with ragged edge; in others there was the
terrible destructive sloughing process devastating the integuments of the
arm. Many of the cases were so situated
1 "Medical and Surgical Memoirs," vol. iii., part I, p. 466. Joseph Jones,
M.D. New Orleans.
that their history could be preserved, and in these .secondary symptoms
appeared, followed in due time by tertiary symptoms. The chancre was followed
successively by axillary bubo, sore throat, and various forms of eruption
{syphilis dermata), while the system fell into a state of cachexia."1
Dr. E. A. Flewellen testified that " while the army of General Bragg was at
Tullahoma, I was medical director, and I know that very great complaint was made
to me as to the character of the vaccination practised in the army. A large
number of men were represented as unfit for duty. I think that one division
represented nearly a thousand men as unfit for duty on account of spurious
vaccination. I saw a number of cases in the early progress of the vaccination,
but they presented nothing abnormal that I could detect. But, as it advanced,
the cases seemed to have the appearance very nearly of syphilitic rupia. It
diffused itself more or less over the whole surface. A large number of surgeons
regarded it as a complication of vaccinia and syphilis. Finally, they settled
into the opinion that it was not syphilitic. There never was, I may say, any
settled opinion among the surgeons of the Confederate army as to what was the
true character of this impure virus."2
Dr. George H. Hubbard relates that on November 30, 1863, he arrived at Fort
Smith, Arkansas, having been appointed Medical Director of the Army of the Fron-
1 " Medical and Surgical Memoirs," vol. iii., part 1, p. 467. Joseph Jones,
M.D. New Orleans. 2Ibid., p. 480.
tier. His attention was immediately directed to several hundred men disabled
in consequence of "spurious vaccination." A Medical Board was appointed to
investigate these cases, and they reported : " At the time we examined the
patients, some had well-marked Hunterian chancre ; some had large excavated
ulcers, with edges everted above the raw and surrounding induration ; the
centres, when not recently cauterised, were of a brownish hue—some, whose
primary ulcers were about healed, had secondary symptoms, such as swelling and
ulcerations of the glands in different parts of the body ; while others had pain
and stiffening of the joints. The disease was brought to the First Arkansas
Infantry by deserters from the Confederate Army, and in our opinion is
syphilis." 1
Dr. William F. Fuqua,2 formerly surgeon of the 7th Florida Regiment, reported
fifty-two cases in Confederate soldiers who presented abscesses in the axillary
glands, pains in the limbs and joints, ulceration of the throat, buboes,
coppery-coloured eruptions, loss of hair, and these symptoms were only relieved
by anti-syphilitic treatment. The cases were attributed to inoculation with
virus from the arm of a sailor who was labouring under syphilis.
Although the annals of vaccination disasters do not furnish any other records of
vaccino-syphilis on so vast a scale as that which occurred in the American
Civil War, other disasters have been recorded of
1" Medical and Surgical Memoirs,''vol. iii., part 1, p. 483. Joseph Jones,
M. D. New Orleans. 2Ibid., p. 471.
"SPURIOUS VACCINATION" AT GRANITEVILLE. 323
sufficient importance to demand special reference. Among these may be mentioned
the cases of "spurious vaccination" at Graniteville, related by Dr. W. F.
Percival, and included in Dr. Jones' work. Dr. Percival says—"About the last of
April, 1866, I was requested to take charge of some cases of spurious
vaccination at the manufacturing village of Graniteville. One hundred and fifty
cases were presented for examination, men, women, and children of all ages,
from fifty years to twelve months. The larger proportion were operatives in the
factory, the others engaged in outdoor work. There was every variety of
constitution, from the pale attenuated girl, to the hardy and robust labourer.
Of the hundred and fifty cases, ninety-three had been previously vaccinated. The
appearance of the sore was identical in every case, viz., an excavated ulcer, of
circular form, with raised and hardened edges and base. They varied in size,
from one half to two inches in diameter, covered with grey or dark sloughy
matter, and secreting unhealthy pus. There was no appearance of granulation. In
some cases ulcers of a similar character appeared on the arms affected ; in
others on the opposite arm, and in a few on the lower limbs. In some, abscesses
formed on the inside of the arm, and in nearly all the axillary glands were
inflamed, and many suppurated. A thick and unhealthy crust would form, to be
soon separated by the pus which accumulated beneath. In one case, there was a
copper-coloured eruption on the body and limbs; in two or three the hair dropped
off. None of these cases were in the primary stage. The disease had existed from
three to eight weeks. Most of them
pursued their ordinary avocations, -as far as possible, and complained of no
constitutional symptoms, or any loss of appetite. The history of these cases, as
given to me by the individuals first vaccinated, was that they had obtained the
virus from a man whom they afterwards discovered to have had primary syphilis.
One was vaccinated from the other, and so it spread. None of the ulcers had
evinced any tendency to heal."1 Dr. Percival adds that the usual treatment for
venereal ulcers effected a cure in from three to six weeks.
I may also allude to the disasters resulting from vaccination at Algiers in
1880.
On December 30 fifty-eight recruits of the 4th Regiment of Zouaves were
vaccinated from a child which looked perfectly healthy. They were all infected
with syphilis, and about half are reported to have died, the remainder being
dismissed the service. No blame was attached to the operating surgeon.2 Another
series which created a painful impression on the public at the time was that of
fifteen young school-girls who were syphilised by vaccination at Lebus (Prussia)
in 1876.
Leprosy.
There is considerable evidence that leprosy has been invaccinated, and the
question has been raised as to
1 " Medical and Surgical Memoirs," vol. iii., part 1, p. 47S. Joseph
Jones, M.D. New Orleans.
2 Third Report, Royal Commission on Vaccination. Q. 9540, 9736.
DR. HAWTREY BENSON'S CASE. 325.
whether some part at least of the recent spread of the disease in certain
countries is not due to the practice of arm-to-arm vaccination. This has been so
fully discussed in a volume entitled " The Recrudescence of Leprosy"J that it
might be thought unnecessary to re-open the subject, especially as the facts
which it is proposed to lay before the reader must be largely a repetition of
what has been so exhaustively treated in my father's work. The matter, however,
is admittedly of such serious and far-reaching importance that no account of the
century's experience of vaccination would be complete which did not deal with
the main points of this question.
It is not proposed to discuss the etiology of leprosy, except in so far as to
show that it is a communicable disease, and may be communicated by inoculation
or by vaccination.
There are instances on record of Europeans contracting the disease in leprous
countries, as, for instance, the case of Father Damien in Molokai, Father
Boglioli in New Orleans, a French Sister of Mercy in French Guiana, and another
in Tahiti; but perhaps the most important case is that related by Dr. Hawtrey
Benson.2
An Irish soldier returned home from India, where he had resided for twenty-two
years ; a few months afterwards symptoms of leprosy developed. The patient was
under Dr. Benson's care at the City of Dublin Hospital, but ultimately went
home, where he died of
1 "The Recrudescence of Leprosy, and its Causation." William Tebb.
London. 1893.
2 Dublin Journal of Medical Science., vol. lxiii., pp. 562, 563 (June,
1877).
the disease. During this last period of his life his brother slept in the same
bed, and wore the leper's clothes. The brother had never been out of Ireland
except once, forty-six years previously, when he spent some time in England. He
developed leprosy, and Dr. Benson exhibited the case before the Medical Society
of the College of Physicians, Ireland, when the diagnosis was confirmed by those
acquainted with the malady. In making his concluding observations before the
Society, Dr. Benson pointed out that one fragment of positive evidence on the
subject was worth a vast amount of negative evidence.
This case must be regarded as affording absolute proof of the communicability of
leprosy from person to person.1
An experiment made on the condemned criminal, Keanu, by Dr. Edward Arning,2 is
interesting from the
1 For further testimonies see
Bakewell. Q. 3,656, Report from the Select Committee on the Vaccination Act
(1867). 1871.
Tilbury Fox. " Skin Diseases," third edition, p. 322. London. 1873.
Vandyke Carter. "On Leprosy and Elephantiasis," p. 178, foot-note. London.
1874.
Macnamara. " Leprosy a Communicable Disease." London. 1889.
Moore. Journal of the Leprosy Investigation Committee, No. I, p. 28 August,
1890.
Francis. Ibid., p. 56.
Cayley. Ibid., p. 36.
Murray. Ibid., p. 46.
Hanson. Ibid., No. 2, p. 64. February, 1891.
Report of the Cape of Good Hope Leprosy Commissioners, 1895, vol. iv., p. 101.
Report of the International Leprosy Conference, vol. ii., pp. 191, 192.
Berlin. 1897.
2 Journal of the Leprosy Investigation Committee, No. 2, pp. 132-133.
February, 1891.
THE INOCULATION OF LEPROSY. 327
point of view of the possibility of the invaccination of leprosy. The Hawaiian,
who, at the time of the operation, was carefully examined by several physicians
and pronounced to be in perfect health and remarkably strong, was inoculated
with a portion of a leprous nodule on the left forearm. A month later the man
suffered from rheumatic pains in the joints of the left arm, and a painful
swelling of the ulnar and median nerves. In the course of six months a small
leprous nodule was formed on the keloid spot where the inoculation took place,
and leprosy bacilli were detected at the seat of the keloid scar for a period of
sixteen months after the operation. Distinct symptoms of leprosy were observed
three years after the inoculation, and in another year the disease was at its
full height. It may be mentioned that the patient was isolated from the day of
the operation for three years afterwards. It has subsequently transpired that a
son, a nephew, and a cousin of Keanu's, have shown symptoms of the disease, but
Dr. Arning urges that at the time of the operation, Keanu himself was perfectly
free from leprosy, and that distinct signs appeared three years afterwards, and
at present (1891) furnishes a typical case of general leprosy.
Mr. C. N. Macnamara,1 in referring to a report on this case by Dr. N. B.
Emerson, President of the Board of Health, and Mr. J. H. Kimball, Government
physician, Honolulu, says—" This report establishes unequivocally the fact that
the inoculated man has become leprous ;
1 " Leprosy a Communicable Disease," second edition, p. 45. C. N
Macnamara. 1889.
and as he had been inoculated three years previously, there is every reason to
believe that the disease is the result of the inoculation."
Keanu has since succumbed to the leprous disease.
The inoculability of leprosy once established, its communicability by ann-to-arm
vaccination must be accepted, and in order to throw some light on the subject,
Dr. Edward Arning vaccinated a number of lepers. He says —-" These experiments
lead to the result I anticipated. In cases of extensive cutaneous leprosy, in
which skin apparently healthy contains bacilli, these were likewise to be
detected in the lymph ; but there were no bacilli to be found in the lymph taken
from cases of pure Lepra nervorum, in which no traces of the bacillus is to be
found in the skin."1
Other experiments have been recorded by Drs. Beaven Rake and G. A. Buckmaster.
Most of these were negative, but we read that " Suspicious looking rods taking
fuchsin were seen in one case in vesicles raised over tuberculated ears, and in
another case in vesicles over anaesthetic patches."2 Even if these results had
all been entirely negative, it would hardly detract from the value of Dr.
Arning's careful investigations. Further evidence of the communicability of
leprosy by vaccination is furnished by cases which have been recorded from time
to time.
1 Journal of the Leprosy Investigation Committee, No. 2, p. 131. February,
1891.
2Ibid., No. 4., p. 34. December, 1891.
SIR WILLIAM GAIRDNER'S CASES. 329
The instances which have probably attracted the most attention are those related
by Sir William Gairdner in the British Medical Journal of June 11, 1887 (vol.
i., pp. 1269, 1270) in an article entitled "A Remarkable Experience concerning
Leprosy; involving certain Facts and Statements bearing on the Question—Is
Leprosy communicable through Vaccination ? " The case as stated by Sir William
Gairdner is as follows :—
" The time seems to have arrived when, without injury or offence to anyone
concerned, it is possible to bring under the notice of my medical brethren some
facts, and some inferences arising more or less directly out of the facts, in a
case which occurred to me some years ago, but which I have found it necessary
hitherto to deal with as involving matters of professional confidence not
suitable for publication. Even now I shall deem it expedient to frame this mere
narrative in such terms as shall not point to any definite locality, or to any
recognisable person, among those chiefly concerned ; although, by a formal
certificate granted only the other day, I feel, as it were, absolved from the
last tie that bound me, even under the most fastidious sense of professional
duty, to reticence.
" Six or seven years ago the parents of a young boy, fairly-healthy in
appearance, but with a peculiar eruption on the skin, brought him to me, and
along with him a letter from a medical gentleman whom I had entirely, or almost
entirely, forgotten, but who stated himself to have been a pupil of mine in
Edinburgh considerably over twenty years before. It is unnecessary to enlarge on
the particulars of this case further than to state that, after more than one
most careful examination, in which I had the assistance of my colleague,
Professor M'Call Anderson, we came to the conclusion which we announced to the
parents, that the boy was suffering from incipient, but still quite well-marked,
leprosy in its exanthematous form; a diagnosis afterwards amply confirmed. What
struck me at the time as most peculiar was, that this case, coming from a
well-known endemic seat of leprosy (an island within the tropics) and with a
letter involving medical details by a medical practitioner of many years' local
experience ; sent to me, moreover, for medical opinion and guidance, should not
have been more frankly dealt with by a diagnosis announced even to the parents,
before they left the island. The father of the child was a sea-captain
constantly engaged in long voyages—for the most part between this country and
the island alluded to. Both father and mother were Scotch, and there were
several other children, all reported as quite healthy, as also were both the
parents. Under these circumstances I wrote to the medical man—who in the sequel
may be called, for brevity, Dr. X.—simply stating the diagnosis arrived at, and
indicating the line of treatment proposed. The parents were informed that it
would be best for the child to live in this country, and his mother agreed to
remain with him accordingly. And, as they appeared anxious to have every
available suggestion and advice, I mentioned the name of Dr. Robert Liveing as
having given much attention to the subject, and offered to write to him if they
would take the boy to London, as they appeared desirous of doing. Although I
wrote to Dr. Liveing, circumstances unknown to me led to a change in their
plans, and, instead of going to London, they went to Manchester, where I believe
some physician was consulted, but I do not remember who he was. Ultimately, the
mother determined for a while to settle in Greenock, and I placed her
accordingly in communication with Dr. Wilson of that town, who for some time
thereafter remained in medical charge of the case.
" Meanwhile, the course of post brought me in a few months a reply from Dr. X.,
not only entirely assenting to our diagnosis as communicated to him, but stating
that he had been perfectly well aware from the first of the case being one of
leprosy, but had deliberately chosen not to affirm the fact or even to allude to
it in any way, either in his communications with the parents or in his letter to
me. No reason was assigned for this (as it appeared to me) very remarkable
reticence ; but, as I did not wish to have the credit of having discovered for
the first time what a gentleman so much more familiar with the disease might
have been supposed to have overlooked, 1 took means to inform the parents of Dr.
X.'s reply, and of his having been all along of the same opinion with regard to
the disease as we were.
SIR WILLIAM GAIRDNER'S CASES. 331
" After this the matter passed out of my mind, and for several years I neither
saw nor heard of this child except accidentally, and in a way entirely to
confirm first impressions. About three years ago, however, while engaged in
lecturing on specific diseases, and among others, briefly, on leprosy, I made an
effort to find out something more about this patient. The mother had removed
from Greenock, and had brought over the whole family to Helens-burgh, where, as
I learned, they were visited by Drs. Reid and Sewell, and from the latter I now
learned that the poor boy had gone steadily to the worse, and was extremely
feeble, covered with sores, and in a most deplorable condition physically, but
still receiving every attention and care that constant medical treatment, with
the most faithful and loving maternal nursing, could afford to lighten his
sufferings. I accordingly proposed, within the next few days, a visit to my old
patient as a matter of satisfaction to myself. Unhappily there was no other
apparent object, either as regards diagnosis or treatment, for a visit which
was, nevertheless, very gratefully accepted.
" The case was now in the most advanced stage of leprosy, proceeding to
mutilation of the extremities, and accompanied not only by external sores, but
presumably by internal lesions, which had reduced the patient to the last stage
of emaciation. It was on this visit that the curious particulars now to be
related were first brought to my knowledge by Dr. Sewell, and afterwards
confirmed by the statement of the mother, showing very clearly, though, of
course, upon second-hand information to a certain extent, that Dr. X. had a very
special reason for his extraordinary reticence in the first instance. Her
husband, who in his frequent voyages had opportunities of coming into
communication with Dr. X., had remarked to him how very strange it was that,
even in writing to a medical man about the case, he had given no hint of his
opinion about it. The doctor's reply to this was, in the end, to the effect that
he had kept silence because he did not wish to compromise a boy of his own, whom
he (Dr. X.) believed to be a leper, and from whom he believed at the time that
the boy he had sent to this country had become infected with the disease. He
further explained that he had vaccinated his own boy with virus derived from a
native child in a leprous family, and, as I
understood (though perhaps not definitely so stated) that leprosy had declared
itself in the native child after the vaccination ; and, further, that (using his
own child as a vaccinifer) he had vaccinated our patient directly from him.
Before sending the last-named patient away with his parents, he had satisfied
his own mind not only that his own boy was leprous, but that he had in this way
become the source of the disease to another ; but the disease in his own child
being in a very mild form, he was anxious not to disclose its existence.
Meanwhile Dr. X. had died ; his estate had passed into the hands of trustees;
and I was informed that this reputed leper-boy had been, under the instructions
of his father and his guardian, placed and retained at a public school well
known to me in this country, and that the boy was pursuing the usual course of a
public school education, in entire unconsciousness of the disease with which he
was supposed to be affected.
"This information, so communicated, placed me in rather a difficult dilemma,
namely—was I justified in taking steps to ascertain the truth of the story as
regards Dr. X.'s boy, either by personal investigation or, at least, by
inquiries conducted so as to result in a well-grounded and scientifically exact
opinion as to the facts? And, further, supposing that such opinion should turn
out to be that Dr. X.'s boy was a leper, was it a matter of duty on account of
others to formally disclose the fact, be the consequences to the boy what they
might? It was hardly probable that a boy generally known to be a leper would be
retained permanently in any public school in this country, even had it been
unquestionably a matter of medical doctrine that such a proceeding was quite
safe. On the other hand, the boy was receiving the benefits of an English
education at the express wish and on the responsibility of his father and
guardian, and without (so far as appeared) any misgivings on the part of anyone.
He was an orphan, and in what was to him a foreign land ; his remaining under
instruction might be, and probably was, a matter of the greatest possible
importance to him. To bring him, therefore, even by an indiscreet inquiry,
under the ban which in many or most countries still attaches to leprosy was
certainly no part of the business of an outsider, and could only be justified
at all by an overwhelming sense of duty to others.
SIR WILLIAM GAIRDNER'S CASES. 333
" Under these circumstances I thought it well to consult, privately, one or two
of those friends in London whom I believed to know most about leprosy, and among
others Dr. Liveing, whom I was able to remind, at this stage, of my previous
letter. These friends concurred in assuring me that, in the rather improbable
event of their being personally consulted as to the retention of a leper in a
public school (it being presumed, of course, that he was physically fit
otherwise), they would have no hesitation at all in affirming that the other
boys would not be endangered by such proceeding. As I happened to be very well
acquainted with one of the medical officers (though not the ordinary medical
officer) of the school in question, I communicated these opinions to him, and
stated to him at the same time the extraordinary circumstances which had
begotten, for me, such a lively interest in the son of Dr. X. In the course of a
few days I was informed that an inquiry had been held by the medical staff; that
the boy had been sent for and privately examined (though not ostensibly ill in
any sense) ; and that it was, beyond all doubt, considered to be a case of
leprosy. The medical authorities decided, however, that under the circumstances
it was not their duty to sound the alarm, or in any way to disturb the boy's
education.
" From this time onwards (except the death of the first patient soon afterwards)
I heard nothing more of these matters till a few weeks ago, when I was asked to
see Dr. X.'s son professionally on behalf of the school authorities ; and, if so
advised, to request Dr. Anderson also to give an opinion as to the present state
cf health of this young man, who happened at the time to be visiting some
friends in Glasgow. It was represented to me that he had maintained, on the
whole, fairly good health since I last heard of him through my medical friend,
and had not been incapacitated from school work except on account of a
contagious eczema which had been prevailing, and with which he had been affected
in common with other boys. Apparently, however, the opinion had arisen that his
general health was not quite so good, and that in view of a cutaneous affection
of this kind, apparently communicable, existing, it was no longer expedient that
he should remain at the school. Indeed, I could not but come to the conclusion
that his removal, on public grounds, had been practi-
cally settled ; and, with every desire to soften the blow as much as possible to
the poor boy, it was felt to be necessary that his guardian, at least, should
receive unequivocal and unbiased testimony as to the actual state of the facts
and circumstances under which the decision was arrived at. Under these
circumstances I saw and examined this boy, and made a report, along with Dr.
Anderson, to the effect that the disease was evidently leprosy, though of a
remarkably mild type, as shown by dis-colourations and cicatrices, and also by
large anaesthetic areas on the back of one limb. All breaches of surface,
however, and all discharge had ceased at the time of our report, and Dr.
Anderson felt still in a position to affirm that no danger to others could occur
from the boy's remaining at school. On this last point I did not feel able to
give an unqualified assent to my colleague's opinion ; but as regards the
matters of fact and observation there was no doubt whatever, and our report
accordingly on these was substantially as above."
In a subsequent communication, Sir William Gairdner says—" Dr. X. confessedly
vaccinated his own child from a leprous family, though probably not from an
actual or apparent leper, and then vaccinated the ' sea-captain's boy' from his
own."1
Mr. C. N. Macnamara, in alluding to these and other cases of a similar kind,
remarks that they " seem to render it probable that leprosy may be conveyed from
an affected to a healthy person in vaccine lymph ; and in localities where
leprosy is endemic, we should be careful as to the source from which vaccine
lymph is obtained."2
One of the earlier references to the subject was by Sir Ranald Martin, who says,
"The dangers to Euro-
1 British Medical Journal, October 8, 1887, vol. ii., pp. 799, 800.
2 Art. on Leprosy in Davidson's '' Hygiene and Diseases of Warm
Climates," p. 445. London. 1893.
SIR RANALD MARTIN'S CASE. 335
peans arise chiefly from vaccination, and from wet-nursing. I felt that very
early in my career in India, and I took the precautions which are here recorded.
I saw an English lady last year in a horrible condition (she said), from having
been vaccinated from a leprous native child." *
Dr. Hall Bakewell, who has occupied the position of Vaccinator-General and
Medical Superintendent of the Leper Hospital at Trinidad, also alluded to cases
before the Select Committee of the House of Commons in I§71 (Q- 3;564). "I have
seen several cases in which it (vaccination) seemed to be the only explanation.
I have a case now under treatment of the son of a gentleman from India who has
contracted leprosy, both the parents being of English origin. I saw the case of
a child last year who, though a Creole of the Island of Trinidad, is born of
English parents, and is a leper, and there is no other cause to which it is
attributable."
Mr. John D. Hillis gives the following cases, in which he says there could be no
doubt the disease was produced by vaccination.
"Joseph Francis C—, a fair Portuguese, born in Demerara, now aged twenty years.
His parents are alive and healthy. He has been suffering for the last ten years
from tuberculated lepra. He has a sister, aged eighteen years, at present (1879)
an inmate of the Asylum, suffering from the same form of leprosy. They were both
admitted on July 30, 1877, from Murray Street, Georgetown. They have three
sisters and one
1 Report on Leprosy by the Royal College of Physicians, Appendix, p. 227.
London. 1867.
brother, who are alive and well. Our patient, J. F. C—,
and his sister were vaccinated with lymph obtained
from a member of a Portuguese family1 in whom
leprosy was afterwards found to exist. They were
the only members of the C— family vaccinated
with this lymph. Within eighteen months of the
performance of the operation by Dr. -- a reddish-
brown spot appeared on the inner side of the right
thigh, preceded, it is stated, by some constitutional
disturbance ; this spot was raised and tender, accom
panied by profuse sweating all over the body, and
remained for some time. Subsequently other spots
made their appearance on the right buttock (which
disappeared shortly after), between the shoulders, and
on each cheek. They were all ushered in by more
or less well-marked febrile symptoms. A red patch
next appeared on the forehead, and epistaxis set in,
periodically occurring to this day. Tubercles then
made their appearance on the face, the other patches
continuing to increase in thickness and roughness, and
forming tubercular infiltration. The latter was re
moved by gurjun oil, under which treatment many of
the symptoms were ameliorated."
"State and Condition on November30, 1879.— He has a light-brown irregular patch
on the front of his chest; this has been larger, thicker, and mahogany-coloured,
and has evidently undergone partial absorption. There is a patch of tubercular
infiltration on the back of the arms, and at the bend of the elbows. The
fingers are
1 Mr. Ilillis says, " It is within the knowledge of Dr. Manget, Surgeon-General,
and the author, that this family are at present afflicted with tuberculated
lepra."
MR. HILLIS' CASES. 337
swollen, shining, and dark-looking, a solitary tubercle forming on the back of
the hand. The swollen condition of the fingers and hands is very
characteristic. There are two tubercles on each cheek, the size of large marbles
; the lobes of the ears are thickened, and a tubercle is forming on the upper
tip. There is no appearance of hair growing on the face. There are reddish-brown
discolorations on the front and back of the legs. There are a few small
scattered tubercles on the dorsum of the feet, and the lower part of the legs
are swollen and hard to the touch. There are tubercles on the scrotum, an ulcer
on the leg where a tubercle has ulcerated, and the larger tubercles are slightly
anaesthetic. This young man is one of the carpenters of the institution ; he is
in hopes the treatment now being adopted may yet arrest the disease, which is
however, making slow but sure progress."l
Mr. Hillis2 quotes the following case from a work by Dr. Piffard, of New York :—
" William T—, aged twenty-five years, was admitted into Bell Hospital in May,
1864. He was of English parentage, but was born and passed his early life in
British Guiana. After a vaccination performed when young, his arm became greatly
swollen and inflamed, and large sloughs separated. Investigation revealed the
fact that the vaccine virus had been taken from a negro whose mother was a
leper. At the age of seven years some brownish spots appeared upon his back and
arms ; and at the age of eleven a blister formed on the
1 " Leprosy in British Guiana," pp. 30, 31. London. 1881. * Ibid., p.
208.
palm of the right hand, followed by permanent contraction of the flexor
tendons. A few months later he felt a tingling sensation around the nail of the
right index finger, followed by a line of suppuration and loss of the nail. The
finger soon healed, but the same morbid process separated itself in the other
fingers of the same hand. After a few months, according to his statement, the
skin of the distal phalanges split, and the flesh shrank away from the bones,
leaving them exposed. The bones separated at the joints and the stumps healed.
These various processes occupied eighteen months or two years. The disease then
affected the distal phalanges of the left hand in the same manner. After this it
attacked the right foot, and a slough formed over the lower part of the instep.
The great toe then became swollen, the skin split, and its distal bone
separated, then, without much regularity, the remaining phalangeal bones of
fingers and toes necrosed and came away."
Sir Erasmus Wilson relates a case in the 1867 Report of the Royal College of
Physicians (Appendix, p. 235).
Elephantiasis tuberculosa; duration of latent period, two years ; total
duration, five years ; no pains ; febrile attack simulating rubeola; vaccinated
Jrom a native child.
" A young gentleman, aged sixteen, with fair hair and complexion, and somewhat
more youthful in appearance than might be expected of his age, has been
afflicted with the tubercular form of leprosy about five years. He was born in
Ceylon, is the son of European parents, and one of six children, all
of whom are
OPINION OF THE COLLEGE OF PHYSICIANS. 339
healthy. His father and mother have always enjoyed good health, the father
having resided in Ceylon for twenty years, the mother since her marriage. He was
nursed by his mother, but vaccinated with lymph taken from a native child." (For
detailed description of symptoms, see Physicians' Report.)
The College of Physicians, in their Report (p. lxxiv., foot-note), refer to the
evidence of Sir Erasmus Wilson and Sir Ranald Martin thus : " The question
alluded to in the communications from Mr. Erasmus Wilson and Sir R. Martin (vide
Appendix) as to the transmission of leprous disease by vaccination and
wet-nursing, is one of special interest to Europeans resident in India and other
tropical countries, and calls for a searching examination."
The following case of Elephantiasis ancesthetica is also recorded by Sir Erasmus
Wilson.1
'' A lady, aged twenty-six, the wife of an officer of the Indian army, became
affected with elephantiasis in 1861. She was born in Calcutta of European
parents, and brought to England when two years old ; she returned to India in
1853 ; was married in 1855 ; has been eight years married, and has now (1863)
revisited England for medical treatment, the length of her residence in India
being ten years. In 1861, being then in Oude, she was vaccinated from a native
child, and shortly after the vaccination ' a slight spot came on her cheek, and
increased in size to the diameter of a shilling.' It was hard to the touch, a
little raised above the level of
1 "Diseases of the Skin" (sixth edition), pp. 620-622. Erasmus Wilann F
Ti.S. T.nnHnn. tX6-7.
the surrounding skin, and of a dull red colour, without pain or tenderness. The
swelling was painted with iodine, and afterwards blistered several times, and
the blister kept open ; but although somewhat reduced in size, the prominence
was not removed. About six months later, dull red flat spots appeared, dispersed
over the greater part of her body. Her hands and feet became swollen, and she
had pains of some severity in her joints and feet."
The following cases were published in an article by Dr. Daubler in " Monatshefte
fur praktische Derma-tologie," February I, 1889, vol. viii., pp. 123-129.
Case 1. Mrs. H—, from W—, thirty-six years of age, married, and the mother of a
healthy child of twelve. The closest inquiries established beyond doubt that her
family was quite free from leprosy. Several years previously, in consequence of
an epidemic of small-pox, she was re-vaccinated. During the two months
immediately following re-vaccination she experienced attacks of shivering three
to five times weekly, was thirsty, but passed less urine than usual; at the same
time the vaccine wounds swelled and became brown, and the patient experienced
great lassitude. The patient had been vaccinated in three places on each arm
over the insertion of the deltoid, and when she saw the medical man two and a
half months after vaccination the vaccine wounds were swollen. The swelling had
been noticed on the third day after vaccination, and reached its greatest height
eight days afterwards. At this time the parts became yellowish, and fourteen
days after vaccination around each of the vaccine cuts there was a raised
yellowish-
DR. DAUBLER'S CASES. 3,
brown discolouration of the skin of the size of a tw shilling piece. These
patches gradually became flatt after about five weeks from the date of
vaccination, b increased in area, and when seen by her doctor fr weeks after
vaccination the skin of the arms and the upper third of the forearms was brown
in colo and wrinkled. The brown spots extended still furthi and after three more
weeks, during which time she w feverish and ill, the patches became smaller and
smalli but the skin never regained its normal colour. In tl fourteenth week
after vaccination she had a seve rigor, which was twice repeated during the
followii week; subsequently the attacks of fever were le frequent and violent.
At and shortly after the tin of the most severe rigors brownish spots appean on
the forehead and cheeks. Eighteen weeks aft vaccination tubercles developed on
the bro and shortly afterwards on the cheeks. Two yea later the woman was sent
to the leper asylu at Robben Island, where she was seen and phot graphed by Dr.
Daubler, tubercular leprosy havir fully developed.
Dr. Daubler here gives a minute description of tl symptoms, and with regard to
vaccination he says th the old vaccination scars were visible, but there we none
from the re-vaccination which took place thr and a half years previously, as
there were then 1 pustules formed, but only swelling and discolouration the skin
occurred.
Case 2. R. du Toit, a half-caste girl, aged fiftee also from W—, and in whose
family no cases of lepro; ever occurred. The patient stated that she had alwa
been healthy till vaccination, which was performed by the same doctor, and at
the same time as Mrs. H—. At first the same local appearances were noticed on
the arms as in the case of Mrs. H—, but after two months, prominent dark patches
appeared on the forehead and cheeks, and after three months more, leprosy was
fully developed on the forehead. When seen and photographed by Dr. Daubler, the
disease had lasted three and a half years. Inquiries made in W— (the domicile of
the two patients), and also from the doctor who performed the vaccinations,
showed that the person from whom the lymph was taken to vaccinate these two
patients had died a short time previously from tubercular leprosy, other
members of the family being leprous, facts of which the doctor was, however,
ignorant.
Concerning the question as to whether vaccination is responsible to any extent
for the spread of leprosy in certain countries, the following from Dr. Edward
Arning is not without interest:—
" Another point which requires our notice regarding the Hawaiian leprosy
epidemic, and which was specially raised by the late Dr. Hillebrand—' Has
leprosy been spread in that island by means of universal vaccination?'
" There can be no doubt as regards the synchronous-ness of the diffusion of
leprosy and the introduction of vaccination into the Hawaiian Isles ; but it
still remains an open question whether it is possible to form a positive
causative connection between the two. I find that the first authentic record of
leprosy cases dates from the year 1830, though the terrible diffusion of the
disease over the whole group of islands occurred twenty-five years later, at a
time when a severe small-pox epidemic
DOES VACCINATION SPREAD LEPROSY? 343
was raging. This occasioned universal vaccination which, however, was performed
in a careless way, and principally by laymen. And it is this fact that
Hille-brand and others consider the foundation for their argument regarding the
diffusion of the disease by means of vaccination. We do not desire to overlook
this fact of simultaneousness, but we are able to give it a different
explanation. When we consider that cases of well-defined leprosy existed in
1830, we must necessarily date the importation of the disease some few years
earlier. During the subsequent few years we perceive that the disease gradually
expanded around the centre of origin. The explanation of the apparent sudden
diffusion of the disease at the beginning of 1850, must lie in the fact that
leprosy is essentially a family disease, though possibly neither congenital nor
hereditary. A sufficiently long time had elapsed from the time of the
importation of the disease down to the period in question, to enable a new
generation to spring up ; and this new generation formed new families, and from
each of these individual centres leprosy was again diffused. Moreover, we must
bear in mind the immense influence which from 1830-1850 the introduction of
civilisation, and the influx of a great Mongolian and Caucasian population must
necessarily have had upon the natives. There is another observation bearing upon
the connection between leprosy and vaccination, which I consider of still
greater importance. This dates from a later period in which no concomitant
factors, as in the above, come into play.
" I am able to state—having excellent authority for so doing, though
unfortunately no statistics—that a
very remarkable local accumulation of fresh leprosy cases took place in 1871-72,
in a place called Lahaina, on the Island of Mani. This happened about one year
after a universal arm-to-arm vaccination, which had been most carelessly
performed. About fifty to sixty cases occurred suddenly in this locality, which
up to that time had been comparatively free from the disease." 1
Dr. Arning emphatically condemns arm-to-arm vaccination in leprous
countries. He says—
" When in Hawaii I attended a German boy, aged twelve, who suffered from
leprosy, from whom when he was seven years old, several white families had been
vaccinated. I am not able to assert that leprosy was specially diffused on
account of this, but still I consider such a fact to indicate that an arm-to-ann
vaccination should be prohibited in countries in which leprosy abounds."2
In a recent essay by Dr. James Cantlie, we have further corroboration that in
the Sandwich Islands and elsewhere, the spread of leprosy has to a certain
extent been caused by vaccination. A series of questions were sent out to a
number of authorities in China, Indo-China, Malaya, the Archipelago, and
Oceania, and among them it was asked, " Has leprosy increased with the use of
vaccination ? "
Among the replies are the following important testimonies :—
Dr. Macdonald, of Fatshan, near Canton, says, " I think leprosy is on the
increase with the increasing
1 Journal of the Leprosy Investigation Committee, No. 2, pp. 130-131 (February,
1891). "Ibid., pp. 131, 132.
DOES VACCINATION SPREAD LEPROSY? 345
population of the country, and that vaccination is a slight factor in the
increase. Lack of efficient segregation, however, accounts for most of it." J
With regard to Swatow, Dr. Anna Scott reports (p. 308), " I answer a most
emphatic ' yes' to this question. The increase of leprosy among children is
frequently remarked upon by our (mission; people, and I have been forced to the
conclusion that vaccination from arm to arm, practised by a class of Chinese
(quack) doctors has caused this very marked increase."
Dr. Albricht, of Sourabaya, Java, writes (p. 358)— " I cannot bring decisive
proof that there is a connection between vaccination and leprosy, but the
tendency of belief is in that direction."
With regard to Hawaii, Dr. C. B. Wood writes (pp. 375, 376)—"A number of years
ago, when arm-to-arm vaccination was practised, it undoubtedly helped to spread
leprosy. All vaccine now used is imported, hermetically sealed." And Mr. Richard
Oliver reports to the same effect (p. 376)—" In years gone by vaccination
undoubtedly caused increase of leprosy, owing to the lymph being obtained
indiscriminately and carelessly."
With these important testimonies from responsible officials, it is difficult to
resist the conclusion that vaccination has acted as a factor in the spread of
leprosy.
Erysipelas.
Erysipelas and allied septic conditions are perhaps the most frequent of the
more serious complications of
1 "Prize Essays on Leprosy," p. 305. Thompson and Cantlie. New Sydenham
Society. London. 1897.
vaccination. The recorded deaths from "erysipelas after vaccination" in England
and Wales for the years 1859-80 are as follows. Since 1880 the deaths from
"erysipelas after vaccination " have been merged into the general heading of
"Cow-pox and other Effects of Vaccination."
Deaths from
Deaths from
Year. erysipelas after
Year. erysipelas after
vaccination.
vaccination.
1859 ... ... 5 I 1870 ......... 2O
1860 ... ... 3 1871 ... ... 24
1861 ... ... 2 1872 ... ... 16
1862 ... ... 3 1873 ••• •■• '9
1863 ... ... II 1874 ... ... 29
1864 ......... 13 1875 .......... 37
1865 ... IO 1876 ......... 21
1866 ......... IO 1877 ......... 29
1867 .......... 4 1878 ........... 35
1868 .......... 9 1879 ............. 32
1869 .......... 19 1880 ............. 39
It must not be assumed that these deaths are all that have occurred from "
erysipelas after vaccination" during the period named. This matter will be
further discussed in a subsequent part of the present chapter.
The early descriptions of cow-pox seem to show that a certain amount of
inflammation is a part of the disease itself. _,enner, in his account of the
vaccination of his first casr Phipps, describes an efflorescence spreading round
the incisions, which had more of an erysipelatous look than was commonly seen
when small-pox was inoculated. Again, he says:—"In calling the inflammation,
that is excited by the cow-pox virus, erysipelatous, perhaps I may not be
critically exact, but it certainly approaches near to it."1
1" Further Observations on the Variohc Vaccina, or Cow-pox," p. 61. Edward
Jenner, M.D., F.R.S. London. 1799.
COW-POX AND ERYSIPELAS. 347
Jenner records an instance in which " an extensive inflammation of the
erysipelatous kind, appeared without any apparent cause upon the upper part of
the thigh of a sucking colt."1 The disease was communicated to a herd of cows,
and thence to milkers; and produced in them true cow-pox. Jenner's writings,
however, do not appear to inspire that confidence which we might have
anticipated, and thus it may be thought advisable to supplement his evidence.
One of the leading German authorities, Bohn, concluded that " the lymph of a
true Jennerian vesicle, pure and clear, is therefore endowed with a power of
engendering erysipelas."2 I may also mention that Unna,3 in his work on the
pathology of the skin, in describing a normal vaccination with animal lymph,
talks of the contents of the pock on the ninth or tenth day as "seated on a
deeply-reddened, erysipelas-like, swollen base."
The following are a few of the cases of vaccinal erysipelas which have been
described from time to time :—
In The American Journal of the Medical Sciences*' for October, 1850, Mr. W.
Morland, the Secretary of the Boston Society for Medical Improvement, gives
extracts from the records of the society, relating to erysipelas following
vaccination, and reported on by medical men. Eleven cases were given, three
being fatal; of the eight
1 "An Inquiry into the Causes and Effects of the Variolie Vaccin<e" p. 72.
Edward Jenner, M.D., F.R.S. London. 1798.
2 " Handbuch der Vaccination," p. 174. Leipzig. 1875.
3 "The Histopathology of the Diseases of the Skin," p. 449. By Dr. P.
G. Unna. Translation from the German by Norman Walker, M.P.,
F.R.C.P., Ed. Edinburgh and New York. 1896.
4 The American Journal of the Medical Sciences, N.S., vol. xx., pp.
318-321.
non-fatal ones, four were very severe, of which three were attended with
extensive sloughing.
In the Dublin Medical Press1 of April 25, i860, Dr. J. Smith Chartres related
that in the previous October he had under his care four cases of severe
phlegmonous inflammation of the upper extremity occurring after vaccination ; in
one instance the destruction of the tissues was so extensive as to necessitate
amputation.
Mr. J. W. Wells, in the Lancet of May 30, 1863 (vol i.,. pp. 618, 619), relates
the case of a lady, aged 55 years, who underwent re-vaccination ; symptoms of
phlegmonous erysipelas developed on the following day, and she died four days
after the operation.
In 1876 there was an official Inquiry at Gainsborough by Mr. Netten Radcliffe,
of the Local Government Board,, into cases of erysipelas following vaccination,
of which six died ; a searching investigation failed to dissociate the operation
from the fatal erysipelas.
In 1882 another Local Government Board Inquiry was held by Mr. Henley and Dr.
Airy at Norwich into certain deaths alleged to have been caused by vaccination.
It was shown that eight children suffered from erysipelas "due to some abnormal
peculiarity or contamination of the lymph ;"2 of these, four died.
On the 25th May, 1883, sixty-eight recruits3 were vaccinated at Dortrecht,
Holland. Of these seven were
1 Dublin Medical Press, 2S., vol. i., pp. 323, 324.
2Copy of "Report to the President of the Local Government Board by the
Inspectors Appointed to Inquire into certain Deaths and Injuries alleged to have
been caused by Vaccination at Norwich" p. 9. Ordered by the House of Commons to
be printed, 24th October, 1S82.
3 Q. 9,465-8. Third Report, Royal Commission on Vaccination.
DR. VACHELL'S CASES. 349
attacked with erysipelas, and three died. In consequence of these cases, the
Minister of War, Mr. Weitzel, issued a circular notifying recruits that
hereafter re-vaccination was not obligatory in the Netherlands army.
Before the South Wales and Monmouthshire Branch of the British Medical
Association,1 on November 15, 1883, Dr. C. T.Vachell, of Cardiff, related a
series of cases where erysipelas followed vaccination. On November 1, a child,
aged three months, and an adult were vaccinated with lymph obtained from
London. On the eighth day the arm of the adult was much swollen and red. On the
same day the child presented every appearance of having been successfully
vaccinated, and five tubes were charged from it. On November 10 five children
were vaccinated from these tubes. On the nth and 12th all these cases were
attacked with erysipelas of the arm vaccinated, and, on inquiry, it was found
that the child from whom the vaccine lymph had been taken was attacked with
erysipelas on November 9.
The Lancet of November 24, 1883 (vol. ii., pp. 919, 920), relates on the
authority of the Suffolk and Essex Free Press that two children named Elliston
and Griggs were vaccinated on October 16. They remained well until their visit
to the vaccination station on October 23, when one of them supplied lymph for
the vaccination of two other children, and was noticed by the mother to have a
swollen face at the time of leaving the station. Subsequently the vaccinifer
and one of the vaccinees died from erysipelas, as well as the other child
vaccinated on the 16th October.
1 British Medical Journal, December 15, 18S3, vol. ii, p. 1213.
Dr. P. S. Fentem, in the Lancet of December 8, 1883 (vol. ii., p. 1010), reports
the following :—On October 2 he vaccinated seven children from the same tube of
lymph. Three of them developed symptoms of erysipelas about the vaccination
marks on the twelfth, thirteenth, and fourteenth days afterwards, and one
terminated fatally. He noted that the sanitary surroundings in two of the cases
were unsatisfactory, but attributed the erysipelas to a certain kind of soap
used to wash the clothes of the three children.
Examples of acute septic poisoning occurred in the course of some vaccinations
at Asprieres (Aveyron) in the month of March, 1885. An official report was
issued, from which it appeared that forty-two infants were attacked, six of whom
died. The symptoms of those who died comprised repeated vomiting, diarrhoea,
great agitation, and, in two cases, convulsions.1
Among the older records of the Local Government Board are the following :—2
(1) A series of nineteen cases of erysipelas from vac
cination at Warrington, with five deaths, in 1871.
(2) A case of serious erysipelas from vaccination
with National Vaccine Establishment lymph at Stoke
Newington in 1871, in which inquiry elicited that
violent inflammation had occurred in others vaccinated
with lymph from the same vaccinifer; the vaccinifer
having an inflamed arm on the thirteenth day and a
small abscess in the axilla.
1 Third Report, Royal Commission on Vaccination, Appendix, pp.
210-
213.
2 Royal Commission on Vaccination, Dissentient Commissioners'
State
ment, section 192.
VACCINAL ERYSIPELAS. 35 I
(3) Six cases of serious inflammation and three
deaths in a series vaccinated with ninth-day lymph
from one vaccinifer at Appleby in 1873.
(4) Several cases of erysipelas and inflammation with
five deaths in a series of vaccinations at Chelsea, in 1875.
(5) Twelve cases of excessive inflammation, six of
erysipelas with three deaths, two cases of axillary
abscess, and one large ulcer in a series of vaccinations
■ at Plomesgate, in 1878.
(6) Ten cases of erysipelas or abscesses with four
deaths and several cases of eczema in a series of vac
cinations at Clerkenwell in 1879, in which "it is clear
that the erysipelatous contagion was imparted at the
time of vaccination."
(7) Three cases of extensive erysipelas from vaccina
tion at Blandford in 1883.
(8) Three fatal cases of erysipelas from vaccination
at Sudbury in 1883.
Between the 1st of November, 1888, and the 30th of November, 1891, one hundred
and thirty-two cases of inflammatory or septic disease (mostly erysipelas)
following vaccination and terminating fatally, were the subject of inquiry by
the Local Government Board. Numerous cases have also been investigated by the
Royal Commission on Vaccination, and are cited in Appendix ix. to their Final
Report.
Cases of erysipelas following vaccination are not infrequently objected to on
the ground that the disease must have been acquired subsequently to the act of
vaccination, and therefore, it is said, preventable.
Doubtless many cases may be attributed to the careless treatment of arms,
insanitary surroundings of the
patient, and other conditions not directly related to the operation ; but the
State which compels vaccination will hardly escape responsibility for these
accidents; and, from the conditions under which a number of our poor still live,
it may be doubted whether there would not always arise cases of the description
under consideration.
Attempts have been made to distinguish these cases from those in which the lymph
itself is at fault. It has been suggested that the incubation period will afford
a means of settling the difficulty. In certain experiments made by Fehleisen1 it
was found that the incubation period varied from fifteen to sixty-one hours ;
but it must be remembered, as Dr. Acland has pointed out, that clinical
observation gives " much wider limits."2 The length of the incubation period of
erysipelas may vary "in a remarkable degree,"3 as has been shown by certain
series of cases reported on by medical men on behalf of the Vaccination
Commission, where several of the children vaccinated at or about the same time
have been affected, and thus pointing to a contamination of the lymph.
Thus in a series of cases in some villages near Norwich (No. 23), Dr. Barlow
found from his brief provisional investigation that " some septic material had
been introduced at the time of the insertion of the vaccine lymph."* The
inflammation commenced at intervals from the first to the tenth day.
1 " Bacteria in Relation to Disease," p. 283. Edited by W. Watson
Cheyne, M.B., F.R.C.S. New Sydenham Society. 1886.
2 Appendix ix., Final Report, Royal Commission on Vaccination, p. 246,
foot-note.
3Ibid., p. 294. * Ibid., p. 232.
VACCINAL ERYSIPELAS. 353
In a series investigated by Dr. Acland (No. 115) there was a still greater
range, that is to say, the erysipelas appeared at intervals of six hours,
sixteen hours, five days, and nineteen da}7s in four cases where it was almost "
a certainty that the infection of the erysipelas was derived from the
vaccinifer." :
Dr. Acland also records another series (No. 181) of six children attacked in
whom "it can hardly be doubted that the abnormal results were due to the quality
of the lymph."2 The period varied from two or three days to more than two weeks.
For further testimonies regarding the variability of the incubation period of
erysipelas see Tillmanns in Deutsche Chirurgie vol. v., pp. 96, 120, 121,
Stuttgart, 1880.
It is also argued that if only one or two children suffer out of a certain
number vaccinated, that this would exclude the lymph ; but it may be pointed out
that in cases of syphilis it is unusual for all those vaccinated with the same
lymph to be attacked. Thus Trousseau 3 records an instance where only one out of
five children vaccinated from the same vaccinifer contracted syphilis; and in
the Paris case recorded by Gudrin 4 one out of forty infants vaccinated was
attacked. Mr. Jonathan Hutchinson6 remarks that in his first series of cases two
out of twelve successfully vaccinated
'Appendix ix., Final Report, Royal Commission on Vaccination, p. 294.
"Ibid., p. 369.
3 '' Bulletin de 1'Academic Imperiale de Medecine, 1 S. vol. xxx., pp. 144,
145. 1864-65.
4Ibid., 1 S. vol. xxxiv., p. 512. 1869.
5" Illustrations of Clinical Surgery," vol. i., pp. 129, 130. London. 1878.
wholly escaped, in his second series of about twenty-six cases more than one
half escaped, and in the third series only one out of twelve is known to have
been attacked, while in the fourth series only one suffered and probably six or
eight escaped.
These facts point to the conclusion that the lymph cannot be exonerated by any
such criteria as have been suggested.
Tubercle.
In the case of consumption, tubercle, and scrofula, there is not the same amount
of unimpeachable evidence of their connection with vaccination as in the
diseases before considered. Dr. Acland says—" Although vaccination may be in no
way the cause of the disease, it may and must always be difficult in such cases
rightly to apportion the precise effect of inheritance, circumstances, and
vaccination ; especially if, owing to feeble health, degenerate tissues, and bad
surroundings, vaccination has been followed by ulceration, glandular abscesses,
or some other complication likely to excite febrile disturbance."1 The
Vaccination Commissioners allow (section 417) that "It may, indeed, easily be
the fact that vaccination, in common with chicken - pox, measles, small-pox, and
other specific fevers, does occasionally serve as an inciting cause of a
scrofulous outbreak." In this connection some suggestive figures are given by
two French writers, Rilliet and Barthez, who found that in 208 vaccinated
children 138 died tubercular and 70 non - tubercular, whereas in 95 children
who died unvaccinated 30 were tubercular
1 Allbutt's "System of Medicine," vol. ii., p. 623. London. 1897.
VACCINATION AND TUBERCLE. 355
and 65 not so.1 Dr. James Copland, who quotes these figures, remarks that "it
cannot be doubted that vaccination favours the prevalence of the several forms
of scrofula."2 Again he says—"Notwithstanding the laudation bestowed upon
vaccination, I believe that, as the lapse of time allows the fact to be more
fully demonstrated, it will be found to be a not unfruitful source of scrofula
and tubercles."2
Dr. Felix von Niemeycr writes :—"The injurious influence which diseases have on
the constitution, and thereby on the tendency to consumption, manifests itself
most frequently and in the most lasting manner in earliest infancy. It is
fortunate if children escape disease, particularly in the first years of their
life, during which by far the most rapid development of the body takes place,
and when by favourable or unfavourable external circumstances the foundation is
laid, in a great measure, for a strong and robust, or a weak and delicate
health. Even vaccination may, by the febrile disturbance preceding the
eruption, as well as by that accompanying the suppuration, both of which are
never absent, and according to my numerous thermometrical observations sometimes
reach a very high degree, considerably weaken, more especially those children
who are not very strong, and may leave behind it the germs of a disposition to
consumption."3
1 " Traite Clinique et Pratique des Maladies des Enfants," vol. ill., p. 116,
foot-note. Paris. 1843.
'Copland's "Dictionary of Medicine," vol. ill., pp. 740, 741. London. 1858.
3 " Clinical Lectures on Pulmonary Consumption," p. 22. Translation from the
second German edition by C. Baeumler, M.D. The New Sydenham Society.
London. 1870.
This eminent authority adds, " I must protest against unconditional
compulsory vaccination, particularly during the first two years of life."
Other writers have endorsed Dr. Niemeyer's opinion. Thus, Dr. Riihle, in an
article on " Pulmonary Consumption and Acute Miliary Tuberculosis," remarks
that " Scrofula also often appears for the first time after recovery from
certain diseases, such as the acute exanthemata, and especially measles.
Vaccination, has also been regarded as a cause, and probably correctly. It does
not, however, seem to produce scrofula directly by the inoculation of a '
scrofulous poison,' but by inducing the manifestation of the hitherto latent
scrofulous symptoms, through an abnormal course of the vaccine pustule and the
active fever accompanying it, in the same way as other febrile diseases of
children act."1
Dr. Birch-Hirschfeld, in the same work, observes :— ■" Frequent experience shows
that vaccination also may not infrequently be followed by a breaking out of
scrofulous symptoms"2—although he remarks that it is to be supposed that in the
majority of these cases vaccination only excites the dormant disease.
Apparently the German Government were fully alive to the danger, for their
statute prohibited the taking of lymph from a scrofulous child ; but, as Dr.
Birch-Hirschfeld says, " This caution, however, becomes illusory, in the
majority of cases, so far as first vaccina-
1 Ziemssen's "Cyclopedia of the Practice of Medicine" (English
■edition), vol. v., p. 485. 1875. 1 Ibid., vol. xvi,, pp. 773.
ANIMAL LYMPH AND TUBERCULOSIS. 357
tions are concerned, because scrofulosis generally does not show itself during
the first years of life, and proof for the possible existence of a scrofulous
constitution can be found only by an examination of the physical condition of
the parents, brothers, and sisters of the child." 1
It is generally held that tubercle is due to a specific organism, and hence the
possibility of its communica-bility by vaccination must be admitted. The
experiments which have a practical bearing on this subject are those of M.
Toussaint.2 He vaccinated a tuberculous cow on the vulva with lymph from a
well-formed vaccine vesicle raised on a healthy child of strong parentage. With
lymph from the pocks on the cow he vaccinated four rabbits and a pig. Two
rabbits killed two months afterwards were found to be suffering from
tuberculosis at the point of inoculation, in the glandsr and also in the lungs.
The pig developed signs of tuberculosis both local and general.
The Medical Times and Gazette, in referring to Toussaint's experiments, says, "
The significance of these experiments can scarcely be overrated ; for, though a
judicious vaccinator would not use lymph taken from a child who exhibited
already evidence of the disease, the chances of cows in whom spontaneous
vaccinia may appear, and whose lymph would at the present time be
J-Ziemssen's "Cyclopaedia of the Practice of Medicine" (English edition), vol.
xvi., p. 774.
2" Comptes Rendus Hebdomadaires des Seances de l'Academie des Sciences," vol.
xciii., pp. 322-324. 1881.
eagerly sought after, being, like so many of their species, tuberculous, are
great; and it would seem, in consequence, that the dangers of animal
vaccination may be greater than those of human, which are supposed to be avoided
by having recourse to the cow."1
Although Sir Richard Thorne, in his recent report to the Local Government Board,
refers to this danger as " very remote," it is evidently one which is
apprehended by the Medical Department of the Local Government Board ; for, with
a view of reassuring the public, he states that the tubercle bacillus, when
experimentally added to a mixture of lymph and an aqueous solution of glycerine,
rapidly loses its vitality. Considering that the researches of Dr. Arthur
Ransome2 and others have indicated that glycerine favours the growth of tubercle
in culture media, it may be anticipated that Sir Richard Thome's statement will
be received with a certain amount of scepticism.
Lupus has occasionally been found growing in the site of vaccination. Mr.
Hutchinson 3 has figured a case in a child eight years of age. The disease
occurred in and around a vaccination scar, and commenced a few months after
the operation. Cases of a like nature
1 Medical Times and Gazette, September 3, 1881, vol. ii., p. 291.
2 " Proceedings of the Royal Society" for 1897, vol. lxii., pp. 187-200.
See also Nocard and Roux in " Annales de l'Institut Pasteur" for 1887,
vol. i., pp. 19-29; Crookshank in "Transactions of the Pathological Society
of London" for 1890-91, vol. xlii., pp. 333-336, and Beevor, Ibid., pp. 344,
345-
3 " Illustrations of Clinical Surgery," vol. i., p. 141, plate xxv., fig. 1.
London. 1878.
TETANUS AFTER VACCINATION. 359
have been described by Besnier1 and Lennander.'2 Dr. Colcott Fox3 mentions three
instances of lupus in vaccination scars. In one case the lupus was left behind
when the vaccination lesions healed. A patient was also examined by Dr. Acland
on behalf of the Royal Commission on Vaccination (see No. 26, Appendix ix.;
also Mr. David Daker's evidence pp. 141, 142, Sixth Report).
Tetanus.
It will have been observed that most of the disasters alleged to be induced by
vaccination come under the heading of inoculable diseases; tetanus, or lock-jaw,
is no exception to this rule. The following cases have been reported from time
to time, and it must not be assumed that they represent the total number of
cases of tetanus attributable to vaccination.
Reported by
(1) Dr. Joseph B. Cottman. New Orleans Medical and
Surgical Journal, 1854-55, vol. xi., p. 783. Negress
affected with tetanus following vaccination; period of
time not stated. Recovery in two weeks by use of large
doses of opium.
(2) Dr. George Ross. The Southern Clinic, 1878-79,
vol. i., p. 468. Boy, three and a half years old when
vaccinated. Tetanus supervened three weeks afterwards
with death on the third day. No other lesion beyond
vaccination.
1 " Annales de Dermatologie et de SyphiJigraphie," vol. x., pp.
576, 577,
Paris. 1889.
2 " Upsala Lakarefbrenings P'orhandlingar," vol.
xxv., pp. 65-70.
Upsala. 1889-1890.
3 The Practitioner, vol. lvi., p. 500. May, 1896.
(3) Dr. Theodore Dimon. St. Louis Courier of Medicine,
1882, vol. vii., pp. 310-312. Boy, nine years old; vac
cinated January 6, 1882, with bovine lymph. Tetanus
supervened on January 27; no cause discovered except
vaccination, which was followed by an irregular shaped
ulcer. Boy died on the tenth day.
(4) Dr. H. J. Berkeley. Maryland Medical Journal,
1882-83, vol. ix., pp. 241-245. Healthy man, forty years
old; vaccinated in the middle of January, 1882. Tetanus
supervened on February 7; death on February 13. No
lesion discovered except at the point of vaccination,
which was occupied by a deep ulcer, with an inflamed
and indurated border.
(5) Dr. W. T. C. Bates. "Transactions of the South
Carolina Medical Association," 1882, vol. xxxii., p. 105.
Mulatto boy, aged five years ; vaccinated February 9,,
1882, with humanised lymph. Tetanic symptoms super
vened on March 8. No other cause but vaccination
discovered. Boy lived fifteen days.
(6) Dr. R. Garcia Rijo. " Cronica Medico-Quirurgica
de la Habana," 1886, vol. xii., p. 388. White child, two
years old; vaccinated in April, 1886; characteristic
tetanus appeared in latter part of May. No lesion
beyond vaccination discovered. Death followed on the
fourth day.
(7) Dr. Zahiroodeen Ahmed. Indian Medical Gazette,
March, 1889, vol. xxiv., p. 90. Adult, aged twenty-one ;
the symptoms appeared fourteen days after primary
vaccination.
(8) Local Government Board, Case x., Appendix ix.
Final Report, Royal Commission on Vaccination.
Female, aged two months ; vaccinated on September
io, 1889; symptoms of tetanus first appeared on October 2, and patient died on
the 5th of October.
(9) Dr. S. W. S. Toms. Medical News (Philadelphia), February 24, 1894, v°l-
lxiv., PP- 209-212. Female white child, five years five months old. Vaccinated
November 6, 1893, with bovine lymph on ivory point. Characteristic trismus on
November 30, with death on December 5.
For two recent cases of tetanus following vaccination see Medical Recoj'd, New
York, January 22, 1898, vol. liii., p. 129, and Indian Lancet, Calcutta, January
1, 1898, vol. xi., p. 42.
Dr. Acland mentions that the case included in the Vaccination Commission Reports
(No. x.) is the only one he is acquainted with in more than five million
vaccinations in this country.1 This would tend to show that in England tetanus
after vaccination is very rare, as we should expect it to be. It would be more
interesting if we had the figures for Calcutta and other parts of India. In an
address to the Medical Society of Calcutta on January 5, 1892, Sir Spencer
Wells2 stated that the infant mortality from tetanus in that city during the
years 1881-90 almost equalled that for all other infantile diseases added
together. Of course, I do not wish to imply that this large mortality is in any
way attributable to vaccination ; but before deciding the question of the
frequency or otherwise of tetanus after vaccination we should have before us the
statistics from countries where tetanus is prevalent.
1 Allbutt's "System of Medicine," vol. ii., p. 598. London. 1897.
2 Report on Sanitary Measures in India in 1891-92, p. 108.
The Amount of Vaccinal Injury.
It is impossible to form any accurate estimate of the total amount of serious
and fatal injury produced by vaccination ; the following table only gives the
deaths recorded by the Registrar-General:—
England and Wales. Deaths from Cow-pox and other effects of Vaccination, from
i88r to /Spj.
1881 ................ 58 1889
............ 58
1882 ... ... 65 1890 ...
... 43
1883 ................ 55 1891
................ 43
1884 ............ 53 1892
................ 58
1885 .............. 52
1893 ...... 59
1886 ....................... 45 1894
...... 50
1887 ....................... 45
1895 ...... 56
1888 ....................... 45
This shows that in England and Wales, according to medical death-certificates,
one child on an average dies every week from the effects of vaccination. This
fatal record, however, does not by any means represent the damage done by the
operation, as for every death there must be a very large number of children who
are injured, but survive for years with enfeebled constitutions.
It has been noticed in the earlier part of the present chapter that in all
probability cases of vaccino:syphilis remain unrecognised, and there also seems
reason to believe that, even if recognised, a certain number are unreported. In
support of this, I may quote from Professor Alfred Fournier's work on
vaccino-syphilis. He says—" There are certainly many more cases of vaccinal
syphilis on the cards or in the memories of practitioners than in the columns of
our journals. For myself, had I
DR. PRINCE MORROW'S OPINION. 363
up to this day published a single one of the numerous-cases of this kind which I
have observed, whether in my private practice or in hospital ? But how many of
my colleagues might say as much? There is more. The same reticence must have
sometimes concealed important cases. For myself alone, I had knowledge of two
actual epidemics of vaccinal syphilis, which have been kept secret, and upon
which I have been able to obtain only incomplete information, the affair having
been hushed up"1
The Royal Commission also remark (section 426) that " it is not to be forgotten
that a natural reluctance to register deaths as due to syphilis may have
prevented some cases where recently vaccinated persons have died from that
disease from being made public."
Dr. P. A. Morrow, in referring to eruptions incident to vaccination, observes—"
It must be confessed that the profession has manifested a most decided
unwillingness to recognise their direct dependence upon vaccination."2
Again, in the Local Government Board Inquiries on erysipelas, held by Mr. Netten
Radcliffe at Gainsborough, and by Mr. Henley and Dr. Airy at Norwich, before
referred to, there were in all ten deaths, and in only one of these was
vaccination mentioned on the certificate of death. Also, in an Inquiry, on
behalf of the Royal Commission, on a series of injuries from vaccination at some
villages in Norfolk, in 1890, Dr. Barlow found, from the brief provisional
investigation he was able to
1 " Lemons sur la Syphilis Vaccinate," p. 53i foot-note. Alfred Fournier.
Paris. 1889.
aJournal of Cutaneous and Venereal Diseases, vol. i., p. 176. New York.
March, 1883.
make, that some septic material had been introduced at the time of the insertion
of the vaccine lymph, and that this was mainly responsible for the untoward
results obtained. There were three deaths, and in none of these was the word "
vaccination" mentioned on the death-certificate.
In this connection Professor Schaefer, of the Women's Medical College, Kansas
City, remarks—" The pathology of vaccination is a subject upon which very
little has been written by writers on vaccination. There is no doubt that every
experienced physician has seen one or more cases of severe localised sepsis
following the operation of vaccination. It will be found, on surveying the
field, that such accidents are by no means rare, contrary to the statements of
the books, as we have been made to believe." l
Dr. Bridges, formerly Inspector of the Local Government Board, gives the
following explanation—"Medical statistics cannot be quite trustworthy on this
point from the nature of the case. A doctor vaccinating a child will obviously
be unwilling to say that vaccination did harm, unless he is a man above the
ordinary standard of courage and conscientiousness . . . statistics founded on
such uncertain facts—facts dependent not merely on the skill but on the moral
courage of the doctor, can have no possible value."2 It is interesting to notice
that history apparently has repeated itself; for Sir Richard Blackmore, writing
in 1723 about the pre-
1 Journal of Cutaneous and Cenito-Urinary Diseases, vol. xiv., p. 399.
New York. October, 1896.
2 Positivist Review, November, 1896, vol. iv., p. 225.
PREVARICATIONS OF THE INOCULATORS. 365
varications of the inoculators, says—" It is in vain to give this matter another
more favourable turn for the operators, by saying, the patient was of a weakly
constitution, and full of ill humours, or that he was of a froward and perverse
temper, and died by a fit of peevishness, or that he was carried off by
terrible convulsions, and not by the small-pox; for men of the least sagacity
must see through these ridiculous evasions invented to cover true history and
defeat our inquiry into matter of fact, and to buttress up the reputation of the
inoculators."1
On the following page he observes—" To say that the small-pox, which the
convulsions attended, was not the cause of the patient's death, but the
convulsions, is the same thing as to affirm that the axe that cuts off a
traitor's head, is by no means the cause of his death, but the effusion of blood
and trembling motions of the body, that followed the separation."
The Royal Commission (section 379), while admitting, as they were bound to do,
that some risk attaches to vaccination, have attempted to minimise the dangers
of the operation by comparing the risk to that of railway travelling; in this
they were promptly taken up by Dr. Collins and Mr. Picton in their Statement of
Dissent (section 184), who show from the Board of Trade returns that the
proportion returned as killed (from causes beyond their own control) to the
number carried by railway was 1 in about 35,000,000, while the risk of dying
from vaccination to the number vaccinated, according to the death-certificates
of medical men, was 1 in 14,159. Of course, these latter figures give no idea
1 " Treatise upon the Small-pox," p. 93. Sir Richard Blackmore, M.D.,
F.R.C.P. London. 1723.
of the total risk of vaccination, but they serve to show the bias of the
majority of the Vaccination Commissioners in their treatment of this subject.
Animal Lymph.
This new departure, recommended by the Royal Vaccination Commission, amounts to
a virtual condemnation of the arm-to-arm system which has been enforced upon the
people for half a century. It is therefore important to inquire whether a
general introduction of calf lymph, as proposed, would be attended with any
diminution in the danger which appears to be inseparable from the practice of
vaccination. In the case of syphilis, facts and considerations have been
presented to the reader for believing that this disease, or symptoms
indistinguishable therefrom, would not necessarily be excluded by the
employment of calf lymph; as the Lancet observed in criticising an article by
Dr. Henry A. Martin—" The notion that animal lymph would be free from chances of
syphilitic contamination is so fallacious that we are surprised to see Dr.
Martin reproduce it, and so contribute to the perpetuation of the fanciful ideas
which too commonly obtain on the origin of vaccino-syphilis."1
The remaining diseases which concern us in this country are tubercle, to which I
have already alluded in this connection, erysipelas, and other inflammatory
complications and skin diseases ; and, with regard to these last, there is every
reason to believe that the introduction of animal lymph would be a disadvantage
as compared with the present system.
1The Lancet, June 22, 1878, vol. i., p. 909.
MR. ROBERT CEELY ON ANIMAL LYMPH. 36;
In the American Medical Times for March 8, 1862 Dr. Henry M. Lyman observes—" It
is certain that the disturbances, produced by the use of a virus which has been
newly derived from the cow, are generally much more marked than the effects
which follow the use ol a more perfectly humanised lymph." x
With reference to the irritating effect of animal virus on the skin, we learn,
on the high authority of Mr. Robert Ceely, that " those who believe their
children will escape cutaneous eruptions when vaccinated direct from the cow,
will be greatly mistaken. Many children have skins—all children more or
less—prone to throw oul eruptions, papular, vesicular, pustular, or exanthematic
upon the excitement of the least increased vasculai action. Hence ordinary
vaccination will cause whal most other febrile and cutaneous irritations produce
Hence more irritating lymph, as it is when direct frorr the cow, will be more
effective in the production of the above results. But there is a special
vesicular vaccine eruption attending the acme and decline of the vaccine
disease. The Germans have called it ' Nachpocken.' ] have often, nay almost
always, seen it as a secondary eruption on the teats and udders of the cows
immediately before and after the decline of the disease in them The same I have
repeatedly seen in children, especially in the early removes from the cow ; and
still continue at times to witness it, to the great temporary disfigurement and
annoyance of the patient, and the chagrir and vexation of the parent. It is
essentially a genuine vaccine secondary eruption. I have witnessed
it ir
vaccinating the dog. I have coloured illustrations of this secondary eruption in
man and animals, and have seen some severe and a few dangerous cases in children
where the skin and visible mucous membranes were copiously occupied with it."1
It may also be noticed that Professor Depaul, of the Paris Faculty of Medicine,
expressed the opinion that calf lymph is more frequently followed by secondary
vaccinal eruptions.2 Ever since Ceely's day numerous authorities have pointed
out the greater potency of calf lymph: thus Dr. Henry Blanc,3 a prominent
advocate of this vaccine, in a treatise on " Compulsory Vaccination," remarks on
its "greater activity;" and the editor of The Practitioner, in reviewing the
pamphlet, pertinently observed that " the very argument which Dr. Blanc urges in
favour of the superior value of heifer vaccination is a distinct and serious
objection to it."4
By far the most damaging reports on animal lymph, however, come from those who
have had the greatest experience of its effects, viz., the vaccinating surgeons
in the United States ; for this method of inoculation was adopted in the States
much earlier and with much greater fervour than it ever has been in this
country, and for the reason that humanised virus was found to be attended with
such serious consequences.
In the Sixth Annual Report of the Board of Health
1 British Medical Journal, January 7, 1865, vol. i., p. 19.
1 Ibid., July 3, 1880, vol. ii., p. 22.
* " Compulsory Vaccination : An Inquiry into the Present Unsatisfactory
Condition of Vaccine Lymph," pp. 16, 24. Henry Blanc, M.D., F.R.G.S. London.
1869.
4The Practitioner, vol. iii., p. 236. October, 1869.
ANIMAL LYMPH IN THE UNITED STATES. 369
of the State of New Jersey, Dr. Thomas F. Wood, in answer to certain queries
relative to vaccination, says— " Vaccination with bovine lymph has brought to
light a series of phenomenal symptoms, except to those medical men who have kept
fresh in their minds the descriptions ofjenner and the early writers. Jenner
described the disease caused by early removes from the cow, and he consequently
gave a picture of only the intensest forms , of it, in his 'Inquiry' and
'Further Observations.' A glance at the coloured engravings in Jenner's great
work, in Woodville's, Pearson's, Bryce's, Willan's, and all others, shows that
the vesicle was larger and the areola more intensely red than in the cases
familiar to us up to the time of the introduction of the Beaugency lymph. The
reader of the early vaccinographers can hardly believe there was not some
exaggeration in their descriptions of the serious constitutional symptoms, and
the bad ulcers which sometimes succeeded vaccination; ulcers so bad, indeed,
that they had to be treated with solution of white vitriol."1
Continuing, he observes that "the degree of sickness is generally greater
following bovine vaccination."2
Dr. Ezra M. Hunt, Secretary of the New Jersey State Board of Health, observes
that " the degree of sickness is, as a rule, greater in a genuine bovine than in
a humanised vaccination, and quite corresponds to Jenner's statement, made as to
his own cases."3 With regard to eruptions—" Like the original cow lymph, as used
by Jenner, it is more active in its effects, and therefore is
1 Sixth Annual Report of the Board of Health of the State of New Jersey, 1882,
pp. 37, 38.
3/die/., p. 39. 3/bid., p. 51.
more likely to excite local irritation, and to be the occasion for the
appearance of some eruptive disorders, to which the person may be inclined." 1
Dr. E. L. Griffin, President of the Wisconsin Board of Health, says :—" The
constitutional symptoms following the use of pure bovine lymph, and those
induced by lymph humanised by a few removes from the heifer, are generally of a
like character and degree. In the case of both, these symptoms are sometimes
quite severe. The cause is quite often found in the condition of the patient
himself. It must be admitted that during the past year an unusual amount of
severe constitutional symptoms and local complications have followed the use of
bovine lymph."2 About skin diseases he observes—" The frequency of vaccinal
erythema following the use of bovine lymph is a noticeable phenomenon. This
constitutional manifestation of the vaccinal disease is seldom observed in the
use of humanised lymph of distant removes from the heifer." 8 Dr. Griffin
thought the eruption to be of small account, and that it only indicated a
thorough saturation of the system with the vaccinal disease.
In the Report of the Oxford Local Board to the New Jersey Board of Health, Dr.
L. B. Hoagland, in referring to an epidemic of small-pox, says—" About fifteen
hundred persons were vaccinated during its prevalence, one third of them with
humanised virus, and the remainder with non-humanised bovine virus, the
constitutional effect being much the more marked when the
1 Sixth Annual Report of the Board of Health of the State of New-Jersey, 1882,
p. 54.
■Ibid., p. 65. 3 Ibid.
latter was used. One child, of five years, lost its life by taking cold in her
arm ; gangrene set in, and she died from septicaemia. Some of the sores were
three or four months in healing."1
Dr. William M. Hartpence, in the Report of the Washington Local Board, remarks
that " Bovine virus was generally used, and our observations lead us to conclude
that the constitutional effects were greater in a larger number of cases than we
had observed in years past when using humanised virus; and, also, our
experience makes us believe that the resulting sores were longer in healing
(speaking in general) than with the humanised virus."2
Dr. E. J. Marsh, President of the Patterson Board of Health, said that although
he had tried both varieties of lymph, " In my use of bovine lymph it was
observed that the vaccine vesicle resulting was much larger, the areolaand
inflammatory induration were more extensive, the crust large, flat and thin,
generally ruptured, and came away before the sore was cicatrised. In two
instances the inflammatory action was so high that the vesicle sloughed out en
niasse, leaving a deep ulcer." 3
The Second Annual Report of the State Board of Health of Indiana, for the year
ending October 31, 1883, furnishes a list of reports on small-pox and
vaccination from the Health Officers throughout the State. The following relate
to the effects of animal virus.
Dr. Henry Gers, of Washington, reported that, three
1 Sixth Annual Report of the Board of Health of the State of New Jersey, 1882,
p. 180, 181. "Ibid., p. 182. 3Ibid., p. 70.
years previously, unpleasant effects were noticed from supposed bovine virus.
(P. 185.)
Dr. D. W. Butler, of Connersville, said that bovine virus was used entirely, and
some cases of vaccination were unusually ill, with an eruption over the entire
body. (P. 186.)
Dr. J. M. Gray, of Noblesville, remarked that in 1872 •erythema, as a result of
vaccination, was quite common. In his experience bad results were more
frequently seen after bovine virus. (P. 186.)
Dr. N. S. Shipman, of Seymour, observed that nothing but bovine virus was used,
and " in a few instances we had ulcerous-looking sores, lasting sometimes for
six months." (P. 187.)
Dr. J. T. Jones, of Franklin, reported on a great number of bad arms as the
result of vaccination with bovine virus. (P. 188.)
Dr. Horace E. Jones, of Anderson, stated that "phleg-monous abscesses and
sloughing ulcers frequently occurred" as the result of bovine virus. (P.
190).
Dr. S. H. Pearse, of Mount Vernon, reported that bovine virus only was used, and
that he saw no difference between the bovine and human. He observed that a year
previously " extensive inflammation" followed the use of bovine in two cases,
and he remarks that in consequence of a case of small-pox fourteen people in one
house were vaccinated, all of whom had sore arms. (P. 190.)
Dr. George B. Walker, of Evansville, ascertained that the bovine lymph was "
more violent and caused troublesome ulceration, and sometimes eruption over the
body." (P. 191.)
ERUPTIONS FROM ANIMAL LYMPH. 373.
Dr. C. E. Lining, of Evansville, reported some very-bad arms, more following-
the use of bovine virus.
And, lastly, Dr. J. R. Crapo, of Terre Haute, noted severe dermatitis, and an
eruption over the whole body, resembling lichen or eczema, as the result of the
use of animal lymph.
In the JournalofCutaneous and Venereal Diseases Dr. Morrow bears out the almost
universal opinion of medical men in the United States when he says—"The
experience of the profession in this country with bovine lymph shows that it is
slower in its development, more intensely irritant in its local and
constitutional effects, and more prolonged in its active continuance." 1
Dr. Alexander Napier,2 Assistant to the Professor of Materia Medica, Glasgow
University, and Physician to the Skin Department, Anderson's College
Dispensary, calls attention to a certain remarkable group of skin eruptions,
which he finds reported in the American journals, and with scarcely an exception
they related to cases where animal lymph was used. He first refers to instances
reported by Dr. Rice in the Chicago Medical Journal and Examiner for February,
1882, in which that gentleman states that " about one in ten of all vaccinated
have bad arms, with a high grade of fever, and eruption resembling somewhat that
of rotheln or German measles."
Further cases are given in the Boston Medical and Surgical Journal for 1882.
In the number for March
1 journal of Cutaneous and Venereal Diseases, vol. i., p. 167. March,
1883.
2 Glasgcno Medical Journal, June, 1883 (New Series), vol. xix., pp
424-432.
23, 1882, Dr. Alfred H. Holt1 records eruptions" in five successful primary
vaccinations with bovine lymph. The rash resembling German measles appeared
about nine days after vaccination, was attended with considerable fever, and,
when it faded, a brownish stain was left on the skin. Dr. Holt thought it was a
reasonable presumption that the eruption was due to vaccination, and remarks (p.
272)—" If such is the case, and this result is going to occasionally follow
vaccination with animal virus, it is highly important that the fact be known."
In the Journal for April 13, 1882 (p. 356), Mr. Vincent Bowditch recorded three
similar cases, the eruption appeared on the ninth day, and was succeeded by
brown staining of the skin as in Dr. Holt's cases. In one of the patients there
was considerable constitutional disturbance, fever, headache, and malaise, and
he remarks that other physicians in the town had similar cases.
Dr. A. I. Lawbaugh, in the issue for April 20, 1882 (p. 384), says that in eight
hundred of his own successful primary vaccinations with bovine lymph,
sixty-eight were attacked with a similar eruption, which was dusky red, covering
nearly the whole surface of the body. The eruption somewhat resembled measles;
and there was intense itching, and a brown stain was left which disappeared in
a few days. In thirteen successful primary vaccinations with humanised lymph,
one remove from heifer, three had eruptions; but there were no eruptions in two
hundred successful re-vaccinations. He remarks that his brother practitioners
have noticed similar experiences.
1 Boston Medical and Surgical Journal, March 23, 1882, vol. cvi., pp. 271, 272.
dr. napier's cases. 375
Dr. Morton Prince, in the number for April 27 (p. 394), observed that, as city
vaccinator, since the beginning of the year he had performed seven thousand
vaccinations, and that skin eruptions accompanying successful vaccination were
so frequently observed that he ceased to regard them as either unusual or
accidental. He describes papular and erythematous eruptions, the former being
so common as to " cease to attract notice." Dr. Prince furnishes notes of two
cases of urticaria with severe constitutional symtoms accompanying vaccination,
and one of very marked and widespread erythema. He adds (p. 395)—"Judging from
the number of times I have been questioned by anxious parents on the meaning of
these eruptions, I believe with Dr. Holt that the fact of their liability to
follow vaccination should be widely known."
Dr. Napier's own cases are as follows :—J
1. A healthy child vaccinated with calf lymph.
Normal course till tenth day, when a plentiful crop of
papules appeared on the lower limbs, lower part of
trunk, and arms. The eruption disappeared in three
days.
2. A child vaccinated with lymph taken from a
patient who had been vaccinated with calf lymph eight
days previously. Normal course till the eleventh day,
when large rings of erythema exudativum appeared on
arms and thighs ; on the following day the eruption
spread, and changed from a purplish to a yellowish red;
it faded on the third, and completely disappeared on the
1 See Glasgow Medical Journal, June, 1883 (New Series), vol. xix., pp. 426-428.
fourth day. The right hand and arm and left foot and ankle were much swollen and
deformed. No pain nor irritation ; fever slight. Two other children vaccinated
with the same lymph presented nothing abnormal.
3. A sister of the preceding. In this case calf lymph
used. Normal course till the tenth day, when a vivid
red, papular, measly eruption appeared over the whole
body, face, and head. Faded greatly in twenty-four
hours, and completely in two days.
4. Calf lymph vaccination. Normal course till the
ninth day, when eruption precisely resembling the last
case appeared. It faded by the evening of the next day.
5. A doubtful case, which Dr. Napier hesitated to
place in the same category, as the interval before erup
tion appeared was very long. Child was vaccinated
with human lymph. On the twenty-eighth day erup
tion exactly resembling that of measles appeared on
the scalp and face, and to a lesser extent on the neck,
chest, and upper arms ; it disappeared in five days.
There was no catarrh, and no other member of the
family was affected.
In summing up these experiences, Dr. Napier remarked (p. 430)—" In nearly every
instance I have mentioned in which spontaneous generalised eruptions followed
vaccination, the lymph used was animal lymph, not humanised lymph. What does
this indicate? That, as Dr. Cameron, M.P., once argued before this Society, the
nearer the virus to its original source in the days of Jenner, the stronger it
is, and the more efficient the protection it affords ? Without venturing to give
any opinion as to the greater efficacy of calf lymph vaccination as a
prophylactic against small-pox—a
OPINION OF DRS. ACLAND AND BARLOW. T,77
matter which can only be settled on the basis of a wide statistical inquiry—it
seems very clear that in animal lymph we have a more powerful material, one
which more deeply and obviously affects the system than our ordinary humanised
lymph, if the degree of constitutional disturbance is to be taken as an index of
the effectual working of the virus."x
More recently we find in an article on " Small-pox in San Francisco," by Dr. S.
S. Herrick, the following remarks :—" Besides the uncertainty of the bovine
virus, there are other features of common occurrence, which are not pleasant and
which are not found in the human product. The sores are apt to be quite serious
in character; a considerable eruption on the body is liable to take place ; and
the points of vaccination frequently develop a raspberry-like excrescence
(sometimes a true ecchymosis) which may remain for weeks, and is often mistaken
by the inexperienced for the normal result of vaccination."2
Apparently the experience of the profession in this country, as far as it goes,
is much the same as has been reported from America. Thus Drs. Acland and
Barlow,3 who investigated cases of vaccinal injury for the Royal Commission,
"are of opinion that a certain proportion of children will always suffer after
vaccination from various forms of cutaneous eruption. These seem to be more
frequent after vaccination with calf lymph, and
1 Glasgow Medical Journal (New Series), vol. xix., p. 430.
2 Tenth Biennial Report of the State Board of Health of California, 1888,
P- '39-
3 Royal Commission on Vaccination, Dissentient Commissioners' State
ment, section 186.
are for the most part free from danger, though often giving rise to considerable
distress." They also think that " calf lymph as now usually employed tends to
produce more severe inflammatory reaction than that which has been humanised."
Lastly, the Commissioners, although insisting that parents should have the
option of calf lymph for their children (section 437), apparently do not
recommend it with any degree of confidence ; for, a little above, on the same
page, they inform us that some of the best qualified witnesses have expressed a
deliberate preference for arm-to-arm vaccination, believing that the advantages
of calf lymph are more imaginary than real. A diminution, therefore, in the
mortality and in the amount of suffering can hardly be expected from this new
departure in the Jennerian cultus.
Glycerinated Lymph.
It has been frequently suggested that some of the most serious of the
unfortunate results arising from the use of animal vaccine might be prevented,
or at all events mitigated, by improvements in existing modes of its collection
and preservation; but, up to the present time, in no country, though much
ingenuity has been exercised, has a really safe variety been discovered.
A method, which has recently found favour in official quarters, and seems likely
to be adopted as far as public vaccination is concerned, consists in the
addition of glycerine to the lymph; it is hardly necessary to observe that this
would be an entirely new departure from the present system of public
vaccination, which is designed, as far as possible, to secure vaccination with
fresh lymph
GLYCERINATED CALF VACCINE LYMPH. 379
from arm to arm. The alleged advantages of the admixture with glycerine are,
that all micro-organisms, with the exception of the vaccine germ, are thereby
rendered inert and innocuous. Now, if it be true that glycerine has this very
extraordinary action, we may infer that lymph which has not been glycerinated
contains elements of danger. The promoters of glycerinated lymph, viz., the
Local Government Board, are to be congratulated on this somewhat tardy admission
of a danger which they have for years strenuously denied.1
This method of preservation appears to have been suggested in or about the year
1849,2 and it has been used extensively at one time or another, not only on the
continent of Europe, India, and Japan, but also in England.
Dr. Renner, the well-known purveyor of calf lymph, writes to the British Medical
Journal of October 30, 1897 (vol. ii., p. 1298)—"I have myself prepared and
supplied none but glycerinated calf vaccine ever since the year 1883 at my
establishment, except 'on points,' which, however, I have discontinued long ago,
and I have frequently demonstrated my procedure in all details privately and in
public;" and hence we have abundant means of testing whether glycerinated lymph
is so very innocuous after all.
In this connection the experience of the late Sir George Buchanan, Principal
Medical Officer to the Local Government Board, is of interest. It
will be
1 See "Facts concerning Vaccination for Heads of Families." (Revised
by the Local Government Board, and issued with their sanction.)
2 See Medical Times, vol. xxi., pp. 227, 248. March 23 and 30, 1850.
remembered that I have adverted to certain vaccinations in the Isle of Riigen
in 1885, where of seventy-nine children vaccinated, all but three were attacked
with impetigo contagiosa, and by infection the disease was spread to three
hundred and twenty out of a population of five thousand inhabitants. The Rugen
lymph was mixed with glycerine (glycerinum purissimum), and it has been
suggested by the late Sir George Buchanan1 that this was the cause of the
untoward occurrences. He handed round to the members of the Epidemiologi-cal
Society a plan showing the component parts of the " stuff" used by Dr. Ebert in
his Rugen vaccinations (p. 115). Sir George had " heard of dilutions of lymph
with glycerine, always from people complaining of the lymph" (p. 117). And he
concluded his remarks by observing—"It will, I trust, be long before such
preposterous adulterations of vaccine give the opportunity of investigating
their results in English practice" (p. 118).
It may be mentioned that the Chairman of the Royal Commission,2 Lord Hcrschell,
when this subject was under discussion, clearly indicated by his questions to my
father, when under examination, his opinion with regard to the danger of
adulterating lymph with glycerine. This will be seen by the following :—
Q. 9,804. (Chairman.) If there is a practice of mixing
the vaccine lymph with foreign
1 Transactions of the Epidemiological Society, 1885-86 (New Series), vol. v ,
pp. 114-118.
2The Royal Commission say (section 448)—"It was at one time suggested that the
introduction of glycerine was likely to be mischievous. The question is one a
further investigation of which is obviously desirable."
LORD HERSCHELL ON GLYCERINATED LYMPH. 381
matters, those foreign matters, if one of them is glycerine, may well be subject
to pollution ?—The intention is to improve the quality of the lymph—to render it
more innocuous.
Q. 9,805. But you may have the best of intentions in that direction, and you may
carry them out; but unless the individual who gets the lymph from the
Institution uses that lymph just as he gets it, mixing nothing with it, the best
of arrangements in the Central Institution will not prevent things going
wrong?—That is so.
Q. 9,810. . . . but, it is surely a point of importance whether it was a result
arising from the use of vaccine matter procured from a well-constituted
establishment, or whether it arose from the mixture of the vaccine matter with
something else by the practitioner who used it. You would admit that, I
suppose?—I see that clearly.
Dr. Liirman,1 of Bremen, gives an account of an epidemic of catarrhal jaundice
in 1883-84 in a large shipbulding and machine-making establishment in that town,
which is of interest from the fact that the patients had been revaccinated with
glycerinated lymph. One hundred and ninety-one persons were attacked. The
disease began with symptoms of gastric and intestinal catarrh, which persisted a
week or more, until jaundice
^-Berliner Klinische Wochenschrift, vol. xxii., pp. 20-23, January 12, 1885.
remembered that I have adverted to certain vaccinations in the Isle of Rugen in
1885, where of seventy-nine children vaccinated, all but three were attacked
with impetigo contagiosa, and by infection the disease was spread to three
hundred and twenty out of a population of five thousand inhabitants. The Rugen
lymph was mixed with glycerine (glycerinum purissimum), and it has been
suggested by the late Sir George Buchanan1 that this was the cause of the
untoward occurrences. He handed round to the members of the Epidemiologi-cal
Society a plan showing the component parts of the "stuff" used by Dr. Ebert in
his Rugen vaccinations (p. 115). Sir George had " heard of dilutions of lymph
with glycerine, always from people complaining of the lymph" (p. 117). And he
concluded his remarks by observing—"It will, I trust, be long before such
preposterous adulterations of vaccine give the opportunity of investigating
their results in English practice" (p. 118).
It may be mentioned that the Chairman of the Royal Commission,2 Lord Herschell,
when this subject was under discussion, clearly indicated by his questions to my
father, when under examination, his opinion with regard to the danger of
adulterating lymph with glycerine. This will be seen by the following :—
O. 9,804. (Chairman.) If there is a practice of mixing
the vaccine lymph with foreign
1 Transactions of the Epidemiological Society, 1885-86 (New Series), vol. v.,
pp. 114-118.
2The Royal Commission say (section 44S)—"It was at one time suggested that the
introduction of glycerine was likely to be mischievous. The question is one a
further investigation of which is obviously desirable."
LORD HERSCHELL ON GLYCERINATED LYMPH. 381
matters, those foreign matters, if one of them is glycerine, may well be subject
to pollution ?—The intention is to improve the quality of the lymph—to render it
more innocuous.
Q. 9,805. But you may have the best of intentions in that direction, and you may
carry them out; but unless the individual who gets the lymph from the
Institution uses that lymph just as he gets it, mixing nothing with it, the best
of arrangements in the Central Institution will not prevent things going
wrong?—That is so.
Q. 9,810. . . . but, it is surely a point of importance whether it was a result
arising from the use of vaccine matter procured from a well-constituted
establishment, or whether it arose from the mixture of the vaccine matter with
something else by the practitioner who used it. You would admit that, I suppose
?—I see that clearly.
Dr. Liirman,1 of Bremen, gives an account of an epidemic of catarrhal jaundice
in 1883-84 in a large shipbulding and machine-making establishment in that town,
which is of interest from the fact that the patients had been revaccinated with
glycerinated lymph. One hundred and ninety-one persons were attacked. The
disease began with symptoms of gastric and intestinal catarrh, which persisted a
week or more, until jaundice
1 Berliner Klinische IVochensckrift, vol. xxii., pp. 20-23, January 12, 1S85.
appeared. The symptoms comprised epigastric oppression, anorexia, vomiting,
faintness, and there was usually constipation. Yellow vision occurred in a few
instances. In one case the patient suffered from general dropsy with cerebral
symptoms, but none of the cases were fatal. Eighty-seven persons in the
establishment, who were revaccinated by other surgeons and other lymph, remained
unaffected. Dr. Edwardes, who relates these cases in the London Medical Record
of April 15, 1885 (vol. xiii., p. 142), remarks that the epidemic "was causally
connected with the re-vaccination, in some way or other."
A feature of glycerinated lymph appears to be that, when it takes, great
intensity of action is observed, both local and general. Thus Dr. James Cantlie1
refers to "much constitutional disturbance" produced by Japanese lymph. I may
also allude to an article by Dr. Robert J. Carter.2 He details the results of
319 re-vaccinations with glycerinated calf lymph. He observes that in 106 of the
patients the axillary glands were " large, hard, and tender, and in some
instances exquisitely painful;" in 3 of the cases the glands above the
collar-bone were also affected. In 9 cases lymphangitis was present, the
lymphatic vessels being felt as hard, swollen, tender cords along the course of
the axillary vessels. In 98 of the patients there was oedema and induration of
the arm, and these manifestations were of a " curiously persistent character."
Dr. Carter remarked that they were apparently dependent on the intensity of the
local inflammation at the site of the vaccination.
''-British Medical Journal, October 5, 1889, vol. ii., p. 762. 2 The Lancet,
June 12, 1897, vol. i., pp. 1611, 1612.
GLYCERINATED LYMPH IN INDIA. 383
Abundant evidence of the danger of glycerinated lymph is adduced in Appendix ix.
to the Final Report of the Royal Commission. The cases are, of course, mostly
erysipelas or of a septic nature ; and, without including those of a less severe
character, they number 84, and of these no less than 24 were fatal.1
In India glycerinated lymph has been a failure in every way. In the first place,
the success per centum has been very low, as will be seen from the following
figures2 for Madras Presidency in 1894-95 :—
"*°* '^h- vaSafJd. parent.
Direct from calf ... ... ... 378,955 97'4
Preserved in glass tubes or plates 142,899 94^1
Preserved with glycerine ... ... 642,296 89^2
In 1895-96 the results are much the same :—8
Animal lymph. ^-^ Ł^
Direct from calf .................................... 300,518 97-8
Preserved in tubes ... ... ... 98,703 951
Preserved with glycerine ... ... 641,181 89^5
Preserved with lanoline ................ 23>i93 94 5
This low percentage of successful results is naturally regarded as a very
serious objection. In the Memorandum by the Army Sanitary Commission on the
Report of the Sanitary Commissioner of Madras for 1894, it is stated:—" In the
Madras Presidency, preserved lymph is largely used. No fewer than 642,296
persons were vaccinated with lymph preserved with glycerine. It is, we think, no
matter of surprise that of these only
1 See Nos. liii., lxxxii., xcix., cviii., cxii., cxxvii., cxxviii.,
cxxxiv.,
cxliv., cxlviii., cl., clxxxi., clxxxix., 21, 81, 122, 168, 207, 208, 21S, 221,
236, 237, 244, 249, 251, 258, 312.
2 Report on Sanitary Measures in India in 1894-95, p. 113.
3Ibid., 1895-1896, p. 102.
8c/2 per cent, proved successful cases of vaccination This messing with
vaccine lymph mixed with glycerine is evidently not only an expensive procedure,
but disappointing in its results. Altogether, vaccination in the Madras
Presidency seems to us to be capable of improvement."1
It appears that the results have been so unsatisfactory generally, that the
preparation of glycerinated lymph, after a fair trial, has been entirely
discontinued in the Calcutta and Darjeeling Depots, the principal reason
assigned by the Sanitary Commissioner for Bengal being that '' Glycerine is a
nutritive medium for the growth of putrefactive and other germs, and, being
fluid, the germs soon pervade it throughout; and, as a fact, this preparation
(glycerinated lymph) in India soon becomes putrid and septically dangerous."2
And when we consider the stimulating action of glycerine on the growth of the
tubercle bacillus, it seems probable that a general introduction of glycerinated
calf lymph would add a new and important risk to the practice of vaccination.
It appears, therefore, certain that by none of the methods at present in vogue
can we lessen the danger and amount of suffering attending the practice; and
when the alleged prophylaxy of vaccination is allowed to be so ephemeral by some
of its ablest defenders, the State may surely, as in the case of other medical
prescriptions, leave the matter to the parent, who, after all, is the most
concerned, to say whether his child shall be vaccinated or not.
1 Report on Sanitary Measures in India in 1894-95, P- 217-
2 Indian Lancet, March 1, 1897, vol. ix., p. 221.
CHAPTER X.
SUMMARY AND CONCLUSIONS.
BEFORE summing up my conclusions, a few words concerning the enforcement of
vaccination may not be out of place, and my task has been simplified by the
Report of the Royal Commission. Four of the Commissioners have recommended that
compulsion should be altogether abolished, and the remaining nine, that honest
objectors should not be subject to fine or imprisonment for refusal to allow the
vaccination of those for whom they are responsible. Those who have studied the
evidence given before this important tribunal, and especially the Blue Book1 of
453 folio pages containing the records of vaccinal disasters, will concur in
according to the Commissioners their appreciation of these wise and humane
recommendations.
The following are the points emphasised in my chapter on this serious aspect of
the question :—
1. That the principle and practice of vaccination involves the introduction of a
specific disease at least twice, and, according to numerous authorities,
many
1 "Papers relating to cases in which death or non-fatal injury was alleged or
suggested to have been caused by, or otherwise connected with, vaccination. "
Appendix ix. to the Final Report of the Royal Commission on Vaccination.
times into the human organism; that this specific disease causes an undeniable
impairment of health and vitality, it being a distinctly morbid process.
2. That the operation of vaccination may occasion a
definite risk to life, one death on an average being
officially registered from this cause every week in
England and Wales.
3. That there is good reason to believe that this
record greatly underestimates the fatalities and injuries
directly resulting from the operation.
4. That no lymph, whether human or animal, or
adulterated with other substances, can be guaranteed as
free from danger.
5. That there is unimpeachable evidence proving that
a variety of inoculable and some incurable diseases are
induced by vaccination.
6. That there is no guarantee that syphilis, or sym
ptoms undistinguishable from this malady, may not be
induced by the inoculation of either human or animal
virus. One of the greatest of our physicians, the late
Sir Thomas Watson, in referring to the risk of vaccino-
syphilis, says:—"I can readily sympathise with, and
even applaud, a father who, with the presumed dread
or misgiving in his mind, is willing to submit to multi
plied judicial penalties rather than expose his child to
the risk of an infection so ghastly." 1
This outspoken deliverance was written twenty years ago, when very few medical
men had ventured to question the justice of compulsion, and is the more
valuable,
1 The Nineteenth Century, June, 1878, vol. iii., p. 1006.
COMPULSORY VACCINATION. . 387
inasmuch as Sir Thomas Watson was a firm believer in the efficacy of
vaccination.
Once admitted that the risk is real, and one which no amount of care can guard
against (even if vaccination were a preventive of small-pox), all ground for
compulsion vanishes; for it then becomes a question of parental or individual
responsibility, as in the case of any other operation or treatment involving
risk to life and health. No surgeon would dream of administering chloroform or
of performing the most trivial operation without first obtaining the patient's
consent; and, therefore, no authority, whether medical or State, has the right
to attempt to over-ride a parent's or patient's scruples. The matter should thus
be left to the option and good sense of the individual, as in the case of other
medical prescriptions. Compulsory vaccination is now even by medical men
beginning to be recognised as a grievous and mischievous mistake, and I have not
the slightest doubt that the profession would willingly relinquish it
to-morrow, if their credit and prestige were not so deeply involved. It seems,
therefore, that the agitation for the repeal of the Vaccination Acts must of
necessity come, as it always has done, from the people themselves. Parliament,
confessing its own incompetency, and relying on medical promises which have been
falsified all along the line of a century's experience, has decreed that
vaccination should be obligatory. Parliament must, therefore, be persuaded to
undo the evil it has unwittingly committed. Unfortunately, the dead cannot be
recalled to life, nor can the parents of those who have been injured by the
operation be compensated ; nor will the scandalous
and unrelenting persecution of upright and otherwise law-abiding citizens, whose
only offence has been a determination to preserve their children's bodies from
the risk of inoculated disease, be easily condoned.
The cruel hardship of qualified persons deprived of employment in the public
service by reason of their refusal to submit to vaccination and re-vaccination
calls for prompt redress. This injustice is acutely felt in the case of pupil
teachers in the public elementary schools; and the penalty for non-compliance is
immeasurably greater than the payment of a fine and costs. As the
Commissioners, after seven years' inquiry, have recommended that all parents
who conscientiously object to vaccination shall no longer be subject to penalty,
it is manifest that the refusal of employment in the public service to these
conscientious nonconformists cannot be logically or fairly defended.
Pending the repeal of the Vaccination Acts, our legislators are in the
responsible position of being a party to the enforcement of a surgical
operation, proved by the Royal Commission to be attended with danger, on every
child born in this kingdom ; a compulsion, it may be added, about the expediency
of which the people of this country have never had an opportunity of passing an
opinion. In the meantime death-certificates of children killed by vaccination
are accumulating at Somerset House, and most of these are doubtless a direct
consequence of this law.
The more hotly-disputed question of the value of vaccination itself has been
considered in the foregoing pages at some length, and it only remains to briefly
summarise the various points.
THE VARIOLOUS TEST. 389
In the early days of vaccination, before it could be put to the test of
experience, it appears to have been felt that the inoculation test would furnish
absolute proof of the protection afforded by the practice against small-pox. In
the first chapter of this volume it has been shown that the lymph which
convinced the profession of the efficacy of vaccination was Woodville's
"hospital matter," which was unquestionably contaminated with small-pox—hence
the immunity which it is claimed resulted from its use may have been an immunity
produced by small-pox, which therefore proved nothing in favour of vaccination.
The few variolous tests which were performed by Jenner himself have been shown
to be inconclusive; and it is significant that Jenner very early discarded the
test in favour of that of re-vaccination.
From the earliest days of vaccination numbers of cases have been recorded of
every description of smallpox following vaccination, from the mildest to the
most severe and fatal, and within the shortest periods of the operation. In the
absence of any reliable method of estimating the proportion of the population
vaccinated, it is impossible to compare the relative attack-incidence of
small-pox in the two classes ; but it is important to note that the proportion
of vaccinated cases in well-vaccinated districts has ranged as high as 95, 98,
or even 100 per cent. A method of comparison free from objection is the
attack-incidence of small-pox in different towns. Gloucester in 1895-96 had an
attack-rate of 48 per 1,000, or about the same as that for the well-vaccinated
town of Willenhall in 1894, and the
unvaccinated towns of Keighley and Leicester in the recent epidemics had only
rates of 2'2 and ro, per 1,000 respectively.
With regard to the death-incidence, we may compare the death-rates of small-pox
at different periods in the history of vaccination, or in different towns ; or
we may split up the cases of small-pox into two classes, vaccinated and
unvaccinated, and compare the case-mortality in each class. In the chapter on
mitigation, I have dwelt at some length on the objections to the latter method
of procedure ; and in my judgment they are so vital that the evidence under this
heading, in attempting to arrive at a decision as to the value of vaccination,
must be set on one side.
There remains to consider the death-rates from smallpox at different times and
places; and, as the protection is admittedly only of a temporary nature, to take
into account the proportion of the mortality borne by children. I have shown
that the small-pox mortality began to decline about 1781, long before the
introduction of vaccination; and it was accompanied by a decline in fever and
in deaths from all causes, and was due to the development of sanitary
improvements. The decline continued after the introduction of vaccination, and
it is almost certain that part of this reduction was due to the cessation of
small-pox inoculation.1
Since the commencement of registration, the facts laid before the reader show
that smali-pox has paid no
1 The inoculation of out-patients at the London Small-pox Hospital was
discontinued in 1808. Baron's " Life of Jenner," vol. ii., p. 238.
THE DECLINE IN SMALL-POX. 391
heed to vaccination at all, one of the worst epidemics of the century taking
place after seventeen years of compulsion ; and quite recently, especially in
London, as appears by the figures cited, we have a remarkable decline of
small-pox coincident with diminishing vaccination. Neither does vaccination
seem to have had any effect on the severity of the disease; the case-mortality
being as high in 1871-72, with a large percentage of the cases of small-pox
vaccinated, as it was in the last century, before Jenner's discovery. Hence up
to the time of this epidemic the diminution of pock-marked faces, as far as any
diminution had been observed, cannot have been due to any diminished severity
of the disease, but must be attributed rather to a decline in the prevalence of
small-pox itself. Since 1871-72, however, there has been a great decline in the
severity of the disease, which has, doubtless, resulted from improved hygiene
and altered methods of treatment. It may also be noted that since the last
century, typhus which is spread in much the same manner, has shown a greater
reduction than small-pox, and is now an almost extinct disease.
The death-incidence of small-pox in different towns is another method of
comparison not open to objection. Gloucester heads the list of recent epidemics,
with a death-rate of over ten thousand per million; but it has been shown that
in a list of twenty-four well-vaccinated towns the death-rates have varied from
six thousand to nearly ten thousand per million, and hence the figure for
Gloucester is deprived of much of its significance. That unvaccinated towns can
be kept comparatively free from small-pox is conclusively proved by the ex-
perience of Keighley and Leicester, which had only rates of two hundred and
eighteen and one hundred and fourteen per million respectively, in the recent
epidemics; and that the most complete vaccination of a district possible will
not prevent a serious epidemic, is shown in the case of Mold, which, in spite of
the vaccination of every child born and remaining in the district for eighteen
years previous to the epidemic, had a small-pox death-rate of 3,614 per million,
in 1871-72.
The last argument urged in the defence of vaccination is the change in
age-incidence. That this is not brought about entirely, or even principally, by
vaccination, is clear, from the fact that a similar change has occurred in the
unvaccinated, and therefore independently of vaccination.
Another important matter to which attention has been directed is that, since the
commencement of registration, the greatest decline in the infantile share of
small-pox deaths took place about 1871-72, and was not associated with a very
large increase in the amount of public infantile vaccination ; whereas the
greatest increase in public infantile vaccination was in the years following the
compulsory Act of 1853, and this was accompanied by quite a trifling reduction
in the infantile proportion of the small-pox mortality.
The Commissioners appear to attach considerable importance to a comparison they
make of the children's share of small-pox deaths in certain vaccinated and
unvaccinated towns. Thus they show for recent epidemics that at Leicester and
Gloucester the proportion of children's deaths from small-pox under ten years of
age was much larger than in the well-vaccinated towns
MR. ALEXANDER PAUL ON AGE-INCIDENCE. 393
of Sheffield and Warrington. In my second chapter I ventured to criticise these
figures on the ground that the experience was not sufficiently extensive, and I
showed that England and Wales in 1871-72, with only 5 per cent, vaccination
default, had almost as large a proportion of small-pox deaths under ten years of
age as there were at Dewsbury in 1891-92 with a default of j,1/ per cent., and I
also pointed out that Mold and Willenhall,1 both extremely well-vaccinated towns
at the time of their respective epidemics, had a large percentage of their
small-pox deaths under five years of age, and I instanced the epidemic in the
unvaccinated town of Keighley, with seven small-pox deaths all over five years
of age.
Since writing my second chapter I have had the advantage of consulting an
important contribution to the age-incidence controversy by Mr. Alexander Paul.2
He points out from the Commissioners' own figures that the children's
percentages of small-pox deaths in the towns specified only show similar
variations to their
1 In a foot-note on page 53 the age-incidence of fatal small-pox at Leicester is
compared with that of Mold and Willenhall, the proportion of fatal cases under
five years of age at Leicester being given at 36'8 per cent. From Dr. Coupland's
report I gather that this figure is incorrect, and that if the deaths of those
children who suffered from the proximity of the scarlet fever ward to the
hospital in which small-pox cases were treated be left out of the calculation,
41 '2 per cent, of the total deaths from smallpox at Leicester were under five
years of age, which is rather higher than the figures for Mold and Willenhall
(34 per cent.).
3 "A Royal Commission's Arithmetic: A Criticism of Vaccination Statistics, and a
Plea for Fresh Figures and Fair Inferences." Alexander Paul. London. 1897.
percentages of small-pox illness ; whereas, according to the theories of the
Commissioners, the variations should be far greater, for they think that the
power of vaccination to modify the character of small-pox is greatest during
the years immediately succeeding the operation. The following are the figures1
for the attacks and deaths placed side by side :—
Children, aged o-io.
Percentage borne Percentage borne
~ . i . by them of by
them of
Epidemics ^ small_pox total smau.pox
illness. deaths.
Warrington, 1892-93 9"83 22"58
Sheffield, 1887-88 ... 12-42 25-60
London, 1892-93 ... 15-21 36-82
Dewsbury, 1891-92... 21-64 51-82
Gloucester, 1895-96... 35-67 64-52
Leicester, 1892-93 ... 30-53 71-43 (or 66"6o)
Of course the question will be raised, that, granted the deaths only follow in
the same proportion as the attacks, that is to say, that no extra penalty must
be paid in the shape of death for neglecting vaccination, this will not account
for the varying proportions of the children's share of small-pox illness in the
different towns, which ranged from 9-83 per cent, at Warrington to 35-67 per
cent, at Gloucester.
Mr. Paul explains this—and I think the explanation is a reasonable one—by the
varying incidence of smallpox attack on adults and children in the several
towns.
1 The figures for the deaths are those given hy the Commissioners, those for
small-pox illness being calculated from the Final Report of the Royal Commission
by Mr. Paul.
AGE-INCIDENCE OF VACCINATED SMALL-POX. 395
Thus, at Warrington, small-pox was mainly spread in the forges near the hospital
; at Gloucester an important factor was the introduction of the disease into the
public elementary schools; and at Leicester the proximity of the scarlet fever
wards to the hospital where small-pox cases were treated undoubtedly raised the
children's share of small-pox illness.
The vaccination hypothesis I believe to be untenable, both for reasons given by
Mr. Paul and also because it does not fit in with the experience of the early
observers on the relation of small-pox to vaccination. If there is anything at
all in the theory that in a vaccinated population the children's share of
smallpox illness will be low, and vice versa, it will be admitted that in an
extreme case—i.e., where all the patients suffering from small-pox have been
vaccinated—the children's share of illness should be very low, indeed lower than
the 9^83 per cent, at Warrington ; this is entirely at variance with the
experience of vaccinated small-pox in the early days, before the age-incidence
of small-pox had commenced to change. Indeed, the large proportion of young or
recently-vaccinated cases led Mr. Edward Greenhow and others to suspect that
cow-pox was wholly, or in part, losing its virtue ; for he found that the
numbers attacked were in the inverse ratio to the number of years which had
elapsed since they were vaccinated. One of Dr. Thomson's correspondents, Mr.
William Gibson, gives figures for the epidemic at New Lanark (see p. 152), where
of 251 vaccinated cases of small-pox, 191 or 76-1 per cent, took the disease at
intervals, up to ten years
after vaccination. This high percentage is what we should naturally expect at a
period before the age-incidence of small-pox had commenced to change. The only
escape I can see for the supporters of vaccination, is to say that all the early
operations were ineffectual, which is a dangerous argument for those who urge
that the decline of small-pox was due to this prophylactic.
This matter of the varying age-incidence of smallpox in the different towns has
been dwelt on so fully because much has been made of it by the Commissioners,
but there are other points connected with the subject which have been carefully
worked out by Mr. M ilnes, and tend to show that the only other diseases at all
comparable with small-pox have shown a similar change in their age-incidence,
and that it is sanitation to a large extent which must be held accountable,
although, for reasons given in my third chapter, another cause has doubtless
been at work—that is to say, a shifting of the small-pox mortality on to other
diseases, such as measles and whooping-cough, which would thus explain the
insignificant reduction which has taken place in the mortality from these
complaints.
It may be asked at this juncture, how it is, with the same set of facts before
me, I have arrived at a different conclusion to the Commissioners. My readers
may perhaps be able to judge for themselves if I put before them the facts which
influenced this body to their somewhat halting opinions. The essence of the case
which convinced the Commissioners of the efficacy of vaccination was given by
their Chairman, Lord Her-schell, at a meeting held on March 31, 1897, for the
LORD HERSCHELL ON VACCINATION. 397
purpose of raising a fund for a national memorial to Edward Jenner.1
After a few preliminary remarks on the terrors of small-pox in the last century,
and its decline after the introduction of vaccination, Lord Herschell introduces
the statistical case for vaccination, and he deals with three points—the first
being the varying age-incidence of small-pox in the six towns, the second the
fatality of the vaccinated and of the unvaccinated in these towns, and the third
point being an examination into the behaviour of small-pox before and since
vaccination was made compulsory. The first two matters have been dealt with so
fully in this volume that I think it is hardly necessary to say anything
further. With regard to the third point, I will state the case in Lord
Herschell's own words. " I am going to invite your attention," he says, " to the
figures with reference to the effects of the introduction of compulsory
vaccination into this country. It is undoubtedly recognised now that the
protection of vaccination is not permanent. It operates most effectually during
the earlier years rather than the later after the operation has been performed,
and it is probably during the first nine or ten years after vaccination that
its operation is most efficient. Bearing that in mind, let me invite your
attention to this, that in the years from 1848 to 1854—that is, before the
introduction of compulsory vaccination—the deaths of children under five years
of age were 1,514 to every million persons living, and that from 1885 to 1894
they were 50 to every
1 For full report of speech see British Medical Journal, May 15, 1897, vol. i..
pp. 1247, 1248.
million persons living. Now take the other end of the scale—45 years and
upwards. Of course, those of that age would be no more affected by compulsory
vaccination between 1885 and 1894—the law having been passed in 1853—than
children would be in the year prior to its introduction. In that class the
deaths only fell from 24. per million to 19."
These figures have been taken from page 48 of the Final Report of the Royal
Commission, and the following table also gives the figures for the intervening
year periods :—■
Deaths from small-pox per million living.
Years. Under 5. 45 and upwards.
1848-54 ....... 1,514 ... 24-0
1855-64 788-8 ... 36-2
1865-74 782-5 ... 87-5
187584 ....................... I27"8 ... 33-9
1885-94 ... ... ... 50-2 ... 19-0
I do not gather that Lord Herschell wishes to found any argument from the latter
part of his statement with reference to the reduction in the adult mortality
from 24 to 19 per million ; but it may be noted that prior to the decline there
was a large increase in the adult mortality, which has led Dr. Bridges to doubt
if vaccination ever would have been made compulsory if these results had been
anticipated. The point, no doubt, to which Lord Herschell wishes to draw
attention is the decline in the children's mortality from 1,514 to 50-2 per
million. It will be observed that Lord Herschell omits to state that there has
also been a large decline in fever during the period under review, nor does he
hint that there may be a cause other than vaccination which would act more
powerfully in children than in adults—
LORD HERSCHELL ON VACCINATION. 399
viz., sanitation—to account for the reduction in the mortality from
small-pox.
Let us now examine the facts Lord Herschell has presented. In the first place,
exception must be taken to the statement that the years from 1848 to 1854 are
before the introduction of compulsory vaccination, for during the year 1854 the
public vaccinations in this country reached a higher figure than they have ever
touched in any year before or since, owing to the Act of 1853 ; secondly, it is
unfair to put forward the period 1885-1894 as if it were a period during which
the vaccination of children had been completely carried out, for, as I have
shown, there has been a large reduction in the infantile vaccinations as
compared with the period 1875-84, and Lord Herschell's own figures show that
coincident with this reduction there has been a decline of 61 per cent, in the
children's small-pox mortality. This decline he has placed to the credit of the
prophylactic he is defending, and then he says he is " surprised " at the force
of the evidence adduced in favour of vaccination.
Although there does not appear to be trustworthy evidence to show that
vaccination possesses any influence over the prevalence or mortality of
small-pox, it is unfortunate that a too implicit belief in its efficacy has
given rise to the pernicious doctrine that sanitary measures are of no avail in
preventing this disease. We can quite understand that the owners of filthy
rookeries and other insanitary premises are only too ready in their own
interests to welcome such a theory, but for a great profession to have become
wedded to the doctrine has, I believe, greatly impeded the progress
of sanitary reform; for while outbreaks of other diseases, such as typhus,
typhoid, cholera, and scarlet fever, have proved valuable object lessons for
municipal sanitary amelioration, each epidemic of small-pox appears to have
taught the profession little or nothing but the necessity of repeated
vaccinations.
It is true that there have been occasional gleams of light from the more
independent thinkers in the medical and lay press, but these have been unequal
to direct public authorities towards the only remedial and scientific
preventive—-personal and municipal sanitation.
Those who have followed the facts presented in this volume concerning the
insanitary condition of London in previous centuries can have come to no other
conclusion than that this was the chief cause of the large small-pox and typhus
death-rates. What else could be expected with the narrow streets, courts, and
alleys ; the imperfectly-constructed houses with little or no curtilage; the
almost total absence of external ventilation, the exclusion of light and air by
the operation of the window tax, the dense overcrowding, the almost constant
inhaling of putrid excrement, the loathsome effluvia from the intramural
burial-grounds, the limited water supply—these, added to the filthy personal and
domestic hygiene, cannot have failed to have influenced the spread and mortality
from these diseases. Neither is it to be wondered at that the insanitary state
of the prisons, as described by Howard, favoured the spread of small-pox and
typhus to the " destruction of multitudes." Much the same state of things
prevails in parts of Egypt, China, and India of to-day, and it is these
districts where insanitary conditions are rife which
SMALL-POX AND SANITATION. 4OI
demonstrate the utter futility of vaccination to cope with epidemic small-pox.
In the Report on Sanitary Measures in India in 1879-1880, p. 142, it is
stated:—"The vaccination returns throughout India show the same fact, that the
number of vaccinations does not necessarily bear a ratio to the small-pox
deaths. Small-pox in India is related to season, and also to epidemic
prevalence; it is not a disease, therefore, that can be controlled by
vaccination, in the sense that vaccination is a specific against it. As an
endemic and epidemic disease, it must be dealt with by sanitary measures, and if
these are neglected small-pox is certain to increase during -epidemic times."
Again, in the Memorandum of the Army Sanitary Commission on the Report of the
Sanitary Commissioner for the Punjab, for 18?g, we read that " Vaccination in ■
the Punjab, as elsewhere in India, has no power apparently over the course of
an epidemic. It may modify it and diminish the number of fatal cases, but the
whole Indian experience points in one direction, and this is that the severity
of a small-pox epidemic is more closely connected with sanitary defects, which
intensify the activity of other epidemic diseases, than is usually imagined, and
that to the general sanitary improvement of towns and villages must we look for
the mitigation of small-pox as of cholera and fever."1
Thus it is on sanitation that we must henceforward rely for the prevention and
extermination of epidemic diseases. The most necessary measures for the
prevention of small-pox must therefore include—
1 Report on Sanitary Measures in India in 1879-80, p. 186.
(1) Demolition of dwellings unfit for human habita
tion.
(2) Construction of houses to secure adequate external
and internal ventilation, and the prompt removal of all
filth accumulations from the premises.
(3) Adequate water supply and efficient sewerage
systems.
(4) Provision of open spaces in towns.
Another wise method of prevention has been revived in recent years, and this is
the separation of the sick from the healthy. This system is mentioned in the
writings of Rast, Haygarth, and Faust, in the last century, and was tried
experimentally at Chester ; but the advent of vaccination, with the confident
promises made on its behalf, put a stop to further development of isolation at
that time. Attention was again drawn to the subject in 1868, by Sir James
Simpson, in a paper entitled " Proposal to Stamp out Small-pox and other
Contagious Diseases ;" and it was shortly afterwards put to a practical test.
Where it has been tried, coupled with sanitation, as at Leicester and in the
county of London, it has been pre-eminently successful in reducing the small-pox
mortality. At the present time, compulsory vaccination, by paralysing efforts
in other directions, blocks the way towards sanitary reform. When the laws are
abrogated vaccination must, like all other medical prescriptions and surgical
operations, rest upon its own merits, or, in other words, on its inherent
persuasiveness, unaided by the arm of the law. The practice will then, in my
opinion, in the not very distant future be surely abandoned.
This will prepare the way for a new era of improved
TRADITION OF THE DAIRYMAIDS. 403
health and human happiness, the result of scientific sanitary amelioration in
all departments of our social domestic, and municipal life.
In due course of time the tradition of the dairymaids of Gloucestershire will
take its proper place among the legends and folk-lore of the past; and, if
allowed to prophesy, I cannot help thinking that another generation will look
back with amazement and incredulity that for a hundred years the people of these
islands should have worshipped at the shrine of a strange, unreasonable, and
mischievous superstition.
APPENDIX
FATALITY OF SMALL-POX, 1721-30.!
Locality of the Epidemic.
Period.
Authority. Cases. Deaths. | Percentage of
ir clttHltlCSf
Halifax........................................................................
Winter of 1721 to Nettleton. Phil.
Trans., 276
43 15-9
April, 1722 j vol. xxxii., p. 51
Rochdale....................................................................
Winter of 1721 to j
Ibid. 177 38 21-4
April, 1722 !
Leeds..........................................................................
Winter of 1721 to I
Ibid. Jgz 189 23-8
April,
1722
j
Halifax parish, towards Bradford -
1772 Ibid., p.
221 297 i 59 19^9
Halifax parish, another part- - -
1722 Ibid., p.
221 268 28 io'4
Bradford.....................................................................
1722 j Ibid., p.
221 129 36 27-9
Wakefield..................................................................
1722 Ibid., p.
221 418 57 13-6
Ashton-under-Lyne -
1722 Ibid., p.
221 279 56 2O'o
Macclesfield ----- 1722
Ibid., p. 221 302
37 i2'2
Stockport...................................................................
1722 Ibid., p.
221 287 73
25-4
i Hatherfield.................................................................
1722 j Ibid., p.
221 180 20 ii-i
Chichester................................................................. 1722
(to Oct. 15) [ Whitaker. Ibid., p.
223 994 168
16-9
j Haverfordwest...........................................................
1722 Perrot Williams.
Ibid. 227 52 22-9
Barstand, Ripponden, Sorby, and part of Halifax parish, four miles from
I the town -----
1722 Nettleton.
Turin's 230 38 16'5
"Account" for 1723, p. 7
Bolton.........................................................................
1723 (?) Jurin's " Account" for
406 89 21-6
I
1723, p. 8
Ware............................................................................
1723 (?)
Ibid. 612
72 117
Salisbury....................................................................
1723 (?)
Ibid. 1,244
165 I3'2
Rumsey, Hants - - - - 1723
(?)
Ibid. 913
143 15-6
Havant ......
17231?)
Ibid. 264
61 23-1
Bedford - - - - - - | 1723
(?) Turin's "Account"
m , 7S6 147 j iS'4 I
i
'
" 1723, p. 8 :
I Shaftesbury - - - - - j 1724
(?) Ibid, for
1724, p. 12 660 roo I 15'i
j Dedham, near Colchester - - - 1724
(?)
Ibid. 339 106 31'3
^3
Plymouth....................................................................
1724 (?) '
Ibid. j 188 32 ! 17'2
Aynho. near Banbury - - - , September
27,1723, Kev. Mr. Wassc,
rector. 133 25 , l8'8
to Dec. 29,
1724 Ibid,
for 1725, p. 55 !
Stratford-on-Avon - ■- - - | September
27,1723, Dr. Letherland.
Ibid. 562 89 15'8
j to Dec. 29, 1724
Bolton-le-Moors ....
September27,i723, Dr. Dixon.
Ibid. 341 : 64 ! t8'8
to Dec. 29, 1724
Cobbani ------ September27,1723, Sir Hans
Sloane Ibid. 105 20 I9'o
to Dec. 29, 1724 j
Dover ..--.- September29,1725, i Dr.
Lynch, of Canter- 503 61 j I2T
to Dec. 25, 1726
j bury, in
Jurin's "Ac i
j count" for 1726, p.
17 ; 1
Deal ------- December 25, 1725,
j Ibid. !
362 33 91
to Nov. 29, 1726
,
1
Kempsey, near Worcester - - December 25,
1725, Dr. Beard, injurin
Ibid. 73 15 20'5
to Nov. 29, 1726
Uxbridge ------ 1727
Dr. Thorold, in Scheuch- 140 : 51 36'4
zer's "Account" for i 1727 and 1728
Hastings ------ 1729-30 Dr. Frewen. Phil. Trans.,
705 97 137
vol. xxxvii., p 108 ;
r I_______ '__________
1 13,192 2,264 ' >7'2
_____________________________________________ ;__________________________
'________ I_____
1 "A History of Epidemics in Britain," vol. ii,, pp. 518-519. Creighton.
1894.
EGYPT.
The average annual strength of the British army in Egypt, with
the number of admissions and deaths from small-pox for the four
teen years 1882-93 :—
Small-pox.
Strength. Admissions. Deaths.
1882 ... ... ... 6,198
3 o
1883
7,897 8 3
1884
6,468 25 I
1885
9,593 52 4
1886 ............................... II,o62
51 3
. 1887 .................................
5,272 26 4
1888
3,346 I4 4
1889
3,431 42 6
1890 ... ... ...
3,209 o o
1891 ... ... ...
3,172 I 6
1892 .............................. 3>I°2
2 O
1893 ............................ 5,°73
4 °
1894 ... ... ...
5,226 o o
1895 ■■• ' ..................
4,5°4 5 o
INDIA.
The average annual strength of the British army in India, with
the number of admissions and deaths from small-pox for the four
teen years, 1882-95:—
Small-pox.
Strength. Admissions. Deaths.
1882
57,344 44 4
1883
56,190 105 9
1884
55,252 77 8
1885
57,i65 12 o
1886 ................ 6i,757 22 1
1887 ... ... ... 63,942 40 2
1888
68,795 i°6 10
1889
68,545 152 17
1890 67,456
36 4
1891
66,178 14 1
1892
68,045 18 3
1893
69,865 33 4
1894
70,983 '3 3
1895 .................. 68>35' '9 2
LEICESTER.
The population of Leicester with attacks and deaths from smallpox for the
fourteen years 1882-Q5 x:—
Small-pox.
Population. Attacks. Deaths.
1882 ... 126,275 29(25) 5
1883 129,483
12(9) 3
1884 ... 132,773 6(3) o
1885 ... 136,147
8 o
1886 ... 139,606 1 o
1887 143,153
10(9) o
1888 ... ... ... 146,790
22(21) o
1889 ... ... ... 150,520 o
o
1890
154-344 o °
1891
177,353 ° °
1892 .„ ........... 180,066 38 6
1893
184 547 308 15
1894
189,136 8 o
1895
193,839 4 °
1 Up to the year 1889 the figures have been taken from Diagram D facing p. 435,
Fourth Report, Royal Commission on Vaccination. In several instances the number
of attacks is in excess of those given by the Medical Officer of Health in his
report on the Leicester small-pox epidemic, 1892-93. Dr. Priestley's figures,
where they differ, are given in brackets.