Books concerning smallpox vaccination Smallpox
THE GOLDEN
CALF
AN EXPOSURE OF VACCINE-THERAPY
a book BY
CHARLES W.
FORWARD
T. H. Huxley once met Herbert Spencer in the Athenaeum. Wearing a lugubrious expression Spencer remarked, " Oh, Huxley, there's been a tragedy in my house this morning." Without waiting to hear its nature Huxley at once retorted, " Oh, I know what has happened. A beautiful scientific theory has been killed by one nasty inconvenient fact."
" Gullible, however, by fit apparatus, all Publics are, and gulled with the most surprising profit." Carlyle, Sartor Resartus.
Second Edition
LONDON:
JOHN M. WATKINS
21 CECIL COURT, CHARING CROSS ROAD, W.C.2
1933
Preface
"OPEN CONFESSIONS"
1. The Golden Calf
2. A Vested Interest at Bay
3. Pasteur and Rabies
4. The " Germ " Theory
5. Immunology
6. That Blessed Word " Research "
7. "Demoralized Research"
8. Tuberculosis : Koch and His Imitators
9. Herod Redivivus
10. Diphtheria : Old and New .
11. The Schick " Test "
Failure.
The Schick " Test "
12. Typhoid and the " Paratyphoids "
13. Tetanus. A " Useless " Serum
14. Cholera and Bubonic Plague
Bubonic Plague
15. Insulin : A " Nobel " Prize Failure
Appendices . . .
1. Water Buffalo Lymph
2. How Calf-Lymph is made
3. Encephalitis Lethargica
4. Creating Panics for Profit
5. Bechamp versus Pasteur
6. The Mellanby Fallacies
7. How Diphtheria Anti-Toxin is
MADE .....
8. Anti-Typhoid Vaccines
9. Anti-Tetanus Serum . .
ILLUSTRATIONS
Tenner Vaccinating his Son
Frontispiece
Calf on Operating Table. Effects of Vaccination, etc.
Encephalitis Lethargica. Peter and Portia Furniss ....
Vera Smith .....
Rosina Sandall .... Do. do. ....
Lucy Withers. ....
Arthur Wilson (Encephalitis) .
Mona Stevenson ....
Mrs. Raymond's Baby (Vaccino-Syphilis) .....
Matthew Thornton
Arthur Arnold (Encephalitis) .
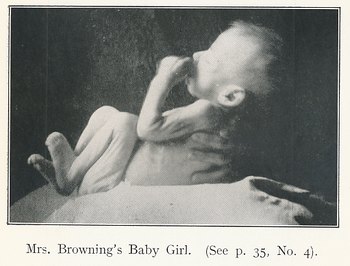
Mrs. Browning's Baby
Elly Leschewsky ....
Anneliese Pricken Medical Bureaucracy at Work Sergeant H. Nicols (Anti-Typhoid
Inoculation) ..... Henry Plant (Loss of Arm owing to
Vaccination) ....
From the day in the early eighties when I paid a visit to Pasteur at his laboratory in the rue d'Ulm, I have been impressed by two things�the lack of anything like convincing evidence that infectious disorders are caused by specific germs, and the extraordinary success with which the so-called " germ " theory has been exploited commercially.
My hesitancy to accept this theory and all that is involved in it is based more upon the equivocations, contradictions, divergencies of opinion and (sometimes unintentional) admissions of its protagonists than upon any criticisms levelled against it by its adversaries. I have been impressed, too, by the apparent levity (amounting at times to callousness) with which treatments more fraught with serious danger to the patient than anything dreamed of in the Middle Ages are applied, and, indeed, forced upon adults and young children. I find, moreover, within the ranks of the profession, and particularly in the realm of surgery serious misgivings upon these matters, which is not surprising in view of the many disasters which have followed in the wake of vaccine-therapy and the conflict of opinion amongst those who pose as authorities thereon.
Such scepticism, however, though expressed at times with considerable force, is sporadic. It does not come to the knowledge of the general public, and may even escape the notice of the busy professional man.
On the other hand, those individuals who amass fortunes by the manufacture and sale of vaccines and serum find it worth their while to carry on a continuous campaign by bombarding every medical practitioner whose name appears on the Register with printed matter extolling the virtues of their questionable products and influencing the minds of the public by announcements in the news columns of sensational " triumphs " in the " war " against disease ; of some new germ discovered; or some new vaccine concocted.
The material I have got together, though it represents a good deal of work is incomplete in many respects, but most of the authoritative opinions I have quoted are reasoned arguments not easily to be controverted, whilst the selection of facts and figures, small as it necessarily is owing to the limits of space, will afford food for reflection.
The death-rate of children from the effects of vaccination�actually higher than the death-rate from smallpox�the appalling disasters at Dallas, Bundaberg, Medellin, Baden (near Vienna), Bridgwater, Concord, Madrid and Lubeck have already recoiled upon the Medical Profession and lowered its prestige in the public estimation.
Reference is made in Chapter 4 to the remarkable extent to which the officials of the Ministry of Health appear to go out of their way to push the use of vaccines, insulin and other doubtful and dangerous forms of treatment. This is a phenomenon which merits investigation. A similar remark applies to the League of Nations Health Committee, upon which there appear to be too many " delegates " with special axes to grind.
And, finally, let me say that The Golden Calf is in no sense intended to be an attack upon the Medical Profession. It has been my privilege to number amongst my personal friends many members of that noble profession. I should be doing less than justice if I failed to remark upon the unselfish devotion to duty and the high standard of public spirit characteristic of the profession as a whole.
The candour of many whose comments appear in the following pages is in itself a testimony to their honesty of purpose.
It is to be feared, however, that in this age of commercialism and bureaucracy, the doctor has been manoeuvred into a false position and made somewhat of a " catspaw " of by the manufacturing chemists and the so-called " Institutes " which make huge profits from the sale of vaccines and similar products. (See Chap. 4.) If this work, by enlightening the more intelligent of the public, should prove helpful in indicating a way out of this impasse, it will not have been written in vain.
CHARLES W. FORWARD. Wimbledon, 1932.
I wish to acknowledge my indebtedness for the help I have received in connection with the production of this book. I am indebted to Miss L. Loat (National Anti-Vaccination League), not only for the loan of books, but for valuable information on certain points of detail, and also to Mr. A. Trobridge for reading proofs. My publisher, Mr. Watkins, has also helped me with useful suggestions. C.W.F.
" Doctors put drugs of which they know little into bodies of which they know
less."
(This applies with far greater force to-day than in Voltaire's time.)
" Our motive in paying visits and making up medicines and vaccinating babies may be questioned when we profit thereby."�Dr. R. Kay, in Brit. Med. Jour., Jan. 27, 1927.
" A new method is introduced," writes Dr. R. J. Row-lette, " it wins a certain amount of favour, it may become the fashion, and unless it is accompanied by some obtrusive disadvantages or dangers, many of us are convinced that the treatment is, if not ' the last word,' at least' a distinct advance,' and we go on with it until a new fashion takes the place of the old. Our reasoning on these matters is never logical, and rarely individual. We are governed by laws�if they be laws�of herd psychology."
" Just think how many millions of vaccine injections have been made in the course of the last few years, and in how very few cases we can definitely recognise an immediate and marked improvement, as we ought to do if the treatment is to be justified. Think, also, how often we are in doubt whether such improvement as occurs in the course of the treatment is due to the vaccine or is a natural result of the actions of the body.
" Think again in how many cases (the vast majority, indeed) there is no apparent
action at all.
" I have used vaccines extensively (employing the services of bacteriologists
for the purpose, so that I should not feel that I had not been carrying out the
treatment properly), and I have in only two or three cases seen any result which
I should not have expected without their use. I have seen lesions getting well
in one part of the body and yet, while still under vaccine treatment, fresh
lesions breaking out in the other parts of the body, and I have also seen bad
and even fatal results follow the use of vaccines,"�Sir Watson Cheyne (President
of the Royal College of Surgeons) in the Lancet, Feb. 27, 1915.
" The ultimate foundation question of the science of bacteriology is, How did the disease germs become disease germs ? But the question is still unanswered."� Woods Hutchinson. A.M., M.D.
" At first sight, the growing popularity of inoculation treatment among practitioners suggests that its utility is thereby demonstrated. But on a further view we become aware of the fact that to a large extent this accession of practical interest on the part of the doctor is due to the forcing of his hand by the patient. This, and a natural desire not to be left behind, may be responsible for much of the increase in the bulk of vaccine therapy as seen to-day, rather than honest conviction, based upon personal experience. . . . Many of us inoculate our patients because it is expected of us rather than because we feel it the best way to cure them."�Sir Thomas Horder, M.D., F.R.C.P., B.Sc, etc., at the Medical Section of the Royal Society of Medicine, Jan. 27, 1914.
" ' Listerism ' is as dead as Queen Anne, and not one day too soon. It was a fad from the commencement, followed by the obsequious crowd who pose as scientists au courant with the age. It has gone the way of many another fad in medicine and surgery. Its congener, the germ theory, on which it was based, has done an immense amount of mischief to medical science, causing a diversion from the only true basis of medical and surgical science�viz., physiological chemistry and anatomy, and bringing undeserved ridicule and contempt on the fractional part of real science to which modern medicine could justly pretend."�Dr. Campbell Black, Professor of Physiology at a Glasgow Medical School.
" It is quite true that there have been many martyrs of science, but they have
not all been scientists.
" Some men say that science says this or that, when they mean scientists, and do
not know or care which scientists."�G. K. Chesterton in Illust. London News.
" Scientifically, it cannot be disputed that from every point of view the
injection of virus capable of multiplying in the body of the individual is bad.
The effect cannot be controlled, and may lead to unforeseen results. . . .
" Who knows for how long an attenuated bacillus can lie dormant and then assume
its former virulence ? "� Professor Jas. McIntosu (Director of the Bland-Sutton
Institute of Pathology).
" The bacterial forms have not the immutability of crystals, nor even the relative stability of species among the higher plants and animals. They are variable to an extent that absolutely confounds the bacteriologist."�E. Burnet. Microbes and Toxins.
" He had never yet met a serum which was effective in killing microbes when added to normal blood . . . the introduction of antiseptics into a wound or into blood fluids or into lymph did nothing but make conditions worse."�Sir Almroth Wright (Med. Soc. of London, Oct. 27, 1930).
" With the increased use of therapeutic serums in the past twenty years, much has been written of the various manifestations of anaphylaxis. Urticaria, arthralgia, adenopathy and cardiac collapse are well-known complications of serum therapy. Coma and occasionally death have been reported following serum injections. Many reports of multiple neuritis and myelitis and encephalitis following vaccination are well known. Another unpleasant complication of prophylactic efforts, and fortunately one less frequently seen, is multiple neuritis."�Drs. George Wilson & Samuel B. Hadden, in the Journal of the American Medical Association quoted in Living Tissue, Mar. 1932.
" The truth is and I grieve to say it, that a grave disservice to medicine is suffered by the exaltation of the work of the laboratory in comparison with that of the wards, and operating theatres."�Lord Moynihan.
" One wonders whether all this laboratory research, and the ever-increasing output of literature is not somewhat in the nature of a search for the philosopher's stone."� Med. Press & Circular, June 4,1930.
They have made them a molten calf, and have worshipped it, and have sacrificed thereunto and said, These be thy gods, O Israel."�Exodus xxxii. 8.
An innovation was grafted upon Western medicine when inoculation for small-pox was introduced from the East.
It was in 1717 that Lady Mary Wortley Montagu, writing from Adrianople, declared that, of thousands who were inoculated there every year not a single one died of small-pox. She had her own son inoculated, and warmly advocated the practice on her return to England. Under her patronage, Mr. Maitland, physician to the Embassy, carried out inoculations, and, when the two children of the Princess of Wales were subjected to the operation, it rapidly became the fashion.
With a few notable exceptions the medical men of the day lent the weight of their authority in favour of inoculation, and were not only emphatic in their opinion as to the protection it afforded, but made light of the risks incurred.
The statements of Lady Montagu referred to above were remarkable for their audacity, for it is obvious that they could have scarcely had a basis other than hearsay, or the opinions of interested parties.
Small-pox inoculation was never enforced by law, and was not common among the poorer classes, but fashion made it almost de rigueur among the well-to-do.
Though not admitted at the time, it is now generally recognized that inoculation had destroyed more lives than it had saved. For by it not only was a healthy person deliberately afflicted with small-pox�from which he, otherwise, might never have suffered, but he, ipso facto, became a centre of infection in the community�a dangerous focus from which those around him might contract the disease. In fact, the prevalence of small-pox in the eighteenth century is in some degree attributable to inoculation.
It must be remarked, too, that inoculation was no more standardized than its successor, vaccination, has been. It was all a matter of chance. It might communicate small-pox in its severest and most deadly form, or, if the virus were taken at an early stage of the disease�as was done by the later inoculators �it might not actually communicate smallpox.
Sir Thomas Watson states that " By carrying the virus and the disease into every village throughout the length and breadth of the land, the practice of inoculation multiplied the foci and enlarged the sphere of contagion, insured the disease to all who were subjected to the operation, and diminished to all who had not the chance of escaping it. In truth, the total mortality was greatly increased by the process."1
1 Nineteenth Cent., 1878.
Inoculation was, at all events, as fiercely and resolutely defended by its partisans as vaccination has been in its day, yet inoculation with small-pox is to-day (as vaccination should be) a penal offence.
It is a prevalent idea that the principle upon which vaccination is based�the alleged homology of cow-pox and small-pox�was arrived at after careful and prolonged research by a highly qualified physician of remarkable attainments. So far is this contrary to fact, that Jenner possessed slender professional acquirements, and his medical degree was not the deserved result of long and careful studies, but of a business deal by which the University of St. Andrews was enriched to the tune of fifteen guineas. It was not until 1792, in the forty-fourth year of his age, that Jenner got his degree from St. Andrews. It is true that Jenner secured for himself a fellowship of the Royal Society, but his biographer, Dr. Norman Moore, admits that this incident might be described as little less than a fraud.
Eighteen years prior to this, and twenty-three years before Jenner sent his first paper to the Royal Society, Benjamin Jesty, a farmer of Purbeck, vaccinated his wife and two sons, having already treated himself in the same way some time previously. Jesty made no claim to anything in the nature of a discovery, for it was a common belief that those who contracted the disease known as cow-pox by milking affected cows were thereby rendered immune from small-pox.
It was this idea which Jenner exploited with so much success and with the result that Parliament voted him �10,000 in 1802 and a further sum of �20,000 in 1807.
Yet experience had been but brief, and certainly insufficient to justify Jenner's claim that a vaccinated person was protected for life !
Fortuitously, the belief in the efficacy of vaccination was helped by a decline in the prevalence of small-pox, a decline noticeable in the case of other forms of epidemic disease, and properly attributable to improved sanitation and general hygiene. In fact, there had been a noticeable decline in small-pox during the years preceding the introduction of vaccination. Thus, from the London Bills of Mortality we learn that whereas from 1760 to 1779 the annual number of deaths from small-pox in the Metropolis was 2,323, in a corresponding period�1780 to 1799�they had dropped to an average of 1,740, a reduction of over 25 per cent. Although the reduction continued after the introduction of vaccination, statistics have been so used as to confuse the real issue. Thus, Baron, Jenner's biographer, points out that the deaths from small-pox in 1798 were 2,237, whereas in 1802 (the year Jenner got his �10,000 grant) they were 226. This might appear to make further argument futile, but, unfortunately for the fame of vaccination, the deaths in 1797, the year before Jenner issued his paper, were 522, whereas in 1805 when vaccination was in full swing the deaths jumped to 1,685. Vaccination enthusiasts have more than once discovered that statistics are dangerous weapons to handle.1
1 The Philippine Islands, population 9,000,000, had 21,772,420 vaccinations in the fifteen years ending 1917, and then had the worst small-pox epidemic known to history. In 1918, 1919, 1920 there were 163,044 cases and 71,170 deaths, 44 per cent, of cases died. The death-rate per million living for the entire epidemic was 7,907.
The over-weening confidence of Jenner and his supporters contrasts with the comments made forty years later by Ceeley 1 who confessed that knowledge of the subject was very imperfect, and that its difficulty demanded " the continuance of vigilant, patient and diligent enquiry."
1 Variolae Vaccinae.
The idea of making vaccination compulsory by law would at one time have been (and, in fact was) scouted. Discussing the subject in the Edinburgh Review (Jan., 1810) a writer declared :�" An official body of vaccinators would never be tolerated either by the public or the profession, and would soon degenerate into a scene of jobbery and intrigue," whilst Sir Robert Peel's opinion was that " to make vaccination compulsory, as in some despotic countries would be so opposite to the mental habits of the British people and the freedom of opinion in which they rightly glory that I never could be a party to such compulsion." 2 Sir Robert Peel and the writer in the Edinburgh Review appear to have over-estimated the capacity of the British people for resisting tyranny, or the race must have deteriorated since the days of John Hampden.
2. Report of the Royal Jennerian and London Vaccination Institution, 1853.
For, three years after the death of Peel, in 1853, the first Vaccination Act was passed by Parliament, the liberty of the subject being over-ridden by the alleged unanimity of the medical profession as to the efficacy and harmlessness of vaccination. Subsequent legislation has been to some extent a case of "pull devil, pull baker" between those who favoured the practice and those who condemned it. For a long time it amounted to something very like lese majeste for a medical man to suggest that death or even any lesser evil could have resulted from vaccination, and it startled many when Sir James Paget admitted that vaccination set up "a permanent morbid condition of the blood." Ugly terms like " vaccino-syphilis " found their way into the pages of the medical press, and something had to be done. Arm-to-arm vaccination was replaced by " calf-lymph " the source of which was long shrouded in mystery, for when Prof. Crookshank made enquiries on this point he discovered that the officials at Whitehall had no standard by which the lymph was judged.1
1 Prof. Crookshank writes :�" We do not know the nature of the contagium of cow-pox, or of human small-pox, or of any of the diseases from which so-called ' vaccine-lymph ' has been cultivated for the purpose of obtaining protection from small* pox " (Sept. 20, 1894).
The attempt to identify " vaccination" as practised at the present day with Jennerian cow-pox is an amazing piece of effrontery. A range of viruses widely differing in character have been introduced as the following series will show:�(1) Cow-pox, (2) Horse Grease, (3) Horse Grease Cow-pox, (4) Swine-pox, (5) Donkey-pox, (6) Goat-pox, (7) Buffalo-pox, (8) Humanized Lymph, (9) Calf Lymph, (10) Glycerinated Calf Lymph, (11) Chloroform Calf Lymph, (12) Small-pox-Monkey-Calf Lymph, (13) Water Buffalo. (See Appendix I.)
Each of these has been successively introduced to cover up the failure of those which preceded it. The ill-effects of the present day concoction have been so marked that the authorities have deemed it wise to reduce the insertions from four to one ! Anything rather than disturb the vested interests in " vaccination."
The official views as to the modus operandi of vaccination had been based for many years on the statistics of Stockwell Hospital, which professed to give the respective failures to protect from small-pox in relation to the number of cicatrices (vaccination " marks ") showing. Thus, the rate of mortality among those with four or more clear marks was said to be 1.1 per cent.; three marks, 2.3 per cent.; two marks, 4.1 percent. The percentage of deaths among those who had no visible marks was stated to be 47 per cent. The order of 1898 1 stipulates that in " primary vaccination the public vaccinator must aim at producing four separate good-sized vesicles or groups of vesicles, not less than half an inch from one another."
1. Instructions to Vaccinators under Contract.
" To vaccinate in one place only�as is too often done, "wrote Dr. Major Greenwood,1 "is to bring the whole practice into contempt."
1 Practitioner, Oct., 1905.
On Aug. 15, 1929, an Order was issued providing for�" One insertion of lymph by a single linear insertion or scratch not more than a quarter of an inch long, merely through the epidermis."
A diluted lymph, and a technique which appears to have for its aim the avoidance of the effects which the older supporters of vaccination deemed as essential to protection, is, indeed, " to bring the whole practice into contempt."
The so-called " humanized lymph," which was obligatory for nearly eighty years, had finally to be condemned, and, since 1898, " calf lymph which no Public Vaccinator had previously been allowed to use, has replaced arm-to-arm vaccination."
During the forty-six years, 1875-1922 inclusive, 1,453 deaths were registered as due to cow-pox and other effects of vaccination.2
2. See Reports of Registrar-General for England and Wales.
A feature of the calf lymph was the addition of glycerine (see Appendix II) with a view to increase the quantity and to destroy all extraneous germs of disease. Then it was found that glycerine is itself a nutritive medium for the growth of putrefactive and other germs.
" I have heard of dilutions of lymph with glycerine," wrote a Chief Medical Officer of the Local Government Board,1 " It will, I trust, be long before such preposterous adulterations of vaccine give the opportunity of investigating their results in English practices." The primary source of calf-lymph was disclosed in a lecture at Owens College, by Dr. S. Monckton Copeman,2 who stated that small-pox material was obtained from living patients and also from the corpses of those who had died from small-pox. This matter �after being passed through the bodies of monkeys and calves�was used to " vaccinate " a number of children.
They have, indeed, made a molten calf and sacrificed thereunto, the victims having been the thousands of children and adults who have been maimed and killed by vaccination. As Mr. Chesterton satirically remarks :�" There have been many martyrs to science, but they have not all been scientists "!
1 The late Sir George Buchanan, M.D., F.R.S.
2 April S85, 1904.
" If it be true that we of physic have, really, for well-nigh a century past, been worshipping an idol of the market place, or even of the theatre, why, the sooner we cease our worship-and take down our idol the better for us altogether. We have set up the idol, and the world has lent itself to the idolatry, because we, whom the world trusted, have set the example. But the world nowadays discovers idolatries on its own account; and if we continue the idolatry it will simply take its own course, and, leaving us on our knees, will march on while we petrify."�B. W. Richardson, Asclepiad, Dec, 1889.
The history of vaccination consists of a series of failures, each discarded method being succeeded by another, and all of them differing essentially from the Jennerian formula. One may admire the ingenuity of the vaccine manufacturers, but it is evident that " for ways that are dark, and for tricks that are vain," the Heathen Chinee is not peculiar !
The indisposition of the authorities to admit any awkward facts telling against vaccination is a feature in the history of Jennerism. Thus, until 1911 it was the practice to tabulate deaths following vaccination under the heading�" Cowpox and other Effects of Vaccination." At the date referred to a new heading, " Vaccinia," was introduced. It is explained in Par. 20c1 that five deaths, all of infants, which would in former years have been assigned to the effects of vaccination, appear under the respective headings of erysipelas, pyaemia, septicaemia, convulsions, and phlegmon. Possibly the Registrar-General could offer some reason for altering the practice of thirty years, but the effect, none the less, is to exonerate vaccination by attributing death to secondary causes instead of to the primary cause�vaccination.
Evidence as to the dangers of vaccination has steadily accumulated, and a terrible list of suffering and fatalities could, be drawn up. In 1922, Profs. Turnbull and McIntosh drew attention to seven fatal cases of post-vaccinal encephalitis lethargica2 (sleepy sickness), and stated that " Vaccination was not a chance coincidence but the causal factor." After due deliberation the Ministry of Health appointed a Committee under the presidency of Sir F. W. Andrewes to investigate and advise " regarding Nervous Sequels stated to have occurred after Vaccination."
1 See Registrar-General's Report, 1914.
2 Lethargy associated with encephalitis is a most distressing symptom. The
patient feels as if all his energy had been drained away. In addition he is
mentally fogged, and feels as if there were a haze clouding his mental
processes."�Dr. N. D. Royle, Ch.M., F.R.A.C.S., British Med. Jour.,, June 12,
1932. (See also Appendix III.)
This Committee was appointed in Nov., 1923, and completed its Report in May, 1925. The contents of this Report were of so damaging a character that it was deemed advisable to withhold it from publication. Its existence was made known by a reference made to it by Prof. Jorge (Director General of Public Health in Portugal) at the International Conference on Public Health at The Hague in the following year. But even then it was not published, and it appeared belatedly embodied in the Report of the Rolleston Committee (Cmd. 3148) issued in 1928 ! In this (the Rolleston) Report ninety-three cases of post-vaccinal encephalitis with fifty-one deaths are stated to have occurred between Nov., 1922, and Sept., 1927, and in a subsequent Report (Cmd. 3738), covering the three following years, there are recorded a further ninety cases with forty-two deaths.
A question in Parliament (Feb. 23, 1932) elicited information of fifteen later cases, of which eight were fatal. Here then is an admitted total of 193 cases with 101 deaths. In The Archives of Diseases in Childhood (June, 1932) Prof. A. Eckstein declares vaccination to be the cause of post-vaccinal encephalitis in conflict with the view expressed by the Rolleston Committee who hesitated to accept the vaccinia virus as " the sole cause." Eckstein and others have shown that even in normal persons the vaccine virus can be demonstrated in the blood between the third and tenth days (and especially between the sixth and eighth) after vaccination, thus proving that vaccination results in a generalized infection. '' The view gains ground,'' writes Eckstein, '' that the vaccine virus itself is to be regarded as the actual cause of the complications." Desperate efforts have been made to explain away or to minimize the importance of these damaging and alarming facts. A typical instance is that of the M.O.H. for Newcastle-upon-Tyne, who stated :�" A great scare has been created because out of the millions of babies vaccinated one or two have developed encephalitis lethargica�a terrible disease certainly, but with which no definite connexion has been proved with vaccination."
" One or two cases," indeed ! " No definite connexion " ! ! In 1927 it was estimated that, as a result of a small-pox " scare," 1 9,000 children were vaccinated. In less than three weeks there were seven cases of post-vaccinal "nervous sequels,"whilst in two Norfolk villages (Wereham and Hillgay) the proportion of cases was over 3 per cent, of those vaccinated.
1.At Bristol.
It is certainly not in the public interest that the dangerous, and frequently fatal, effects of vaccination should be hushed up or minimized. In whose interests is it so systematically done ? The more intelligent of the working-class parents naturally refuse to have their children's health imperilled in spite of the pressure put upon them by the vaccination officers.
" I have no hesitation in saying," writes Dr. Ed. Cragg, " that if the payment for vaccination from the public purse were to cease, leaving doctors to obtain payment in the ordinary course of their private practice, in a twelvemonth a very large percentage of the profession would be anti-vaccinators." 1
1 Vaccination Inquirer, Oct., 1917.
The Herald of Health (U.S.A.) estimated that ten million dollars (two million pounds sterling) were paid to physicians in Great Britain annually that would not be paid had the law not enforced vaccination.
To-day less than 50 per cent, of the children are vaccinated, and there are actually more deaths among children under five from vaccination than from small-pox. "It is most clear to me," wrote the famous Sydenham, " from all the observations that I can possibly make, that if no mischief be done by physician or nurse, it (i.e. small-pox) is the most slight and safe of all diseases." Ludicrous attempts are made by the interested officials to magnify any slight eruptive disorder into a serious epidemic of small-pox, and by means of carefully engineered " scares " to which the press is prone to lend its support, to frighten the foolish and timid members of the community into being vaccinated (Appendix 4).
The eruptive disorder labelled variola minor is almost invariably exploited for this purpose. Yet, Sir George Newman admits that, " as a factor in the general death-rate the disease (variola minor) remains practically negligible. There is no indication of the minor variety changing into the major." 1
Dr. R. P. Garrow (M.O.H. for Hornsey) stated that he did not think the present type of " small-pox " was worth preventing. He had seen 2,000 cases. " He had been cured of any views he had ever held about the advisability of compulsory vaccination." 2
Vaccination stands to-day discredited in the eyes of intelligent people who have studied it without bias, but there are still behind it large vested interests,3 and it is realized that when vaccination goes other highly profitable forms of medical quackery will receive a serious blow.
1. Report of Chief M.O.H. (1930).
2. Roy, Soc. of Med., Jan. 25, 1929.
3. In an article in Municipal Engineering (Dec. 17, 1931), it is suggested that
the proposal that the Vaccination Acts be repealed put forward by Dr. Forbes (M.O.H.
for Brighton) would be no easy matter. " Public vaccinators and vaccination
officers and all sorts of people are so very statutory in character the moment
there is any suggestion of action they are going to take steps to prevent
interference."
It may possibly be thought that cases of injury from vaccination or inoculation are few and far between, and that those referred to in these pages are exceptional. The inference is in the other direction. Thousands of cases must have occurred in which the primary cause was never divulged in the death certificate. " In certificates given by us voluntarily, and to which the public have access," writes Dr. Henry May,1 " it is scarcely to be expected that a medical man will give opinions which may tell against or reflect upon him in any way. ... In such cases he will most likely tell the truth, but not the whole truth, and assign some prominent symptom of the disease as the cause of death."
" As instances of cases which may tell against the medical man himself, I will mention erysipelas from vaccination, and puerperal fever. A death from the first cause occurred not long ago in my practice, and although I had not vaccinated the child, yet in my desire to preserve vaccination from reproach, I omitted all mention of it from my certificate of death."
1 Birmingham Medical Review, Jan., 1874.
The tenacity with which the health authorities cling to vaccination in the light of facts is remarkable. Any slight disorder of an eruptive character is made an excuse for a revival of vaccination, and its moral if not legal enforcement.
Moreover, coercion in a most objectionable form is brought to bear by " getting at " the heads of firms and inducing them to issue edicts to the effect that their employes must choose between being vaccinated and temporary or permanent discharge. (See Rosina Sandall's case, p. 36.) Ihe plausible excuse is that they do this to protect the other workers, but if vaccination really does protect against smallpox those who are vaccinated can be in no danger. Moreover " alastrim " �the mild eruption which is magnified into a minor form of small-pox, is, as above stated, not a dangerous complaint.
The despotic attempts to force unnecessary measures involving considerable work and expense aroused protest from several Metropolitan Boroughs.1
1 Report of Chief M.O.H. (1930).
If space permitted many pages might be filled with descriptions of cases in which most serious permanent injury has followed as a result of vaccination or inoculation, and many fatal cases could also be included. It has only been possible to find space for a few selected, but quite typical cases.
Vaccination�Illustrative Cases.
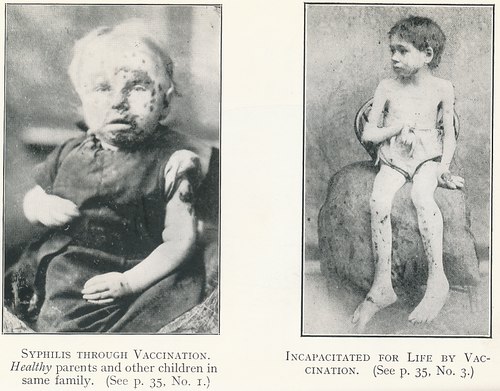
(1) Mrs. Raymond's baby girl. The parents and other children were all in good
health. This child, as shown in the photograph, suffered from vaccino-syphilis
seven weeks after vaccination.
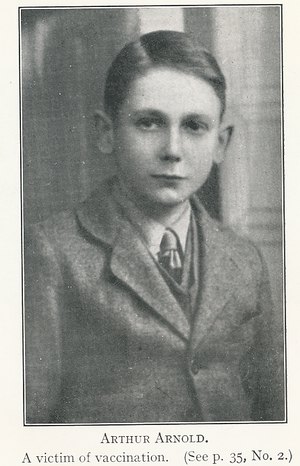
(2) Arthur Arnold, " Mayville," Villiers Road, Kingston-on-Thames, aged 14
years, vaccinated May 29, 1928, died of sleepy-sickness, June 15, 1928.
(3) Matthew Thornton. The photo shows his condition about twelve years after
vaccination. The vaccinated (right) arm is paralyzed and useless. On the back of
the hand, the elbow and shoulder were sores too hideous to be described in
detail, and exuding a foul yellow matter.1
1 See. Burnley Gazette, Mar. 26, 1890,
(4) " My baby, a fine healthy child, was vaccinated by a Public Vaccinator.
Three weeks afterwards a terrible rash broke out over the entire body, which
caused fearful agony to her. The doctor who attended her at birth is attending
her now for blood-poisoning, caused undoubtedly by the use of poisoned lymph,
and the baby is suffering severely." (Extract from a letter from Mrs. Browning
of South Lambeth. The child died shortly after it was written.)
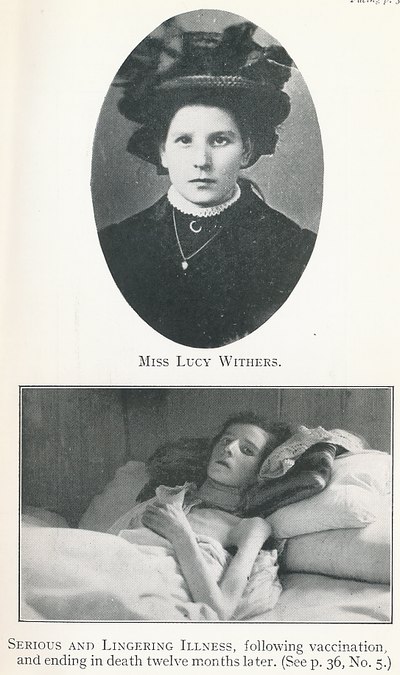
(5) Miss Lucy Withers. Vaccinated in Feb., 1909. She was never " up to the mark
" afterwards and was seriously ill from Easter onwards. The second photo shows
her a year later, and six days before her death (Feb. 16, 1910).
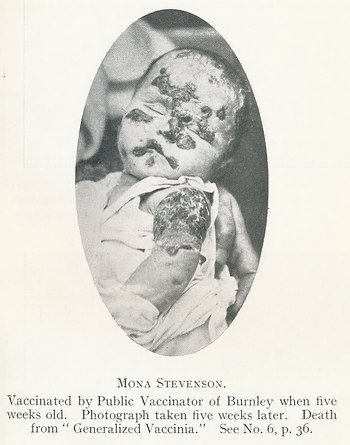
(6) Mona Stevenson, the baby daughter of a remarkably strong man, a miner.
Vaccinated at five weeks old by Dr. Clegg, Public Vaccinator of Burnley. By the
time another five weeks had passed he certified as the cause of death :�"
Generalized vaccinia, 36 days ; exhaustion."
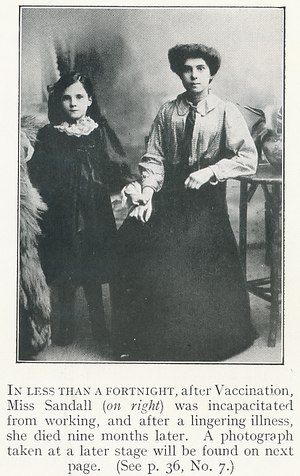
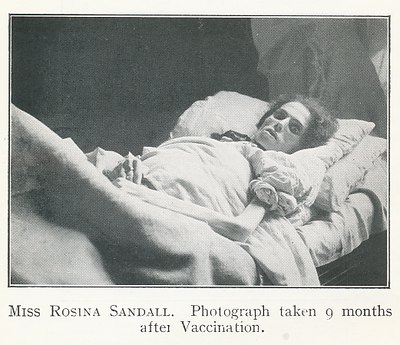
(7) In 1909, Miss Rosina Sandall, aged 22, of Bristol, was one of a large number
of employees who submitted to re-vaccination because of fear that they would
otherwise lose their situations, a slight outbreak of small-pox having been made
the occasion of one of the usual " scares." She was vaccinated on Feb. 13th,
and, within a fortnight, sores broke out on her arm and foot, and she was never
able to resume her occupation. By Nov. nth she was�with the exception of her
feet, which were swollen and painful�a " living skeleton." She died on Nov. 14
after nine months of great suffering.
(8) Vera Smith, aged fourteen, of Byron Avenue, Manor Park. A bright, healthy
girl. Died of " post-vaccinal encephalitis," the result of vaccination, June,
1929.
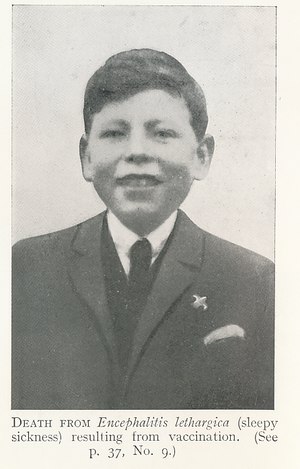
(9) Arthur Wilson, aged fourteen, of 155 Hugh Street, Castleford, Yorks. A
healthy boy who died of " post-vaccinal encephalitis " in November, 1928.
(10) Peter and Portia Furniss (twin brother and sister) aged four and a half
years, of South Wigston, near Leicester. Died (one 24 hours after the other) of
" post-vaccinal encephalitis " in May, 1931. They had been vaccinated a
fortnight previously with Government lymph !
[The following cases are interesting as having occurred (with innumerable
others) in Germany, where vaccination is rigorously enforced, and which is held
up by pro-vaccina-tors as a pattern for this country to follow.]
(11) Elly Leschewsky. A healthy girl prior to being vaccinated. The condition of
her arm shortly after vaccination is only faintly indicated in the photograph.
(12) Anneliese Pricken. A healthy baby. Died when eighteen months old from the
effects of vaccination five weeks previously.
" His very achievements in the right direction, however, make any error on his part al] the more dangerous, and make it all the more the duty of thinking men to sift the evidence upon which he rests his extravagant claim of having discovered a means of preventing the outbreak of hydrophobia."�Dr. Charles W. Dulles (Philadelphia).
The possibilities of exploiting a plausible theory such as vaccination were hardly likely to be overlooked. Edward Jenner�"that fortunate �sculapian," as Sir Benjamin Richardson described him,1 had received thirty thousand pounds not for the results of years of laborious work but for researches gathered from " common-place experience, which, by good fortune of time and circumstance, were turned into extraordinary fame."
1 The late Chief Statistician at the Ministry of Health, Dr. M. Greenwood, declared that there was a good deal of evidence that jenner had been a rogue.
Vaccination was, from a commercial point of view, a remarkably good proposition. There was first the manufacture of the " vaccine," in itself a highly profitable industry, and there were also the sums of money�enormous in the aggregate�paid in the shape of fees to public and private vaccinators !
When vaccination was made compulsory it was little to be wondered at that the more commercially-minded members of the medical community should visualize a world in which not only they that are sick should have need of a physician, but also they that are whole. For, if the latter could only be persuaded to undergo treatment to ward off, or render them " immune " from, each of a series of disorders (all of which many persons now escape) it opened up enormous possibilities in the shape of financial gain to all engaged in the business.
It was to the French chemist Pasteur that the world owes the linking up of bacteriology with medicine as a highly lucrative commercial proposition.
Louis Pasteur distinguished himself as a chemist when, in 1848, he investigated the relation between composition, crystalline form, and optical activity, and helped to establish a new branch of science�Stereochemistry. At Lille he found opportunities to investigate the processes of fermentation as applied to the production of wines and beers. In 1857, as Director of Studies at the Ecole Normale, he proved that fermentation is the result of the action of minute organisms, and seven years later he disposed of the theory of spontaneous generation.
Pasteur had developed a clever technique as a microscopist and bacteriologist, and was able to apply this in his investigations on silk-worm disease with the result that his fame in France steadily increased, and problems such as chicken cholera and anthrax in cattle1 were submitted to him for investigation.
As Pasteur had never had any training in biology, pathology or medicine it is obvious that he could only approach such problems as the causation and cure of disease from the point of view of a laboratory chemist. (See Appendix 5.)
Yet, this fact did not deter him from claiming, upon what appear ludicrously insufficient grounds, to have discovered a remedial treatment for hydrophobia.
His experiments began by inoculating two rabbits with the mucus taken from the mouth of a child who had died four hours previously after having been bitten in the face by a dog a month earlier.
1 Inoculation, as preventive of charbon, was practised upon 4,564 sheep at Kachowka in Southern Russia, of which 3,696 died.
The rabbits were both dead within thirty-six hours. The saliva of these rabbits transmitted the disease to other rabbits. Dr. Raynaud, who had been making similar investigations, came to the conclusion that the rabbits had died of hydrophobia.
Upon the strength of this surmise, and after some further investigation, Pasteur communicated a note to the Academie des Sciences, entitled :�" On a new disease produced by the Saliva of a Child dead from Hydrophobia."
He was, apparently, not aware that, as far back as 1844, Dr. Samuel Wright had contributed a paper to The Lancet in the course of which he remarked that healthy saliva, when injected into the veins, produces symptoms closely similar if not actually identical with those of hydrophobia ; and, if the quantity be sufficient, death, apparently hydrophobic, is a consequent result.
It was upon this slender foundation that the Pasteur legend was built up. Hydrophobia, a by no means common disorder, was written up in the press as a scourge that constantly threatened humanity. As usual, statistics were forthcoming which (with a little manipulation) conveyed the impression that a marked reduction in the number of deaths had followed the Pasteur treatment. How do the facts stand ?
For the thirty-five years preceding Pasteur's treatment the annual average of deaths from hydrophobia for the whole of France was 31.1 For the nine years following, the annual average was the same�31 deaths. But the figures furnished the world by the Institut Pasteur exclude an average of 16 deaths of persons who had not been treated by Pasteur, and it is stated that the directors did not include in the statistics cases where deaths occur in the course of treatment or those which take place within fifteen days of the last inoculation.
1 " Statistics show that a large number of persons are bitten annually without any bad results, and also that a large number are bitten by rabid animals with impunity, and that this impunity is secured by attention to the wound."�Thomas M. Dolan, M.D.. F.R.C.S.
When statistics are dealt with in this partisan fashion, the compiler being biased by considerations of a commercial character, they become practically valueless and may be so presented as to lend support to any theory.
" M. Pasteur has been obliged to propagate a belief in the frequency of hydrophobia. Now, hydrophobia in man is a rare, a very rare disease. I have seen only two cases in thirty-five years of hospital and civil practice ; while my colleagues, both in town and country, count the cases they have seen by units, and not by dozens (still less by hundreds). To magnify the advantages of his treatment, and to conceal his failures, M. Pasteur has every interest in exaggerating the annual mortality from hydrophobia in France, but this is not in the interest of truth." 1
1 Prof. Peter (Member of the Academy of Medicine, Paris, and successor of Trousseau).
The list of failures of Pasteur's treatment for hydrophobia is a ghastly one, and would occupy many pages. Nor has the Institut Pasteur learnt anything apparently during the years that have intervened.
On September 15,1924, Joseph Antoine, a lad of seven years, was bitten by a cat. Shortly afterwards the cat bit one of his sisters who appeared no worse for the incident. The boy received the Pasteur treatment, and fifteen days later became apathetic and subsequently complained of pain in the left hip (the side opposite the bite) and limped. His temperature rose to 38.5�C, he lost strength, and, four days later, paralysis of the lower limbs appeared, and death followed from spinal paralysis (Landry's).
In Hydrophobia Statistics, Pasteur Institute, Weltevreden, Table 6 gives 192 deaths after Pasteur treatment. These were attributed to paralysis, but the more probable cause is some unknown property of the "vaccine."
Colonel W. F. Harvey and Major H. W. Acton state that " anti-rabic immunization, be it by dried cords, dilution, or dead virus, is in urgent need of standardization and evaluation of its degree of efficacy," and further, " We have definite proof that large doses of healthy brain matter when inoculated into susceptible animals give rise to paralysis and even to death."
In his Pasteur Treatment, Fermi states :� " Premising that in practice we must save men and animals already bitten, the results of Pasteur have not been confirmed by any subsequent investigator."
" In our present state of knowledge," writes Prof. Karl Pearson, F.R.S., " I venture to assert that it is not wise to speak of the conquest of rabies." 1
Prof. Peter told the Academy of Paris as far back as Jan. n, 1886, that anti-rabic treatment was not only useless but dangerous, and that, instead of curing, M. Pasteur actually gave hydrophobia.
Dr. Thomas Dolan states that a careful examination of the tabulated statement of deaths forces one to the conclusion'that " not only does M. Pasteur not protect from the disease, under the very conditions demanded by himself, but that he has added anew terror to it by the introduction of paralytic rabies." 2
1 Times Literary Supplement, Jan. I, 1920.
2. Pasteur and Rabies (G. Bell & Sons).
The use of the word " vaccine " is explained by Pasteur as follows :�" J'ai donne a l'expression de vaccination un extension que la Science, je l'espere, consacrera comme un hommage au merite, et aux immense services rendu par un des plus grands hommes de TAngleterre, votre Jenner." 1
1 Transactions of Internat. Med. Congress, 1881, Vol. I, p. 90.
The real reason for using the false description, " vaccine," was more probably the calculation that so dangerous an innovation could be more easily " put over " by some sort of camouflage. At all events the word has since been loosely and indiscriminately applied to all and sundry preparations of this kind, though the cow is in no way associated with their production.
" The most remarkable point in the whole discovery against rabies," said Roux, in his Croonian lecture, " is that it has been carried out, the virus itself being still unknown ; not only do we not know how to cultivate it outside the body, but in allowing it to be really a microbe, we can but do so by analogy, for as yet no one has been able to isolate it."
It is curious how, seventy or eighty years after Jenner received his douceur at the hands of the British Parliament, imitators such as Pasteur, Koch and others should have again discovered how to exploit disease commercially.
The profitable business of vaccination appears to have fired the imagination of experimentalists, and a wild search for the " specific germ " of every infectious disorder was started. Just at the time Pasteur was claiming to be able to cure hydrophobia, the startling news came from Germany that a Dr. Robert Koch, who claimed to have discovered and isolated the bacillus tuberculosis, had introduced a new method of treatment and that the conquest of consumption was un fait accompli !
" If I could live my life over again I would devote it to proving that germs seek their natural habitat�diseased tissue�rather than being the cause of the diseased tissue, e.g., mosquitos seek the stagnant water, but do not cause the pool to become stagnant."�Prof. Rudolph Virchow.
It is doubtful if any superstructure in the shape of hypothesis has ever been raised upon flimsier basis of fact than the theory of the specific " germ " as the causative factor in disease�the theory that each disease has its own particular bacterium, and that, in the words of Florence Nightingale, as quoted by Tyndall,1 the matter of each contagious disease reproduces itself as rigidly as if it were dog or cat.
1 Floating Matter in The Air.
Miss Nightingale actually wrote�" I was brought up both by scientific men and ignorant women to believe that small-pox, for instance, was a thing of which there was once a first specimen in the world, which went on propagating itself in a perpetual chain of descent, just as much as there was a first dog, and that small-pox would not begin itself any more than a new dog would begin without there being a parent dog. Since then I have seen with my eyes and smelt with my nose small-pox grow up in first specimens, either in close rooms or overcrowded wards, where it could not by any possibility have been ' caught,' but must have begun. Nay, more, I have seen diseases begin, grow up, and pass into one another. Now dogs do not pass into cats. I have seen, for instance, with a little overcrowding, continued fever grow up, and with a little more typhoid fever and with a little more typhus, and all in the same ward or hut." 1
1 Notes on Nursing,
This so-called " Germ " Theory has brought about a revolution in medical treatment. It has destroyed medicine as an art, and failed to re-establish it as a science. By means of it medicine has become commercialized, and sickness and the fear of sickness are systematically exploited for pecuniary profit.
The apotheosis of Pasteur has subordinated the role of the " beloved physician " whose highest interest was the welfare of his patients, to that of the self-seeking serum-monger and anti-toxin manufacturer, whose scarcely-concealed aim is to utilize the medical practitioner as his agent.
The practitioner who hesitates to follow the newest fashion in medical treatments from conscientious doubts as to its efficacy, misgivings as to its dangers, or because he feels it has not been sufficiently tested, may be admired for his courage, but will almost certainly suffer financially.
" Of medicine," writes Osier, " many are of opinion expressed by one of Akenside's disputants at Tom's Coffee House, that the ancients had tried to make it a science and had failed, and the moderns to make it a trade and have succeeded." And he further remarks that the practice of medicine "is an art, not a trade ; a calling, not a business."
" What we have to fear," declares Dr. Robert Hutchinson,1 " is the influence of the mass mind . . . the exploitation of discovery for commercial ends . . . the pull of the politician, the philanthropist and the press."
1 Harveian Oration.
The notion that disease can be studied apart from the patient could only have emanated from a laboratory, and a doubtful service was rendered to medicine when the comparatively recent science of pathology began to be separated from physiology with which it is closely allied.
Disease is not an entity, but a derangement, and cannot be classified, docketed and organized as an exact science (as the disciples of the Pasteur school would have us believe). Dr. Chassaigne has expressed this truth with clarity and force :�" Vous demandez des certitudes, ce n'est surement par la medicine qui vous les donnera. . . . Certes, il est des maladies qui Ton connait admirablement, j usque dans les plus petites phases de leur evolution; il est des remedes dont on a etudie les effets avec le soin le plus scrupu-leux; mais ce qu'on ne sait pas, ce qu'on ne peut savoir, c'est la relation du remede au malade, car autant de malades, autant de cas, et chaque fois l'experience recommence. Voila pourquoi la medicine reste un art, parcequ'elle ne saurait avoir une rigueur experimen-tale! toujours la guerison depend d'une circonstance heureuse, de la trouvaille de genie de medecin. Et, alors, comprenez done que les gens qui viennent discuter ici me font rire quand ils parlent au nom des lois, en medecin. Ou sont-elles ces lois, en medicin ? Qu'on me les montre ! " 1
1 Dr. Chassaigne, Lourdes, p. 198
To the ordinary man or woman the germ theory implies the existence of minute organisms definitely maleficent to the animal body. The biologist, however, sees in the germ or bacterium a species of flora playing a part in the scheme of nature.
In the special branch of botany known as bacteriology the vegetable micro-organisms have been classified as follows :�
(1) Hyphomycetes or Moulds.
(2) Blastomycetes, or Sprouting Fungi.
(3) Schizomycetes or Fission-Fungi.
It is to the last class that most of the alleged " disease-producing " germs belong.
One of the striking features of microorganisms is their variability of form, or what is described as " polymorphism/' a factor which renders identification�a sine qud non of the theory of " specificity "�very difficult, and accounts for the many divergencies of opinion on the subject. " Modern researches on variation and mutation reveal an uncomfortable habit in bacteria of acquiring fresh characters when brought into new environments " {B.M.J., 23.5.1914). Moreover, there are conditions under which certain germs alter their shape, losing their ordinary form, and becoming unrecognizable.
" It is certain that it is not only the form but also the species which is variable amongst the bacteria, and this variability is even more characteristic of their physiological properties than their shape." 1
1 E. Burnet, Microbes and Toxins.
Thus, the so-called cholera germ may change from a vibrio to a bacillary or coccoid shape ; if grown on blood serum or agar-agar the alleged diphtheria bacillus often becomes elongated, clubbed or branched; whilst tubercle bacilli show a similar tendency, and anthrax bacilli may grow as yeast forms. " Vibrios " may become spirilla ; the ray-fungus pass through a coccoid and bacillary stage ; and the diphtheria bacillus be long, short, straight or clubbed. In ordinary broth typhoid bacilli will appear in one form, but in carbolized beef-broth their form will differ widely. Little wonder that a pathologist at St. Bartholomew's Hospital should have declared the question to be " beset with so many difficulties that we must for the present be content with an arbitrary standard based, perhaps, on preconceived ideas." 1
1 Kanthack, Allbutt's System of Medicine.
In noting the effect of violet rays upon the rod-shaped bacillus of anthrax, Mdme Henri, of the Pasteur Institute, found that this organism changed into a round coccus�a totally different germ. Moreover, when a guinea-pig was inoculated with this germ the diseased condition set up bore no resemblance to anthrax.
When the discovery of the Klebs-Loffler bacillus was announced we were told that a reliable diagnosis of diphtheria was assured, but " now we are told that the bacillus of Klebs and Loffler is not found in some of the cases which we have been accustomed to call diphtheritic." 1
" The diphtheria bacillus," writes Dr. Runge,2 "is capable of relinquishing, spontaneously and completely, its most characteristic property, its infectiousness."
1 S. J. Gee, M.D., F.R.C.P.
2 New York Journal (1912).
From the above it will be seen how very serious are the difficulties in the path of the bacteriologist who sets out with the idea of classifying his flora with a precision approaching that of the curator of Kew Gardens. Unfortunately for the bacteriological pathologist there are other difficulties not less serious to be surmounted.
Bacteria can only be properly studied when growing, and the bacteriologist can only watch their growth on various artificial media in test-tubes and incubators. This method may constitute an interesting hobby, but to attach to it any scientific value as indicating what takes place in the living human body is obviously absurd.
Dr. A. A. Kanthack is very plain spoken on this subject. " In the laboratory," he writes, " we can only place them [germs] in conditions which approximate, often very slightly indeed, to those pertaining to them in nature. In most cases the artificial cultivation of bacteria in test-tubes and incubators has no pretence to resemble natural growth ; it is merely an experimental device by which we seek to unravel the mysteries of microbic life. We vary the soil as much as we can, we alter the surroundings, we imitate what we suppose to be the natural state ; but as we can never reproduce this exactly, our conclusions can only be regarded as approximations to the truth. In bacteriology conclusions are too readily drawn on incomplete evidence, yet in this study especially rigorous and unimpeachable evidence is required."
This lack of analogy between the cultivation of bacteria in the laboratory, and their behaviour within the tissues of a living animal appears to constitute a fatal flaw in the " specific germ " theory. The difficulties are acknowledged, and even emphasized by the more candid writers on this subject.
We are " far too ignorant," declares the writer already quoted, " of the minute changes, chemical or physical, in the tissues to speculate with any degree of promise ; but this much is certain, that, even if we choose media most closely resembling the tissue substances, we cannot reason directly from changes in the test-tube to changes in the animal body." 1
1 Kanthack
" We must always remember," he continues, " that the artificial media used in the laboratory for the cultivation of micro-organisms are ' artificial,' and the phenomena observed under these conditions are evidently not the natural ones."
The much-vaunted laboratory tests can have little scientific value in view of the above statements, for, as Dr. Carmalt Jones, of Westminster Hospital, remarks:� "It is undoubtedly possible to send specimens of the same serum to different laboratories, conducted by capable authorities, and to get different results from each of them." 1
1 British Mid. Jour., Nov., 1914
And further, " we must realize that we know very little of the natural life and habitat of most pathogenetic organisms."
It may be well to ask, at this stage, whether the germ theory is supported by facts. " Hypotheses, if they are well made, are at least great helps to memory, and often direct us to new discoveries. But we should not take them up too hastily (which the mind that would always penetrate into the causes of things, and have principles to rest on, is very apt to do) till we have very well examined particulars, and made several experiments on the thing which we would explain by our hypothesis, and see whether it will agree to them all." 1
1 John Locke.
Certain " postulates " have been laid down as essential to the soundness of the germ theory. The specific germ must be (a) a parasite or a facultative parasite ; (b) it must be found invariably in the tissues of an animal dead from or affected with the disease in question ; (c) it must never under any circumstances occur in other diseases, nor within the normal tissues; (d) the organism transmitted from the diseased or dead animal to an unaffected, susceptible animal must reproduce the lesion, and in this second diseased animal the original organism must be found; (e) if the organism can be cultivated outside the animal body, then an artificial cultivation inoculated experimentally into a susceptible animal must again produce the disease, and this animal must again contain the organism in its tissues or blood ; (f) these processes must occur in invariable succession under identical conditions; (g) the toxins and poisonous substances obtained from the artificial cultivations must agree chemically and physiologically with those obtained from the diseased animal.
Now, at least b, c, d, and e would appear to be vital to the theory, yet, upon no less an authority than the editor of The Lancet it is admitted that " it must be acknowledged that all these postulates are complied with very rarely indeed, if ever." 1
Dogmatism appears to take the place of logic where the germ theorist is concerned.
" The Klebs-Loffler bacillus is found in every case of diphtheria," writes Dr. Kanthack, and with unconscious humour he remarks, " We must refuse to call any lesion diphtheria unless it is associated with the bacillus."
In other words, if the facts are against the theory so much the worse for the facts !
The Lancet 2 states that the Klebs-Loffler was absent in 14 per cent, of the cases of clinical diphtheria, the Report of the Royal Commission (1912) puts the percentage at 20, whilst Osler 3 declares that the bacillus is not to be found in 28 per cent, to 40 per cent, of the cases.
" In patients with positive ' swabs ' the bacilli are not always biologically diphtheritic or virulent." 4
1 The Lancet, Mar. 20, 1909,
2 Sept., r928.
3 British Med. Jour., Feb. 13, 1926.
4 British Med. Jour., Feb. 13, 1926.
" Cases present themselves," says The Lancet, " with all the symptoms and signs of Pulmonary Tuberculosis without the presence of Tubercle bacilli." 1
In the Lubeck trial it was stated that the presence of Koch's bacillus was necessary to tuberculosis. Yet, in 25 cases of peritoneal tuberculosis examined by Borchgravink, only seven had any bacilli at all, and only one of the seven showed them in abundance. The acute cases were all in the group of 18 which had no bacilli at all.
In 848 cases of venereal disease (adult women admitted to the Lock Hospital) the gonococcus was found in only 411, whilst it was not found in 437 cases which showed gonorrhoea clinically.2
Let us turn to postulate " c." The disease having been found to exist without the bacillus, it will also be found that the bacillus may be present without the disease.
In the Manual of Bacteriology 3 it is stated that Klebs-Loffler bacilli were found in the throats of 15 per cent, of children admitted to the Victoria Hospital, Chelsea.
1 Nov. 15, 1919.
2. Dr. J. J. Abrahams, Roy. Soc. of Med., Feb., 1932.
3. Hewlett.
In a Report of the Ministry of Health (No. 10) p. 14, it is stated that in the Willard Parker Hospital, New York, of 1,200 patients 20 per cent, had diphtheria bacilli in their throats, and were in contact with diphtheria cases, and yet in no single instance developed diphtheria, although in many cases the bacilli were of a virulent type.
We thus have the disease without the germ, and the germ without the disease. So much for postulates " b " and " c."
Except with the connivance of heroic volunteers postulate " d" cannot be tried out on human beings, but whether tried on men or animals any conclusions must be far from reliable, as the introduction of any toxic agent into the system is likely to produce a more or less marked reaction.
In the earlier days of the germ theory, Pettenkofer boldly swallowed a whole tube of cholera germs " containing enough of the comma bacilli to poison a regiment," but no ill effects followed.1
1 Microbe Hunters, de Kruif, 1927, p. 1.
Dr. John B. Fraser carried out elaborate investigations on himself and five volunteers. About 50,000 Klebs-Loffler bacilli were swallowed to test whether diphtheria followed. Further quantities of 100,000, 500,000 and a million more were swallowed without any ill effects.
Fraser describes a series of tests to decide whether the Eberth bacillus would cause typhoid. Most of the cultures were grown from stock tubes supplied by Parke, Davis and Co., and one furnished by the Toronto Board of Health. Each test was negative though millions of germs were swallowed. A further series of tests showed that one might swallow a million (and over) pneumococci without causing pneumonia or any disturbance.
The germs were given in milk, water, bread, cheese, meat, fish, and apple. Six persons (three male and three female) voluntarily took part in the tests and the investigation lasted about two years.1
Dr. Etienne Burnet, of the Pasteur Institute, states that Koch's discovery of the "Cholera bacillus" had to contend with an obstinate scepticism because cholera could not be produced with it at will in laboratory animals, and even when several savants swallowed cultures of it the results were very inconstant.2
1 Canadian Lancet, quoted in Vacc. Inq., Oct., 1917.
2. Microbes and Toxins.
" We should not bring the art of medicine into disrepute by quack-like promises."�Sir W. Osler, Life, by Harvey Cushing, p. 179.
The miscalled " science " of immunology rests upon the assumption that the body is constantly liable to be attacked by disease in the materialized form of microbes or " germs"; that each disease has its specific germ; and that the powers of the body are perpetually engaged in the attempt to overcome the maleficent invaders.
This particular view is summed up in the following extract:�" Normality of health is not the absence of attack and struggle ; the body is never under ordinary environment free from the incessant contest. Disease is the sign of temporary or progressive failure in defence." 1
1 Report of Medical Research Council, 1925.
It is suggested that, taken, so to speak, unawares, the body is unable to put up a sufficient resistance. The immunologist contends, however, that the feeble powers of resistance may be increased, not by cultivating vigorous health, but by introducing into the system the germs (or theif toxins) of particular diseases in a less virulent, or " attenuated " form.
This idea has been ingeniously elaborated, and we are told wondrous stories of "
antigens " and " antibodies " which act as defensive hosts and which it is
claimed the immunologist can increase in strength and numbers.
The theory has been developed with a fixed determination to take a great deal
for granted, and to ignore many inconvenient facts.
The refusal of the facts to support the hypothesis, and the nebulous character of the so-called evidence has been referred to in Chapter IV.
This concept of disease as a definite entity �the basis of Pasteurism�comes into conflict however with the views of not a few of the most notable authorities in the medical profession, who refuse to draw a sharp line between the conditions respectively described as " health " and " disease," preferring rather to view the former as a balance of the physiological processes, and the latter as a disturbance of, or deviation from that balance.
" Health, whether of body or mind," wrote the late Sir Clifford Allbutt, " is not a fixed position or rotation ; it is an oscillation about an ideal axis ; but the stability of this complex system about its axis or axes is a marvel." And he further expresses the opinion that "to regard and name diseases as species, or even as varieties, in a biological sense, is an error of the same kind as to regard them as entities. A disease is a particular state of an individual, and, although certain families show persistent bents to certain kinds of morbid variation, yet the constancy of this fashion bears a very small proportion to that of the characters of a variety in a biological sense." 1
The late Sir F. Treves declared " not only is there nothing preternatural in disease, but it is the outcome of natural processes ; and, more than that, there is evidence to show that many of its manifestations and of its methods are marked by a purpose, and that that purpose is beneficent.
" The time has come when it would rather appear that many of the so-called symptoms of disease are expressions of a natural effort towards cure, that they are not only not malign in their intent but have for their end the ridding of the body of the very troubles which they are supposed to represent." 2
1 Allbutt. A System of Medicine {Introduction).
2. Address at University College.
Dr. Pye-Smith remarks, " We call that which brings us discomfort' disease,' and look upon disease as obtrusive, abnormal, unkindly, but, if we knew it, the highest temperature of fever is as strictly in accordance with the laws of animal thermogenesis and thermolysis as the slight diurnal oscillations of health ; and the excessive secretion of the kidneys in diabetes is as much a part of the system of nature as the moderate increase produced in a healthy man by a cold east wind or by copious draughts of water." 1
There would seem to be no common ground between such diametrically opposite views as those of the authorities above quoted, and that held by immunologists. Either the body is a marvellously constructed machine that� provided the laws which regulate its action are complied with�will maintain its integrity for a century or longer, or it is an unstable organism, more or less imperilled by its environment, and engaged in a constant, and, but for the immunologist, futile and unequal struggle against hosts of unseen enemies. It is, however, not possible to observe the actual processes which go on in the normal human body, and the immunologist, who need not have " studied medicine or science," 2 has to fall back upon laboratory experiments which, as Kanthack informs us, approximate, often very slightly indeed to those pertaining in nature. All that he needs is a micro-scopist's outfit, some pus, blood or excreta of a patient suffering from some special disease, and a supply of guinea-pigs or other animals. With this outfit he can evolve any wild hypothesis or weave as many cobwebs as he likes in the shape of fantastic theories.
1 Lumleian Lectures, 1892.
2. Dr. Etienne Burnet (of the Pasteur Institute).
By means of such simple expedients, and the help of confiding newspaper editors, he may get his name before the public as a pioneer. Nor can this statement be brushed aside as being merely the view of an ill-informed and incompetent critic, for Prof. F. W. Twort1 has pointed out how easy it is for a second-rate man to be appointed as bacteriologist to a hospital, and to publish " research work " mediocre in quality, or he may fall into one of the pitfalls and his results be obviously wrong. " It is very easy," writes Mr. Twort, " for a man even with a small knowledge of his subject, to impress those with less." And he goes on to show that the very type of man he has in mind may quite easily be acclaimed as a leading bacteriologist, recognised by Government departments, perhaps become one of their expert advisers, and receive grants for his researches. " Can it be wondered at," he asks, " that at least nine-tenths of the so-called discoveries are eventually recognised even by practical surgeons to be worthless ? "2
The theory associated with the name of Metchnikoff�" phagocytosis " rests upon the apparent ingestion of bacteria by the phagocytes of white corpuscles of the blood. It is a fascinating concept�these serried hosts of white corpuscles preying upon man's mortal but unseen foes. Metchnikoff's conception was that " acquired immunity is due to the leucocytes having by a process of training (as he called it) acquired a power of more effectively confronting, ingesting and destroying microbes."3 Fascinating as was Metchnikoff's theory of phagocytosis, he had to modify it from time to time until very little was left. In fact, in the course of the combat between the cell and the invading germ the phagocyte was sometimes vanquished (as Gebritchewski demonstrated), being destroyed by the products of the bacteria it had ingested. " Us ont fait de leur mieux en englobant les microbes, mais ceux-ci se sont adaptes aux milieu interieur des cellules, et ils ont triomphes."4 It lent itself to the elaborations of Wright and Neufeld that certain body fluids played their part in preparing the bacteria for phagocytic digestion. This opened the way for the " opsonins" of Wright and the bacteriotropins of Neufeld�" a new flowering of the phagocytic doctrine," as Ehrlich expresses it. Metchnikof's sage criticism on Wright and Neufeld is that the behaviour of leucocytes taken out of the body, washed, and in an artificial medium can hardly represent the phenomena which take place in the tissues of the living body.
1 Of the Brown Institution.
2 Daily Telegraph.
3 Sir Almrotli Wright,
4 Roux, Trans. Int. Cong, of Hygiene, 1891.
Whenever the chemist invades the realm of the biologist he needs careful watching. A case in point is that of Ehrlich and his " side-chain " theory. The term itself is borrowed from the chemistry of the benzene compounds. Ehrlich attempted to establish an analogy between the benzene " ring " of the chemist and the living cell of the biologist. In order to embrace in it the almost unlimited complexity of facts observed in experiments with the various antibodies, anti-toxins, haemolysins, bacteriolysins, precipitins and agglutinins, he developed his theory to a degree of complexity that carries it well beyond the comprehension of the ordinary man.
Referring to the " side-chain" theory, Wright remarks that it " would seem to lie open to critical assault in that the hyper-replacement of side-chains does not necessarily conduct to an excretion of these into the circulatory blood. In point of fact, in the case of muscle, on which Ehrlich here relies, it leads to something very different, to a hypertrophy of this tissue." 1
" Ehrlich's theory," writes Burnet, " is dangerous, in that it offers too readily conceptions which have the appearance of explanations, and which, therefore, are apt to dull the appetite for research."
" Ehrlich's original conception of immunity neither corresponds with the facts nor explains the processes of cure." 2
Popular as Ehrlich's side-chain was for a time, it is a striking comment as to its lack of permanent value that in Muir and Ritchie's Bacteriology (Ninth Edition, 1932) two pages are considered sufficient to devote to it out of the sixty-odd pages in the chapter on immunity.
What happens when sera or anti-toxins are inoculated into a human being can only be guessed at, and the guesses will almost certainly be wide of the mark. If death follows inoculation it is easy to say that the condition of the patient was so serious that not even serum could save him ; if he recover it is equally easy to claim it as another triumph for seropathy.
1 Encyclo. Britannica ; Art. " Immunity." XIV Edition.
2. Di Christina : Atti
della Pontificia delle Scienze, 1927.
The basis of the various theories of immunity is experiments made outside the body, or, as it is usually described�in vitro.
All attempts to define immunity in the terminology of the chemist are futile. This applies to the theory of Arrhenius, Madsen, and Walbum, who criticize the complexity of Ehrlich's views, but whose own theories are open to the objection that they apply the laws of chemical equilibrium and rates of reaction in speculations as to the reactions which go on between bodies of which nothing is known from the chemical point of view.
The more one studies the theories of immunity, the more complex the whole subject is found to be. Singer, assuming that invading organisms are the cause of disease, and that the body, under various forms of excitation, is constantly throwing into the blood stream substances which are directly or indirectly inimical thereto, remarks, " of the chemical nature of these substances we have no knowledge." 1
1 Short History of Biology, p. 449
Paradoxically, however, it is from Sir Almroth E. Wright�the originator of the system of anti-typhoid inoculation�that one may quote the most damnatory passages in criticism of vaccine therapy. The following extracts are taken from his Studies in Immunisation, and, in order to enable the reader to follow the argument, certain portions have been set in heavier type, which they are not in the original. For it might be said that these passages were written some time ago, and that Sir Almroth has altered his views. The statements below are, however, couched in such emphatic language, and bring out with such force the " insuperable" difficulties (which, from the point of view of the patient, maybe described as dangers) in predicting the effects of inoculations. Not less ironical is the admission of this eminent immunologist that " acquired immunity may in many cases be presented to-day and gone to-morrow." 1
1 Encyclo. Britannica. XIV Edition.
" Though inexperience might suppose," writes Sir Almroth, " that the blood testings, which had been carried out, and the clinical experience which had been gained, would enable us to tell with absolute accuracy the effect of a given dose of this or that vaccine upon the human organism, we have not only not arrived at this point, but there is very little likelihood of our ever arriving at it. When we are handling, on the one hand, vaccines, and, on the other hand, the human organism, we are dealing with factors neither constant nor invariable.
" Let us consider, first, the vaccine. Here, even where we particularise a particular dose of a vaccine which has been standardised by counting the contained microbes or by weighing the contained microbial substance, we can never leave out of consideration the possibility that a difference in the strain of the microbes, or some minute overlooked difference in the mode of preparation, or, perhaps, some change occurring spontaneously during keeping might affect the potency of the vaccine. It will follow that where we prescribe, let us say, a dose of gonococcus or streptococcus vaccine such as would correspond to 1,000,000 gono-cocci, or, as the case may be, 1,000,000 streptococci, we cannot always be sure that we shall be applying precisely the same ictus immunisatorius. Here, then, is one of the difficulties which stand in the way of our accurately forecasting the effect of the inoculation of a bacterial vaccine.
"It is a difficulty which can be circumvented only by directly controlling the effect of the vaccine upon the patient. More formidable is the difficulty which is created by the fact that there is not, as is clearly shown in connexion with preventive inoculation against typhoid fever, any constancy in the immunising response of healthy men to one and the same dose of one and the same vaccine.
" And greater than all is the difficulty which is created by the fact that there are very great differences produced by one and the same dose of vaccine in the infected as compared with the healthy, and in the severely infected as compared with the lightly infected. For this reason it is impossible to foresee accurately the effect which a vaccine will produce when inoculated into an untried patient.
" Lastly, still further difficulties arise when we are asked to predict, instead of the result of an isolated inoculation, the effect of a whole series of inoculations periodically undertaken upon a patient. The difficulty of prediction here is insuperable, owing to the circumstances that, either as a result of the patient's personal factor, or as the result of the special features of his infection, the point at which he fails to respond to small immunising stimuli, and the point at which he tolerates or responds to larger immunising stimuli, are reached in the one case earlier and in the other case later."
The various conflicting theories as to the nature of " immunity " are merely based upon assumptions. These " little systems " have their day and cease to be. " Theory has succeeded theory; most of them have been but passing opinions, many have been based on the unfounded premises of incomplete research, a few bear the stamp of patient work and of careful observation." 1
1 Kanthack.
But, the commercial exploitation of suffering humanity goes on steadily. And the dream of a huge bureaucratic institution�a Ministry of Health with greatly extended powers enabling it to decree that the whole population or any section of it shall be subjected to any particular form of vaccination�may yet be realised if the public are not educated as to the facts.
Even to-day, one may, as the result of a street accident, be rushed in an ambulance to the nearest hospital, and subjected to an inoculation. Yet, the therapeutic value of anti -toxin is still a disputed question !
The persistent efforts to push the Schick test and anti-diphtheritic serum constitute one of the most disgraceful chapters in the history of medical bureaucracy.
If the authorities took half the trouble to teach the public the laws of health, the results would be far-reaching and lasting. One of the gravest dangers of so-called immunisation is that the fancied protection may lead to the neglect of personal care of health by attention to Nature's laws.
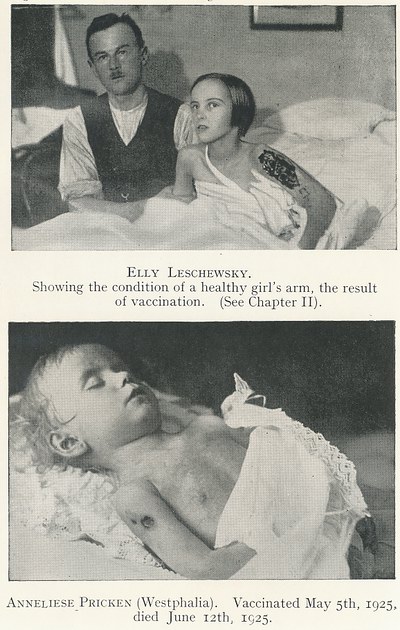
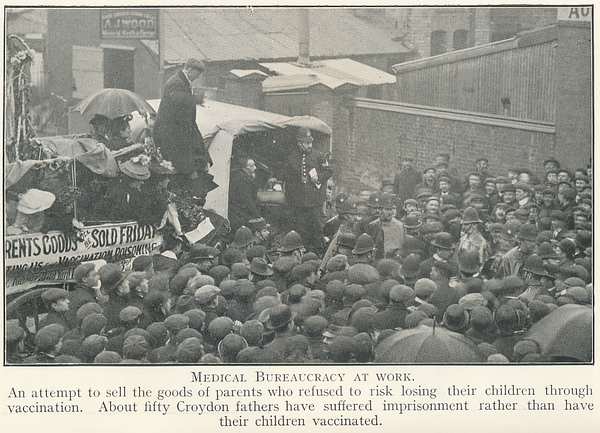
Chapter 6: THAT BLESSED WORD " RESEARCH "
" Words are, of course, the most powerful drug used by mankind."�Rudyard Kipling.
The extent to which the human mind is influenced, and in fact dominated by mere words, has been the subject of comment by more than one writer.
A word, good in itself, and good in its implication, may be misapplied to sordid and ignoble ends. Such a word is " research " !
It has been already pointed out that the example of Pasteur's success in developing laboratory research into a commercial proposition, brought into existence a host of eager imitators, and, combined with the possibilities of publicity in the guise of sensational articles in the Press, opened up an endless vista of pecuniary reward to those engaged in it.
It is no exaggeration to say that many millions of pounds have flowed from time to time into the channel indicated, and it is equally true that little, if any, real benefit to suffering humanity can be traced as a result.
It is the fashion nowadays for almost every hospital�whilst issuing piteous appeals for funds on the ground that it is on the verge of bankruptcy�to indulge in the luxury of a " laboratory," with an assorted collection of rats, mice, guinea-pigs, and (when the dog stealers have had a lucky day) a stray canine pet or two ! 1
1 Hewett, a dog stealer, was captured by Inspector Curley as he was about to
enter University College with two valuable terrier puppies which were tied up in
a sack and half suffocated. Hewett was sentenced to six months' hard labour, and
a further month for cruelty, and the Magistrate at Bow Street remarked that he
had been informed that a number of cats and dogs had been missed from the
neighbourhood near the College, and " that a cruel and unscrupulous person
supplies animals to the school." The case was dealt with on Nov. 20, 1926.
At a meeting held at the Aeolian Hall, on Jan. 19, 1927, a man named Jackson
asked to be allowed to speak, and stated that he had supplied hundreds of dogs
to the College and other laboratories.
Beds or even wards may have to be closed down, but the " path." department must have its supplies of material for experiments.
The rage for fitting out unnecessary laboratories at the public expense was recently commented upon in a medical journal:� " The provision of elaborate and expensive group laboratories which the recent Report of the London County Council declared are now being built is likely to become a heavy charge on the rates, and, according to Dr. E. Graham Little, is a wasteful duplication of existing laboratories at the voluntary hospitals. And he goes on to point out that the 17,000 beds in the L.C.C. general hospitals are predominantly filled with chronic cases�disablement from accident, old age, mental deficiency, and other incurable conditions presenting no difficulty in diagnosis, and not calling for laboratory investigation." 1
The successive stories of the wonderful results are monotonously alike. The anonymous " Medical Correspondent " of our daily newspaper is ever ready to announce another triumph of what he describes as " medical science"�the discovery by some diligent laboratory worker of a new bacillus, or the concoction of a serum or anti-toxin is heralded upon evidence that any student of logic would deride.
" Hope springs eternal in the human breast," writes the poet, and the new gospel reaches the eyes of countless sufferers who eagerly enquire of their medical advisers if the latest " boon " might be suitable to their case. Should he reply that the claims made for the new remedy have yet to be proved, the doctor is criticized as not being up-to-date. '' Many of us inoculate our patients because it is expected of us rather than because we feel it is the best way to cure them." 2
1 British Med. Jour., April 30, 1932.
2 Sir Thomas Horder.
By means of a persistent campaign the public has been led to believe that the medical practitioner of the pre-Pasteur days was au bout de son Latin, and that the laboratory chemist with his microscope, test-tubes and guinea-pigs had arrived to inaugurate a new era. As the late Sir James Mackenzie remarked :�" The public have a great belief in obscure and tortuous methods. . . . The public demand from the mysteries of medicine, what they require in the mysteries of religion, and where there is a demand there will always be those to meet it." 1
1 The Beloved Physician, p. 447.
"Research " in the medical sense has been cunningly worked as a popular " stunt," and rests upon the false notion that disease is in no way related to one's habits of life, but is something tangible and corporeal that may be exterminated in the manner of an insect pest. Hence such popular catch-words as, " The War on Cancer," " The Fight against Tuberculosis," etc., ad captandum vulgus.
Disease, as has already been pointed out, is a condition of the human body, and can be studied therein by its manifestations (symptoms), and the response made by the organism to particular treatment.
" Medicine," writes Sir Andrew McPhail, "is an art founded upon observation, with, experience alone as its guide�observation, that is with the human eye of the complete patient, and not parts of him in the form of a slide under a microscope."
The isolation or segregation of organisms which happen to be found in the tissues of a diseased animal, with a view to studying them in a laboratory under conditions which "only approximate " to natural ones ; or to proceed to base conclusions upon phenomena observed under " conditions " that " are evidently not the natural ones " is a travesty of science.
Lord Moynihan recently complained " that physiologists were neglecting research on man (' nominal research ') and were concerned too much with research on animals ; that the aloofness from medicine was increasing year by year, and that their discoveries were becoming of less use to the clinician." He singled out for particular criticism the Report of the Medical Research Council.
He characterized as amusing the assumption that ready-made weapons are fashioned in the laboratory and handed over with magisterial authority to the physician, who humbly acquiesces in their prescribed use.
As to surgery, he pointed out that the advances in knowledge of gastric and duodenal ulcer and cholelithiasis had been made by surgeons with little help from the laboratory.
Indeed, the contribution of the laboratory to the surgery of the stomach was not only almost negligible, but was potentially dangerous, because so divergent from human experience. Sir Walter Fletcher, Secretary to the Medical Research Council, resented the criticism, and a correspondence took place in the columns of the medical press in the course of which Lord Moynihan declared " Sir Walter is really incorrigible. I convict him of the grave offence of misquotation. . . . He replies not with apology or withdrawal but with a shoal of petulant irrelevancies.
" He is himself wholly unfamiliar with (and if his views are represented in the Annual Report of the Council) a little disdainful of, the activities of members of his own profession, a little too truculent over the supremacy of laboratory workers."
In his address to the students of Guy's Hospital the distinguished President of the Royal College of Surgeons said further:�
" The Medical Research Council, which might exert so magisterial and so
inspiring an influence on the progress of medicine, seems too busy with little
things, too aloof from the day-to-day practice of medicine, out of touch with
the needs and desires of clinicians.
" The truth is, and I grieve to say it, that
a grave disservice to medicine is suffered by the exaltation of the work of the
laboratory in comparison with that of the wards and operating theatres.
" The attitude of the Medical Research Council condones, if it does not
encourage, that estrangement of the physiologists from human problems, for
which, of course, it was not primarily responsible. The Council must either have
a larger representation of clinical medicine and surgery or call practitioners
to its aid in an advisory capacity.
" If physicians and surgeons are to profit in the future by the work of the
laboratory the physiologists must concern themselves more and more with human
afflictions, especially those which approximate closely to normal conditions."
The determined attempt of the new school to usurp the position hitherto held by the clinician is forcefully commented on by Dr. Thomas Dolan, F.R.C.S. :�" The clinical observer has been pushed on one side by the men who are supposed to be engaged purely in ' original research,' the men who work solely and simply in laboratories, who look through microscopes at infinitesimal organisms, or who apply complicated instruments to curarized frogs to measure their heart-beats, or who take up the more fashionable pursuit of bacteriology, as if the clinical observer were not equally entitled to claim that he was engaged in original research. As the consequence of fashion we have a vast literature of the modern school, but unfortunately not valuable in proportion to its vastness. It is a mass of undigested, crude material, produced in accordance with the wants of the market. Theories have been started based on imperfect experiment. Bacteriological research being encouraged by endowments and by the fashion of the day, naturally has thrived."
It is a striking phenomenon in relation to " research " that the conclusions of laboratory workers are accepted ex cathedra, as being above criticism. Dr. Erwin Liek, a Dantzig surgeon, makes reference to a monograph by a young " scientist " who " asserted and tried to prove that he had succeeded in replacing the natural circulation of the blood of the kidney by an artificial collateral circulation. His discovery would have been of value because it would have enabled us to operate on the kidney while tying up the artery, and thus providing the kidney with blood without endangering the life of the patient. I found that the man had completely misled me. There was not a word of truth in his statements. His experiments had been inadequate and he had drawn from these inadequate experiments illogical and absurd conclusions. Yet this useless and worthless publication secured to the writer official recognition and an appointment at the Berlin University." 1
1 The Doctor's Mission
It would require a lengthy chapter to make even a passing reference to the various claims made from time to time of " discoveries " by research workers. A few typical cases may, however, be referred to.
Insulin will be dealt with in Chapter 15. The latest figures from Toronto itself are conclusive evidence of its failure. A Sunday newspaper startled its readers by stating that a " man with only a year to live " was, thanks to the generosity of the proprietors, to be placed under the treatment of a Dutch doctor who claimed to have at last found a cure for cancer. The whole thing appears to have proved " a nine days' wonder," for the doctor's remedy was put to some sort of test in England, and after that the affair appears to have fizzled out.
In commenting upon this matter, the Lancet remarked : " although the preliminary results were encouraging, subsequent enquiries have failed to justify the early promise. The investigating Committee, therefore, has come to the conclusion that the Bendien method of diagnosis for malignant disease cannot be accepted as reliable."
Another well-advertised discovery was that of a Miss Chevassut who claimed to have found the " spherule " of disseminated sclerosis�an organic affection of the brain and spinal cord. Early in 1931, the Halley-Stewart Trust somewhat prematurely provided the funds necessary for the equipment of a Laboratory and Nursing Home at 20, Chesterton Gardens, Hampstead. Provision was made for a nursing staff and accommodation for twelve patients, and Dr. B. H. Stewart was appointed as medical superintendent.
From April to Sept., 1931, 116 patients were treated. Sixty-nine of these were readmitted, thus giving opportunities for observing the results.
According to an analysis drawn, up by the medical assistant:�
27 cases were definitely worse.
25 showed no change of condition.
13 showed slight improvement.
4 showed considerable improvement.
In commenting on these figures, Dr. F. M. R. Walshe states :�" I may say with confidence these results are markedly worse than hospital records would show for the treatment on other lines of disseminated sclerosis, and also are not so good as a similar number of untreated cases would probably show, I can only conclude from your figures that the treatment you have been investigating must aggravate the malady, and that the patients so treated are worse off than if they had been left alone."
Miss Chevassut had described a successful cultivation of the " specific organism " and claimed that it could be regularly maintained in " sub-cultures." She failed, however, to comply with the request of the three specially appointed pathological experts that she would give them an opportunity of examining and verifying her detailed description for themselves.
In 1913 and 1914 Prof. Stockhard published results of experiments on the effect upon fertility of the daily administration of alcohol in quantities large enough to produce sensible intoxication, but not otherwise to impair the health of the parents. The experiments were made upon guinea-pigs.
His conclusions were that there was a fall in the number of births, an increased liability to still-births, and the production of weakly and defective offspring. Moreover, these tendencies appeared to be inherited and to suggest that alcohol in the circulation could injure the germ plasm and bring about a permanent degeneration of the race.
Miss Durham, seventeen years later, using a specially chosen stock of guinea-pigs has repeated "exactly Prof. Stockhard's experiments and the results were statistically analysed but no confirmation was found of single essential point of Stockhard's findings.
Chapter 7: "DEMORALIZED RESEARCH"
" To mistake inferences or axioms for facts has been a curse of science."�Sir Clifford Aixbutt, in Nature.
The Medical Officer of Health for Hudders-field has stated :�" Rightly or wrongly, I have long held firmly to the opinion that research is badly overdone," and he further mentioned that he believed that in 1887 a London hospital was given �300,000 for cancer research�the equivalent of an endowment of �15,000 per annum ! He describes the results of cancer research as "a minus quantity."
After a quarter of a century of experimentation by the Imperial Cancer Research Fund " it has still to be confessed that we are ignorant of the cause of the disease." l
1 British Med. Jour., Feb. 5, 19271
It is a sad reflection upon the credulity of the public that, after a series of uninterrupted failures extending over a period of a quarter of a century, the slogan " Cancer Research " should be still successfully exploited.
A glance at the figures showing the number of experiments (many of them involving revolting cruelty) on the one hand, and the alarming increase in the death-rate on the other, ought to convince any one with a modicum of intelligence that these vast sums of money are being thrown away.
| Experiments for Cancer Research in England (official Returns.) | Deaths from Cancer per 1,000,000 of population�as shown by Registrar- General. | ||
| 1904 I904 879 1905 I2,l87 I9O5 889 1906 21,082 I906 922 . I907 40,032 1907 915 1908 40,870 I9O8 93I 1909 45,l82 I9O9 962 1910 49,662 I9IO 967 1911 41,025 I9II 992 1912 24,870 1912 1,023 1913 26,269 I913 1,064 1914 22,371 1914 1,069 1915 11,657 i9I5 IJ2I 1916 7,624 1916 1,166 1917 6,231 1917 1,210 1918 6,027 I9I8 1,218 1919 7,644 1919 1,145 1920 6,136 1920 1,161 1921 7.359 X92i 1,215 1922 13,146 1922 1,229 1923 14,081 1923 1,267 1924 8,083 1924 1,297 1925 12,623 1925 1,336 1926 15,167 1926 1,362 1927 15,275 1927 1,376 1928 34,180 1928 1,425 1929 20,098 1929 1,437 1930 25,259 1930 1,454 |
8,292 | ||
The futility of the experiments is apparent and it is certain that had a small proportion of the time and money thus wasted been devoted to investigating the effects of habits of life (and particularly diet) in causing cancer in human beings, conclusions of practical value would have been reached. This view is shared by men eminent in the surgical profession. Thus, Prof. Hastings Gilford (formerly Hunterian Professor, Royal College of Surgeons) remarks :�" I do not believe anyone who does this with an open mind can come to any other conclusion than that to search for the cause or cure of cancer by means of experiments on lower animals is useless. Time and money are spent in vain.
" Laboratory cancer research having proved a failure and operative treatment but a limited success, we see no hope of deliverance except in measures of prevention. And in this direction there is very lively hope. A century ago cholera and typhoid fever were regarded with as much terror as cancer is to-day. Yet though we have never been able to find a cure for either of these diseases we have completely rid ourselves of the one and are rapidly getting rid of the other . . .
" Inquiries into the cause of the prevalence of cancer in some countries and of its rarity in others seem much more likely to provide us with ways of prevention than our present methods of studying debatable forms of tumours grown by artificial means in the bodies of inferior animals."
And, more recently,1 he added :�" That the research into the cause and nature of cancer is making no headway is obvious to everyone who has followed the drift ever since the movement began with the beginning of this century. And now, after thirty years of research all that it has to show is a prodigious heap of facts and deductions got by much industry from animal sources, but, so far as man is concerned, no better than a tumour� an innocent tumour�no use to man and most decidedly of no use to mice." ..." And now, after a quarter of a century of research, we see to what a deplorable waste of energy and ability and money this academic, aimless toil may lead."
1 Oct. 25, 1930
Sir William Arbuthnot Lane writes1 :� " To show how little use Medical Research has been in this direction (controlling and curing cancer) one need only call attention to the fact that within the last three years, an important research body, confirmed by eminent medical opinion, stated that food has nothing to do with cancer, that cancer came like a bolt from the blue. The unfortunate factor in all professions is that, in proportion as one develops a special sense, one loses one's common sense. It is now dawning upon the profession that, while the use of drugs and operations is essential in the treatment of disease, it is the pre-eminent duty of the profession to study health, to observe its reaction to diet, and to educate the public in the simple laws of Health. Prevention is the duty of the Medical Profession and its study has unfortunately been hopelessly neglected. . . . That all the diseases of civilization from pyorrhoea to cancer, are due to errors in diet is absolutely certain."
1 Sunday Express, Dec. 27, 1931.
Sir William turns from the laboratory to the kitchen :�" The foundation of cancer is laid in the kitchen and in the dining-room, and women have it in their power to limit its ravages and even to eliminate it altogether." This, at least, is a message of hope, as against the message of despair contained in Voronoff's caustic comment:�" In your country you spend thousands of pounds every year on cancer research, but your scientist experiments with rats, and if ever a cancer cure is found in that manner, it will cure cancer in rats, but not in human beings."
Among other deplorable results of the Health Insurance Act was the control of a
sum of about three thousand pounds per week by the Medical Research Council. The
ineptitude of this body was demonstrated by their allocation of large sums to
Dr. and Mrs. Mellanby during the past ten years. It has issued at the public
expense a series of pamphlets purporting to convey information as to the results
of experiments upon puppies, and inferences drawn therefrom respecting the
feeding of children ! These experiments are said to throw light upon the
etiology of disorders such as rickets, scurvy and dental caries, and though they
have been written up in the lay press, they have failed to impress the more
intelligent section of the profession. It was claimed that Mrs. Mellanby's
experiments proved the importance of Vitamin D, and Prof. Mellanby suggested to
the British Medical Association that the expenditure of a few thousand pounds
would provide yearly sufficient Vitamin D to ensure the perfect
formation of the teeth of every member of the community, if given from, or
before birth.1
It seems an extraordinary thing that a carnivorous animal�the dog, should be selected for the purpose of demonstrating the effect upon human beings of special feeding, and it led to the patent error that oatmeal is not suitable as a food for children, though generations of Scotsmen�big-boned, brawny and brainy�have been reared from infancy almost exclusively upon the national food in days before " vitamins " were heard of.a The chemical processes in the body of a flesh-eating animal differ radically from those of a frugivorous animal. Much of Mrs. Mellanby's time, much public money, and much acute suffering to the unfortunate puppies might have been saved if some one had pointed this out beforehand. (See Appendix 6.)
" As regards experiments devised to show the influence of different diets on the resisting power of the teeth to caries, I am frankly mistrustful of them, so great are the opportunities they afford for error." 3
1 Hastings Lecture, March, 1931.
2 Addressing a meeting of the London Associated Medical Women's Federation, Mrs.
Mellanby stated that, in the feeding of children, if oatmeal was the cereal
taken a large quantity of Vitamin D must be taken to counteract it.
Asked which type of cereal was the best for the growing child Mrs. Mellanby
recommended rice and white flour \
3 Dr. Harry Campbell, Brit. Med. Jour., Mar. 12, 1932
Curiously enough, an investigation under the aegis of the Medical Research Council led to conclusions opposite to those of the Mellanbys.1 But these latter conclusions are based more soundly upon observations on children.
" It would be interesting to know," remarks Dr. Sim Wallace, " if this august Council has ever considered how much its methods and work have demoralized research, and degraded the medical profession in the estimation of those who view it from a detached and philosophical standpoint." 2
In connection with Vitamins it has been impudently claimed that modern research has resulted in the discovery that cod-liver oil is valuable in rickets whereas in the early years of this century, most writers considered its use disadvantageous in the treatment of this disorder. The value of cod-liver oil was recognized by clinical observation before Mrs. Mellanby was born. In a Text Book of Medicine (Fagge and Pye-Smith, 1901) it is stated that, " among medicines the most valuable is cod-liver oil." Hare's System of Practical Therapeutics (2nd ed., vol. ii, p. 236) states�" Cod-liver oil is the most important agent."
1 The Lancet, Dec. 5, 1931.
2 Presidential Address to the Society of Medical Officers of Health (Dental
Officers' Group).
Dr. Thursfield wrote to the British Medical Journal with reference to a misleading article which had appeared :�" You go on to stress the great advance which the experimental work on rickets has made in the treatment of that disease . . . the clinical facts are against that assumption. Rickets, as we workers knew it in 1890-1900 period, began to disappear in the 1900-1910 period, and after 1910 severe rickets was becoming as rare a disease as it is to-day."
Many persons have been seriously perturbed by revelations as to experimentation upon young children�a logical corollary to experiments upon other animals.
A glaring instance was that of Dr. Samuel McC. Hamill as reported in his own words in the Archives of Internal Medicine.1 He, with two other U.S. physicians, carried out experiments on 160 children to determine the best method of applying the so-called tuberculin " test." The unfortunate infants were all under eight years of age, and Dr. Hamill relates how he managed to get 134 of these little victims in his clutches : "I went with Dr. -----to Sister Marie, the Sister Superior of St. Vincent's Home, and we together explained to her that we wished to apply these tests for the double purpose of deter-
1 Dec. 15, 1908.
mining the incidence of tuberculosis among the cases in St. Vincent's Home and among those being admitted to the home, and at the same time to make a comparative study of the different tests. We were granted permission without any hesitation and the work was conducted throughout my term of service without the slightest comment on the part of anyone. But it was applied only to children in the home at that time. When I returned from my vacation in the autumn I prepared to apply the tests to children who were being admitted to the home but gave this up after hearing from Dr. ------ that there had been some criticism on the part of the Sisters of the work which had been done."
In other words, the terrible sufferings of these little children so touched the
hearts of the Sisters, and aroused such adverse comments that the doctors dared
not continue. The " tests " are as follow :�
(1) The placing of a drop of the irritating fluid in the eye�the conjunctival
test.
(2) von Pirquet's method. Scraping the skin and applying the tuberculin to the
raw area.
(3) In this (Moro's) method an ointment containing tuberculin is rubbed into the
skin.
(4) The tuberculin is injected under the skin.
Of No. 1 the researchers state : "It has the great disadvantage of producing a decidedly uncomfortable lesion, and it is not infrequently followed by serious inflammation of the eye, which not only produce great physical discomfort and require weeks of active treatment, but which may permanently affect the vision and even lead to its complete destruction." No less than 152 of the children were subjected to this cruel process, which, on the admission of their torturers, " has no justification in medicine."
Dr. L. Emmett Holt of Columbia University carried out and reported on no less than 615 similar experiments on young children, " some of whom were dying or extremely sick." Adverse criticism was aroused and the New York Evening Post deprecated the fact that such charges should be made against a physician of Dr. Holt's standing. On further investigation, however, the Post 1 made the following comments :�" It appears in Dr. Holt's own article in the Archives of Pediatrics for Jan., 1909, that he did use the tuberculin test with ' dying children or those suffering from extreme prostration '�to use his own words. The majority of the one thousand cases treated by Dr. Holt were ' under two years of age.' At the same time that these experiments were being conducted, three physicians of standing, as set forth in the Archives of Medicine of Dec, 1908, declared that this tuberculin diagnostic procedure ' which will so frequently result in serious lesions of the eye, has no justification in medicine.' With this we close discussion of this unhappy incident; we leave to the medical profession the question whether, in the near future, experiments of this kind upon dying children shall not be tabooed."
1 April 17, 1914.
Dr. A. H. Wentworth reported in the Boston Medical and Surgical Journal that, on more than forty occasions, he tapped experimentally the spinal canal of infants whose symptoms presented no indication for such a surgical procedure. In commenting upon this the Philadelphia Polyclinic1 remarks :� " The account of the action of this man�we dislike to call him a physician�is enough to justify the prejudice against hospitals which we find deeply rooted among the poor, and constantly combat as ignorant and superstitious. He does not tell us definitely whence the patients came ; but they apparently were hospital inmates, whom he was supposed and professionally bound to treat with humanity and skill."
1 Sept. 5, 1896.
The publicity given to these facts seems to have resulted in Dr. Wentworth losing his position at the Children's Hospital, but, some years later his name appeared as a member of the Massachusetts Medical Society (affiliated with the American Medical Association). The following is an extract from the Journal of the American Medical Association,1 and has reference to similar experiments on new-born babes by Dr. M. Hines Roberts :�" I was in doubt as to the true nature of the normal spinal fluid immediately after birth, and for this reason attention has been focused with equal interest on normal as well as on pathological specimens.
1 August 15, 1925
" A total of 423 babies has been studied. A lumbar juncture was done on every infant without regard to the character of labour or the condition of the child at birth."
If one might anticipate a comment that some of these experiments were done by American medical men, two things should be said, viz., that as the chapter on diphtheria proves, experiments are made upon British children, and it is not to be supposed for a moment that the American Medical Association would admit that its standard of ethics is lower than that of the British medical profession.
Chapter 8: TUBERCULOSIS: KOCH AND HIS IMITATORS
" It is the over-crowded dwellings of the poor that we have to regard as the real breeding places of consumption ; it is out of them that the disease always crops up ; and it is to the abolition of these conditions that we must first and foremost direct our attention if we wish to attach the evil at its root and wage war against it with effective weapons."�Prof. Dr. Koch.
There is a remarkable family likeness in the methods by which the products of the " research " laboratories are foisted upon a confiding and unsophisticated public.
A disorder is usually selected that at some period more or less remote could be referred to as a " scourge" the successful treatment of which was hitherto beyond the scope of medical art.
It is, however, almost a sine qua non that, thanks to improved sanitation, better housing or feeding, or changed methods of registration, the death-rate shall have materially fallen, and be still on the decline. The dice are thus loaded in favour of almost any new treatment, good, bad or indifferent, as the unsuspecting public is told to note what a marked decrease in the death-rate has taken place concurrently with the introduction of the new nostrum.
It was quite appropriate, therefore, that, at a time when the incidence of tuberculosis showed a decline of something like 50 per cent.,1 an announcement should be made to the effect that Koch, who, eight years previously, had isolated the bacillus which he declared to be the cause of tuberculosis,2 had discovered a means of destroying this organism in the human body, and thus curing consumption.
1 " The disease is dying a natural death with improved conditions of the working
classes, and it is by further developments on such lines, and not otherwise,
that its extermination will be attained."�Dr. T. D. Lister (Mount Vernon
Hospital for Consumption, Hampstead).
2 Although the use of tuberculin was originally based upon the tubercle bacillus
being the causa causans of tuberculosis, Dr. Coplans, the London representative
of the Pasteur Institute, stated at Leeds (in 1926) that " the bacillus was, it
was now known, not the only cause of the disease."
In the Philadelphia Public Ledger (Sept. 4, 1928), Prof. R. J. Anderson of Yale
University announced the discovery that " one of the outstanding signs of
tuberculosis, the tubercle, is generated in rabbits by a purely chemical
product." The fact that the injection of foreign proteids may cause tubercles
had been proved by Metchnikoff, H. Martin, Wooldridge, Schmorl, Rocht, etc.
(Pulmonary Tuberculosis, Muthu). Even " normal guinea-pigs have been found with
tubercle bacilli in the lymph nodes " according to Cooper and Petrofi (British
Med. Jour., Feb. 15, 1930).
Referring to the reduced death-rate from Tuberculosis, Dr. Alexander James
pointed out (Scotsman, June 6, 1916) that the improvement showed itself years
before the bacillus had been discovered, and years before isolation and crusades
against infection had been thought of.
Mr. Muirhead Little has shown that tuberculosis was understood before the discovery of the bacillus, and his historical survey is another demonstration of how keen was the clinical sense of many of the early observers.1 It would be difficult to put one's finger on any chapter in the history of medicine marked by such medical ineptitude on the one hand, or public credulity on the other.
The be-spectacled features of the Berlin professor had hardly become familiar to the world by means of the innumerable press clich�s when the whole edifice collapsed like a house of cards, and the commercial interests to whom such enormous profits were to have accrued received an unpleasant set-back.
An astute writer2 commenting on the fiasco, remarked :�" What could have led sober and staid men to believe that a disease like pulmonary consumption could be cured from the results of one set of laboratory experiments is simply impossible to say, and the more impossible now that the facts are better known. Couple with this rush and excitement the wild demands for the 'lymph,' the collection of the afflicted from all sources to exhibit them under experiment with a remedy the nature and action of which were unknown ; couple with these the mortality and the violence of symptoms springing from the undeclared nostrum; add to all the miseries of the unhappy sufferers who, misled largely by false medical enthusiasm, left the known, if poor, paths of medicine by which they could be conducted towards recovery, to have their means reduced, their fond hopes dispelled, and in some instances, their short days shortened and who shall calculate all the mischief that has been accomplished in this one paroxysm of hasty judgment and hasty generalization ? '' Referring to the lame apology that, after all tuberculin might help in the diagnosis of tubercular disease, the same authority remarks " Would that such an apology had been writ in the water in which it was conceived and no more. There is nothing in which the accomplished physician is more accomplished than in the detection of tuberculosis. Even a student who could not at his ' final' make the diagnosis would stand a good chance of being plucked."
1 Brit. Med. Jour., Feb. 15, 1930.
2 Sir Benjamin Ward Richardson, M.D,, F.R.S.
The story of this tragedy was thus told in the Lancet some years ago in the report of a lecture on " Forty Years in the History of Tuberculosis " :
" In 1890 Koch introduced the subcutaneous injection of tuberculin as a specific immunising agent against tuberculosis. It is not surprising that the new method, ushered in with such excellent credentials, excited the liveliest interest in all civilised countries, and the hope was freely expressed that now at last one of the greatest scourges of the human race would be brought under control. The commotion aroused in the medical world was incredible. Nothing like it had been seen since the South Sea Bubble in 1720. A veritable stampede to Berlin ensued, doctors and patients nocking in frantic haste from all quarters of the globe to the new Pool of Siloam. At first only a limited quantity of tuberculin was available for foreign use, and this was entrusted to a favoured few. Observers in all countries had no difficulty in convincing themselves that tuberculin had a powerful effect on tuberculous subjects. But when in accordance with Koch's instructions the dose of tuberculin was gradually increased, constitutional symptoms of a severe nature were frequently excited, with fatal results in many instances.
" In a comparatively short time the failure of tuberculin treatment had to be reluctantly admitted and Koch's method of administration was virtually abandoned."
Although the writers on medical subjects in the Encyclopedia Britannica manifest a�perhaps, unconscious�bias in favour of all that pertains to laboratory research, Dr. Allen K. Krause has little to say for tuberculin.
"Even specific treatment," he writes, "aiming at the production of immunity, while helpful in certain patients, has proved disappointing. Tuberculin in its various forms is no longer regarded as a ' cure in the strict sense of the term,' and is not entirely free from risk, the natural power of the human body to amplify its powers of resistance is very great, and many cases do well if placed under favourable conditions of life."
Koch's original tuberculin was prepared by growing " cultures " of tubercle bacilli in a special broth for several weeks, a concentrate of this being filtered through porous porcelain. The poisonous brown fluid resulting was then ready for use !
One might have anticipated that, after the ghastly results which had followed the use of this horrible concoction, everyone concerned would hide his diminished head, and whatever stock was left over would have been poured down the nearest drain !
But those commercial interests already referred to had to be reckoned with, and, instead of trying to forget it, like a bad dream, Koch introduced a " new Tuberculin ' R ' " or residual�the idea being to allow the solid material time to deposit itself, thus diminishing its noxious properties, at least to some degree.
Tuberculin B.E. (Bacillary Emulsion) is a still later product. The comment in the Encyclopedia Britannica above quoted, applies to all three varieties, they can no longer be considered as a cure, whilst their use is not free from risk.
Dr. F. G. Lyon 1 in the Hunterian Oration (1912) remarked :�" Since the original Tuberculin failed to establish itself as a remedy, other preparations derived from the bacillus have been put forward. I cannot find that any greater success has attended them. Tuberculin had proved in the words of the Royal Commission ' a vast failure as far as the treatment was concerned."'
A well-known text-book 2 in speaking of the effects of tuberculin, states that no effect follows if it is injected into a healthy person, " but if he has a tubercular disease the injection produces a high temperature, rigors, pains in the joints, sometimes albuminuria and rashes on the skin, and at the same time the tubercular lesion is stimulated to activity.
" These dangerous results forbid the use of tuberculin for man."
1 Senior Physician to the City of London Hospital for Diseases of the Chest.
2 Hale White's Materia Medica, 19th ed,, pp. 695-6.
Referring to Koch's later preparations, the same authority remarks :�" Neither has been proved to have a beneficial therapeutic effect in tubercular disease, but it is now considered that either may be useful for chronic varieties ; but they can hardly be said to have proved this. Many think tuberculin often does harm."
Dr. Muthu declares :�" The experience of medical men gathered from many sources goes to show that tuberculin injection has no specific value in the treatment of tuberculosis," and he quotes the Medical Research Committee which, having investigated results covering a period of twelve years, found that the evidence for the value of tuberculin treatment is completely negative.1
1 Pulmonary Tuberculosis, p, 184.
The Manchester Guardian (June 24, 1916) comments on the decision of the Hull and East Riding Convalescent Home to abandon (after eighteen months experiment) the use of tuberculin " because its disadvantages have been found to outweigh its benefits."
The Ventnor Hospital for Consumption had already found tuberculin fail in the 300 cases upon which it was carefully tested. It lengthened treatment, diminished ability to do work, injured nutrition and left the after results more unfavourable.
" In my own experiences," writes Dr. H. G. Adamson, " in every case of lupus treated by tuberculin, the disease has subsequently become less controllable than before the treatment was used." 1
Many other eminent medical authorities might be quoted�including such names as Bardswell Thompson, Batty Shaw, H. G. Adamson, Sir James Fowler, F. G. Chandler, etc.
One might have thought that the effect of such an avalanche of adverse criticism would have deterred anyone from further attempting to foist tuberculin or any colourable imitation of it on the market. But the commercial mind is not easily discouraged, and the moving force behind the serum business partakes much more of the commercial than of the scientific !
It is not surprising therefore that Koch should have had a host of imitators�a comprehensive list will be found in Stedman's Medical Dictionary�or that when beaten back upon the use of tuberculin for human beings it should have been pushed as a " test " for cattle ! 2
1 The Lancet, Aug. 10, 1918,
2 Koch denied that the bovine form of the bacillus caused tuberculosis in man
(International Medical Congress, 1900). A Royal Commission on Tuberculosis was
appointed which sat for ten years with a net expenditure of �75,557, and
published an elaborate report to the effect that man is infectible by the bovine bacillus,
Prof. Koch notwithstanding.
" It is strange,' comments Sir W. Osler, " how he (Koch) still sticks to his
views in spite of all the overwhelming evidence against him."�Life of Osler,
Harvey Cushing.
The extent to which the so-called " tuberculin test " has been advertised both in this and other countries only goes to show how easily the authorities and the public may be hoodwinked by men who know their business.
For it is a remarkable fact that, although the tuberculin test may prove the existence of infection (just as in human beings it has the effect of stirring into activity existing though dormant, tuberculous lesions), it gives no indication as to the degree of the infection; emaciated, heavily infected animals may fail to react at all.1
l Encyl. Britannica. XIV Edition.
" The so-called vaccination of Calmette is criminal charlatanism which kills our children."�Prof. Kuelz.
When a reputable tradesman introduces an article which fails to achieve all that he claimed for it, he withdraws it from the market. Unhappily, this is not the attitude of those associated with the serum and antitoxin industry. The prospects of gain are so vast that neither the most convincing evidence of the uselessness and danger of such products, nor the series of disasters following their administration exercises any deterrent influence on those who pursue this business.
The ghastly failure of Koch's original tuberculin should have acted as a warning and checked any similar enterprises. But whilst Koch's failure afforded abundant proof of the dangers of inoculation it simultaneously opened the eyes of the bacteriologists to its enormous commercial possibilities. So Koch's discredited tuberculin was followed by Tuberculin Residual, that by Tuberculin O. and T.B. Emulsion, and these in turn by T.A.; Behring's Tuberculase; Bereneck's T.; Buchner's T. ; Denys' T. ; Endotin ; Hirsch-field's T. ; Klebs' T. ; Klemperer's T. ; Landmann's T.; Maragliano's T.; Rosen-bach's T.; Ruck's T.; Splenger's T.; etc.1
1 See Sledman's Medical Dictionary
Finally, there are Spahlinger and Calmette. The former treatment has had a somewhat chequered career commercially ; but�sponsored by Sir Bruce Bruce Porter�an attempt has been recently made to bring it into favour. At a specially convened meeting consisting principally of journalists, Sir Bruce Bruce Porter stated that Spahlinger " grew the tubercle bacilli for the purposes of the vaccine under environments of food, heat, etc., which were identical with those found in the particular body wherein the microbes were creating disease," by which he means, presumably, the human body. One would like to ask Sir Bruce Bruce Porter what environment other than the human body could be properly described as being identical with it.
" He later placed them," we are informed, " under such conditions that they died a natural death." Again one would like the conditions defined under which the tubercle-bacillus dies a natural death. " They thus retain unimpaired the chemical and physical structure by which they are effective vaccinating agents," the eminent physician proceeds to inform us. Verily, there is much truth in the remark of Sir Clifford AUbutt that " medical discourse and medical literature are pervaded by assumptions."
Yet, although Sir Bruce Bruce Porter is lending his valuable aid as publicity agent, and a group of philanthropists have been persuaded to give financial support to the Spahlinger serum, " there is, at the moment, no published evidence to indicate that the method rests on any firmer basis than that of empiricism. Incidentally, it may be remarked that the method of vaccination put forward by M. Spahlinger is almost directly opposed in principle to the method of vaccination with B.C.G. put forward by Prof. Calmette, and it is very difficult to imagine if the principles upon which they are respectively based are correct, how both of them could be effective."1
1 British Med. Jour., Feb. 13, 1932.
As Dr. Robert Carswell drily remarks, " It remains to invite the evidence upon which the claim is founded " (Brit. Med. Jour., Feb.13. 1932).
Sir Frederick Menzies recently submitted a Report on the Spahlinger formula; to the Central Public Health Committee of the London County Council in which he stated that, although Spahlinger claimed that he had disclosed full details of the method of preparation, the fact remained that so much information of fundamental importance was missing that no two competent bacteriologists working independently upon his formula would be the least likely to produce identical preparations.1
1 British Med. Jour., May 14, 1932.
Some few years ago the Daily Express made an offer to Spahlinger of �10,000 on condition that he allowed a small medical committee to examine and report on his treatment, but this offer was not accepted. It has been stated that the fortune of the Spahlinger family approximating to �100,000 has been lost in the course of his " researches," but, when matters were investigated by a commissioner sent to Geneva by the Daily Express, it was reported that a considerable sum had been lost by speculations in a motor factory, and in an hotel at Trouville. Nearly all patients treated by Spahlinger are said to have contributed a sum of �500 to the " cause," whilst Sir Stanley Birkin handed over �20,000 in gratitude for " cure " of his daughter, which was followed shortly afterwards by this young lady's death ! In two years a sum of �46,500 is said to have been contributed to Spahlinger's funds.
The personnel of the Institute consisted of his mother, his wife, a typist, an English mechanic, an English architect, a Press agent, a school friend and two male assistants, none of whom possessed any medical knowledge.
That Press agent seems to have been an inspiration !
The exploitation of immunization against tuberculosis has taken such a hold of the imagination of the " research" worker in search of fame and fortune that no considerations deter him from the pursuit of his goal. The appalling tragedy of Liibeck when seventy-six infants were killed by Calmette's B.C.G.,1 created a tremendous sensation at the time, but, instead of Calmette and his colleagues of the Pasteur Institute being put in the dock, two less responsible persons, Prof. Deycke and Dr. Aldstsedt, were sentenced respectively to imprisonment for two years and fifteen months.
1 In the finding of the Court sixty-eight out of the seventy-six deaths were manslaughter " definitely due to the treatment they had been given against tuberculosis," whilst of the 168 children who were seriously ill, 131 " definitely owed their illness to the treatment.'' Ninety-seven per cent, of the dead children had developed active tuberculous lesions in the intestine, the periods between the administration of B.C.G. and their deaths varying from nine weeks to thirty-four weeks. The conclusion that B.C.G. actually sets up tuberculosis appears inescapable.
The detached attitude of Calmette, both with regard to the disaster and the trial which followed, was characteristic. Apparently, in his view, under no conceivable circumstances can B.C.G. as supplied by the Pasteur Institute be held responsible for the deaths of these infants. Yet, but for this deadly concoction, every one of them might be to-day nestling in its mother's arms.
One of Calmette's principal contentions has always been that for some days after birth the mucosa of the small intestine is abnormally permeable, allowing tubercle to pass through and reach the mesenteric glands. Upon this hypothesis he urges that B.C.G. should be administered to infants by the mouth during the first ten days after birth. But, as the British Medical Journal points out, his hypothesis is not proved. If, however, he is right it affords an explanation of the apparently favourable results claimed for infants treated with B.C.G., for these infants are carefully segregated and protected from the ordinary risks of infection to which other infants are exposed. Prof. Neufeld, of Berlin, in dealing with Calmette's claim that the deaths from all causes are less in infants treated with B.C.G., suggests that a selection of the healthier and stronger infants is made.
What can hardly fail to impress the casual observer as an iniquitous element in the Calmette campaign is the callous obstinacy with which those interested in the sale of " B.C.G." refuse to admit its failure, or to take warning from the tragic results which have followed its use.
" There have been numerous accidents," writes Dr. Jean Bachelier,1 " but M. Calmette has been in no hurry to throw light on these unhappy cases. He has systematically ignored them."
Dr. Bachelier mentions six cases of death from following the Calmette treatment at the Baudeloque Hospital (Paris), and four cases where children of healthy parents so treated developed tuberculous suppuration of fingers, tubercular disease of the spine, etc.
The treatment was commenced in 1921, and the number of adverse reports from various quarters should have sufficed to give pause to its promoters. The so-called vaccination " of Calmette," says Prof. Kuelz, " is criminal charlatanism which kills our children." 2
1 Le XXe Siecle, Aug., 1930.
2 Biologische Heilkunst, No.
21, 1930
The following extract is from Dr. Bachelier's article (already referred to) :�
" Professor Bessau, of the University of Leipzig, rejected vaccination with B.C.G. on account of its virulence. Professor Dr. Gins, according to the Berliner Tageblatt of May 25th, 1930, declared that vaccination with B.G.G. is dangerous, and that there was already a report of the death of three children injected with B.C.G. in Berlin. Professor Schlossmann of Dusseldorf, published in a Dresden paper in May, 1930, a statement to the effect that all the experiments made on many monkeys at Dusseldorf, and carried out absolutely in accordance with the directions of Calmette, proved that the B.C.G, is without the least value, all the monkeys vaccinated with B.C.G. having died of tuberculosis.
" Stadtmedizinalrat Schmincke, of Berlin, declared on the 25th May, 1930, that the bacilli B.C.G. are without value, virulent and dangerous. Professor Kolle, of Frankfurt-am-Main, has shown that many cultures of B,C,G., when used in laboratory experiments on animals, show a dangerous tuberculous virulence. The Hungarian Government has recently forbidden for all Hungary the use of B.C.G. Professor E. von Hutyra, Director of the Veterinary Institute of the University of Budapest, has produced in young guinea-pigs a progressive and fatal tuberculosis through the injection of B.C.G. This tuberculosis reproduced itself to the eleventh generation of guinea-pigs.
" Drs. Debarge and Girod, of Geneva, published in 1927 (Rev. Med, Suisse rom.) the death of a child from tubercular enteritis twenty-five days after Calmette vaccination. Drs. Berger, Hunziker and Staehelin, of Zurich, published in 1928 (Schweiz-Med. Wochenschrift) eleven cases of children vaccinated, of which five became ill with tuberculosis of glands, of skin, and of bones."
Reports of prominent physicians led Nagel-schmidt of Berlin to the conclusion that B.C.G. was dangerous.
Eminent Austrian specialists in tuberculosis and children's diseases, including Nobel, Rosenfeld, Gotzl, and Moll discarded it as a remedy, whilst Pirquet, writing in the Vienna Medical Weekly,1 declared :�" The tubercle bacillus can establish itself in the organism through the Calmette system, and the result cannot be foretold. Such a dangerous process cannot be approved of or tolerated."
1 Nov. 23, 1928
At Vienna, the Health Bureau declined to introduce Calmette's system, whilst even in France where, according to Prof. Much " the French Senate has raised these questions to a political question of prestige," and " To be against Calmette is to be against France ; " a number of doctors including Leon Tixier, F. Viola, Nobecourt, Lignieres and others have reported serious injuries.
"Calmette's statistics are incomplete," writes Prof. Lignieres, " and there is no physician or statistician in the whole world who regards them as statistics. They contain no proof of the results of his vaccination."
Both its dangers and its fallacies have been exposed by Dr. Dible, and Dr. Greenwood, late statistician to the Ministry of Health, has ably pointed out the statistical errors upon which its claims are based. Among others opposed to B.C.G. are Walgren (of Sweden), Assis and Dupont (of Brazil), and Watson (of Canada). Yet, in the teeth of all this, an active publicity campaign has been carried on, and there have actually been indications that attempts have been made to use the Health Committee of the League of Nations as a catspaw. At the Liibeck trial it was stated that French research workers have been "hunted from position to department because they told the truth concerning Cal-mette."
One may be excused for being sceptical as to the value of any treatment requiring such sinister propaganda.
Tuberculosis is a diminishing disorder1 against which�as Koch declared�the best
1 A recent Report of the Senior Medical Officer of Health for Tuberculosis gives
the following figures :�
Total Deaths. 1911 (First National Ins. Act) .. .. 53,120
1930............35.745
a reduction of about 35 per cent. !
defence is a healthy environment. No language can be too strong in condemnation of the callous, commercial exploitation of the lives of defenceless infants, no penalties inflicted upon the local doctors (who, after all, were merely accessories in the tragedy) can compensate the distressed parents for those empty cots, no swollen profits distributed in the shape of dividends by the Pasteur Institute or any similar concern 1 can justify the continuance of these Herodian enterprises. These little ones were not sick babies, but healthy children of normal parents. There was no reason why, with ordinary care, any one of them should have had tuberculosis. But it was " Big Business" to scare the Liibeck parents by means of a cunningly-conceived publicity campaign exaggerating the dangers of tuberculosis, and holding out promises of protection against its risks.2 (See Appendix 8.)
1 As an instance of the lucrative nature of this class of business, it was
stated some years ago that the Lister Institute was conducted at a cost of
^5,600 annually and that its income was �11,000.
2 It has been stated that a series of fatalities, even larger than that of
Liibeck, occurred in another town in Eastern Europe but, as the newspapers
inform us that Calmette has many powerful friends, it is not surprising if this
has been hushed up, or denied altogether.
Dr. Julius Moses (a Member of the Reichstag and Federal Health Council),
declared " The Lubeck-Calmette affair has acted like an earthquake. The
public's faith in medical science is shaken to its foundations " (quoted in
Animals' Champion).
It would seem from the following letter that other instances of the dangers attaching to the use of B.C.G. have escaped the publicity of the Lubeck disaster :�
" Your detailed account of the Liibeck Child Murder process and the role of the Calmette preventive leads me to send you some very interesting data, as yet unknown to the public, which I established in Spain in the years 1928 and 1929, and it was also in the meantime officially confirmed. The matter in question was a trial on a grand scale of vaccination with the B.C.G. preventive of Prof. Calmette which was carried out on nearly 800 infants in the Children's Home of Madrid, in the summer of 1929.
"According to an official statement of the Society of Spanish Children's Doctors, numerous deaths and most serious illnesses occurred in these try-outs of vaccination.
"An official investigatione stablished the fact that, in the course of six months, of 757 children vaccinated with the Calmette preventive, 333 became seriously ill and 164 died.
" The well-known Spanish children's doctor, Dr. Munyerro, reported to the Conference of Children's Doctors regarding these cases, which were also later put on record by the Health Ministry.
" The direct result of these sad events was the immediate inhibition by the Spanish children's doctors, of the further use of B.C.G.1" Such a highly profitable proposition as " B.C.G." is not likely to be abandoned without a strenuous effort on the part of those interested, in spite of Liibeck or a score of similar disasters.
The Pasteur Institute has just issued a publication intended to counteract the effect of the damaging records which have come to light.2
The compilation of statistics to bolster up discredited " vaccines " has almost
become a fine art, and such plausible statements as the present brochure are too
often accepted at their face value by departmental officials.
In commenting on this latest production, the British Medical Journal3 remarks
that the records of the Pasteur Institute " are not easy to summarize. Analysis
of the three most careful inquiries on human subjects yields very unsatisfactory
and unconvincing results. It appears fairly certain that, if in any district a
given number of infants are vaccinated (with 'B.C.G.') and the subsequent
mortality among them from tuberculosis is compared with that of unvaccinated
infants, a definite advantage will be found in favour of the vaccinated group.
The reason
for this is not far to seek, depending mainly on the favourable environmental
and social conditions of those selected for preventive treatment.... When,
however, care is taken to insure that the infants in the control group shall be
readily comparable with those in the vaccinated group or when suitable allowance
is made for the differences between them . . . the advantage in favour of the
vaccinated group is much less apparent."
1 Lubeck General Anzeiger, Nov. 7, 1931.
2 Vaccination preventive de la
tuberculose de I'homme et des animaux par le " B.CG."
3 July 23, 1933.
Chapter 10: DIPHTHERIA : OLD AND NEW
Printed statements are issued under the authority of Medica Officers of Health to the effect that anti-toxin inoculation is free from danger. Such statements are contrary to facts.
Amongst the more flourishing industries of modern times is the production of " anti-diphtheritic " serum. It has been estimated that a worn-out horse such as may be purchased for three or four pounds, if bled every ten days, would yield two quarts of serum on each occasion. As this precious commodity can be disposed of at about �12 per quart, the yield, even if the wretched beast lasted only three months, would represent enormous returns to the manufacturer. (See Appendix VII.) Yet this highly-profitable and sheltered industry would appear to have been built up on nothing more or less than fictitious claims. The method was first proposed by von Beh-ring, a Prussian Army officer, and was tried upon a child in a Berlin clinic in 1891, It was not generally adopted in England and Wales, however, until 1894, and it is important to keep this date in mind, as any variations in the death-rate prior to 1894 cannot be attributed to anti-diphtheritic serum.
The death-rate from diphtheria (per million living) during successive periods of
five years from 1871 should be carefully noted :�
1871-75
121 1901-05
204
1876-80
122 1906-10
154
1881-85
156 1911-15
140
1886-90
170 1916-20
143
1891-951
253
1921-25
88
1896-1900 272
Diphtheria statistics appear to indicate that this disease rises and falls,2 the death-rate varying considerably over periods of years. So far from the serum treatment having modified the death-rate, it was actually higher by about 8 per cent, during the quinquennial period following the introduction of the treatment as compared with the already high figure for the preceding five-year period. And, if we leave out the period during which the serum was brought into general use, and take the average death-rate for the twenty years before and after, we find the average rose from 142 prior to serum treatment to 192 per million after its introduction. The whole issue has been greatly (and it would seem purposely) confused by those interested in defending the serum.
1 Inoculation generally adopted 1894.
2 In The Lancet of March 1931 reference was made to the " extraordinarily severe
epidemic of diphtheria" which had recently occurred in Berlin and to " the high
case mortality in spite of large doses of anti-toxin given at an early stage."
At a meeting of the Berlin Medical Society, Prof. Friedberger derided the whole
anti-toxin legend, and attributed the apparently favourable results to the
continuation of an already declining curve. He declared that a study of a large
series of American and European statistics had disillusioned him.
After analysing the returns of diphtheria mortality for American cities, the
Journal of the American Medical Association (May 23, I931) appears to consider
it an open question whether the reductions recorded were due to the natural
fluctuations in the disease itself, or in the susceptibility of its human host,
or whether, and how far they had been influenced by such preventive measures as
toxin, anti-toxin and toxoid immunization.
The fact that there was no appreciable diminution of the death-rate after the introduction of serum would have been the deathblow to this form of treatment had it not been backed by powerful commercial interests, and the subterfuge of case-mortality introduced to distract public attention from the fact that the general death-rate from diphtheria had not been reduced.
Serum treatment had already been adversely criticized by eminent medical authorities.
Thus, Dr. Joseph Winters, Professor of Children's Diseases (Willard Parker Hospital, New York) stated :�" Some months ago I shared with my colleagues the hope that a specific against the toxins of the diphtheria bacillus had been discovered, and I regret to say that as a result of that experience, I am here to-night to speak in opposition to the anti-toxin treatment of diphtheria. My remarks will be based entirely on three weeks of daily clinical observation of the effects of the anti-toxin in 154 cases of diphtheria treated in the Willard Parker Hospital.
" In not a single case has there been the least evidence that the formation of the false membrane was checked, or that the throat was free from membrane earlier than in cases which have not been treated by anti-toxin.
"In not a single septic case has the anti-toxin made the least impression on the symptoms. The toxaemia (blood-poisoning) has not been in one instance relieved or lessened. There has been no indication in the character or frequency of the pulse, or in the general condition of the patient that a specific had been administered. At the Willard Parker Hospital in the month of December, 1894, the recoveries from laryngeal diphtheria, without anti-toxin, were about 75 per cent. This has never been equalled with the anti-toxin treatment."
So far from clarifying the position, the theory of the Klebs-Loffler bacillus as a causative factor has tended to confuse it by substituting a bacteriological for a clinical method of diagnosis.
Swabs are submitted to laboratory tests, and the diagnosis of diphtheria (negative or positive) depends not upon any of the recognized clinical signs, but upon the result of such tests:
" In 1929 there were admitted to the Birmingham City Hospitals, 2,099 cases with a diagnosis of diphtheria ; 706 (33 per cent.) presented no evidence of clinical diphtheria upon admission to hospital. In 1931 2,162 cases were similarly admitted, of which 744 (34.4 per cent.) showed no evidence of clinical diphtheria. Fully 50 per cent, of these revised cases had been sent in purely as a result of a report upon a swabbing. A considerable proportion of them proved to be Schick-negative or immune to diphtheria on admission. In the great majority the swabbing when repeated was negative or the organisms present were shown to be a virulent. Investigation of these cases�with the Schick test and with virulence tests�occupies on the average ten days, at the end of which period the patients are discharged. Meanwhile valuable beds are occupied, and the patients, especially the adults, suffer considerable social and economic inconvenience." 1
1 Brit. Med. Jour., Aug. 22, 1931
If the bacillus is found in the throat the patient is theoretically a diphtheria case. As one medical authority put it, " you may be dying of a sore throat which every doctor would pronounce one of diphtheria, but the bacteriologist will have nothing to do with you unless he finds his specific bacillus. On the other hand, if he found that bacillus in the throats of half a dozen of the healthiest of us in this room we should all be set down as diphtheria patients."
Dr. Samuel Gee (Bartholomew's Hospital) writes " for practising physicians, the main note of diphtheria is still found in the presence, not of special microbes and morbid poisons, but of false membranes upon certain mucous surfaces or upon abraded skin."
" It is no use playing with words," writes Dr. Burnet, " It is on the clinical facts that the problem ought to depend. There are found in the most typical cases of diphtheritic sore throat diphtheria bacilli possessing every degree of toxicity, and also bacilli which are not pathogenic (i.e., for the guinea-pig, since they cannot be inoculated in man). All these bacilli are called diphtheria bacilli. On the other hand, there exist non-diphtheritic affections both of the throat and nose in healthy individuals where bacilli resembling diphtheria but non-toxic are to be found."
A high degree of technical skill in bacteriology can hardly be expected of the average general practitioner, and to complicate matters the so-called diphtheria bacillus varies in form, and bacilli bearing a close resemblance to the Klebs-Loffler organism are found in healthy and non-diphtheritic sore throats and these " pseudo-diphtheria" bacilli include several varieties and species.
The bacteriologists have set up a method of diagnosis which directly conflicts with the accepted clinical indications, and rests merely upon the presence of a particular organism in the throats of healthy persons. Dr. Winters may well ask :�" I should like to know why anti-toxin is used in cases where the Klebs-Loffler bacillus is the only evidence of diphtheria when it is a well-established fact that the anti-toxin treatment has no influence on the bacillus. It persists as long in cases treated with antitoxin as it does in cases treated without it."
It may now be seen upon what false premises the claims for serum-treatment rest. The number of deaths from diphtheria did not decrease until many years after the introduction of serum but the number of cases diagnosed by the bacteriologists as diphtheritic have so swelled the sum total that the percentage of deaths is of course less. Any child in the hands of hospital or other institutional authorities, developing a slight sore throat is almost certain to be subjected to inoculation on the pretext of " a precautionary measure."
The mortality from diphtheria in England and Wales in the thirty years previous to 1895 was 4,676 per million living. In the thirty years after the introduction of anti-toxin it had risen to 5,197 per million.
This fact alone should have sufficed to finally discredit serum treatment in the eyes of the medical profession.
If further evidence were needed to convince any unbiased student of this question it is to be found in the startling fact that whereas from 1890 to 1894 there were 10,777 cases admitted to the London Hospitals, from 1895 to 1899 they had increased to 29,058, whilst from 1900 to 1904 there were 31,774.
The reckless (or deliberate ?) diagnosis had reached such a point in 1922 that the Report of the Registrar-General stated that during that year there were 2,027 cases wrongly diagnosed in the London area alone ; and Dr. Hutchinson who investigated an outbreak of diphtheria in a large institution, is reported by the Ministry of Health as saying :�" he found that of 107 notified cases, the diagnosis in no less than 100 of them had been based on bacteriological grounds alone."
The diagnoses were, in fact, made in the teeth of the instructions issued by the Department in their Report (No. 10, p. 5) :�" The notification of cases of diphtheria under the Infectious Diseases Notification Acts should be limited to persons actually suffering from diphtheria, i.e., those exhibiting clinical signs of the disease, with or without bacteriological evidence of the presence of diphtheria bacilli."
By what subtle influences do such statements as the following get into the text-books : " The presence of Klebs-Loffler bacilli in association with a sore throat may be regarded as conclusive proof that the lesion is diphtheritic even though there may be no typical diphtheritic exudate." 1
A London panel doctor was severely censured by the Medical Service Sub-Committee of the Insurance Committee for failing to take a " swab" of a throat. Yet the Public Health Committee of the County of Warwick 2 state :�" the taking of swabs as a routine measure is unnecessary and misleading. The presence or absence of the diphtheria bacillus on the swab is no proof of the existence or otherwise of clinical diphtheria in the patient."
1 Index of Differential Diagnosis of Main Symptoms, Herbert French.
2 Report, Jan., 1926.
The British Medical Journal refers to " the utterly illogical and wasteful practice of wholesale swabbing " (March 19, 1932).
The distinguished throat specialist, Dr. Lennox Browne, wrote to protest against the character of some of the literature appearing in the British Medical Journal about antitoxin. He described to the Clinical Society of London five cases in which he had tried the anti-toxin. Two of these died of suppression of the kidney secretion in 35 and 54 hours respectively, whilst in the other three cases there was a tendency to such suppression.
Dr. Hansemann, a colleague of Virchow's, declared " No one has seen this anti-toxin ; it has not been produced in a test-tube ; it is not a fact only a hypothesis, yet it is spoken of as if it had been isolated, and were a definite chemical substance."
A very premature report purporting to give the results of anti-toxin treatment in the London isolation hospitals was published in The Lancet and British Medical Journal barely three weeks after it had been in use.
This report stated that in one hospital in forty-three cases of diphtheria the mortality was 4.6 per cent., " the lowest mortality on record." A surgeon at the hospital in question found that the 4.6 per cent, was based upon calculations that included cases admitted one or two days before, and that the percentage rose to 8 per cent, within two days, whilst three weeks later it was 19 per cent., and at the end of four months 27 per cent., practically the same rate as had obtained under older methods during the two previous years. This premature and utterly misleading report secured wide publicity. What was its genesis ?
It emanated from a soi-disant " School of Medicine " which makes a huge profit from the sales, etc.
Another report, which found its way into many journals, referred to a quarterly meeting of the Board of Governors of the London Hospital and stated that the use of anti-toxin was represented at the meeting as having reduced the mortality from diphtheria in the London Hospital by 50 per cent. An enquirer wrote to the hospital authorities for confirmation of this remarkable statement, and, in reply, the governor informed him :�" No medical report whatever on this matter has been published, and it is felt to be premature to make any public statement on the matter. The statistics of the cases treated here are very far from complete."
Why does the medical profession allow itself to be exploited and out-manoeuvred ?
Chapter 11: THE SCHICK "TEST" FAILURE
"There will be more vaccination, more immunizing, more consulting and use of the physician. His services will be increased many fold."�Dr. Pfeiffenberger.
A more serious aspect of this treatment is the grave risk involved, greater, in fact, than the risks accompanying the disease it is supposed to prevent.
" If diphtheria is brought under proper treatment and surroundings on the first day of the disease," writes Dr. Berdoe, " it almost invariably recovers. Diphtheria is scarcely ever fatal if the patient is put to bed and properly cared for on the first day of the illness."
An American physician communicated 1 the results of injections of pure serum from a mule into human subjects :�
1 Journal of the Arner. Med. Assoc, May 4, 1895.
(1) There appeared in the patients a fine rash-eruption, causing intense burning
and itching,
(2) Severe neuralgic pains occurred.
(3) A pronounced rise of temperature.
(4) After the disappearance of the eruption the temperature declined to normal.
(5) There appeared swelling of the extremities, lips and eyelids.
Numerous deaths have occurred as a result of the treatment with serum.
Variot is quoted as having drawn attention to the quickening of the heart's action, weakening of the heart, and disturbance of the pulse rhythm following the injection of serum. Dr. Lennox Browne drew the attention of the Clinical Society to what could not but be considered as an increase, under the use of serum, of the most grave complications of diphtheria, viz., anuria, nephritis, and cardiac failure.
At Dallas (Texas), in 1919, sixty children were made seriously ill, and ten died as a result of injections of toxin-anti-toxin. The symptoms were pyrexia, vomiting and pain, inflammation of the skin and the formation of large vesicles filled with a clear fluid. The mixture injected had passed the " tests " of the New York State Board of Health.
In 1924, at Concord and Bridgewater (Mass.) forty-five children were made seriously ill by similar treatment and many of these suffered terrible pain. In the same year, Dr. Lee Pattison reported in the British Medical Journal that, as a result of inoculation at the Crippled Children's Hospital at Sheffield, a boy &f eight had an inflamed and painful arm for three days, and a girl had a painful arm and fainted in bed.
In September, 1923, seven children died at Baden (near Vienna) from inoculation with anti-diphtheritic serum.
Yet, in the teeth of these facts Medical Officers of Health have the effrontery to assure the public that inoculation is free from danger!
Thus, the Public Health. Department of Salford issues a leaflet in which inoculation is stated to be " safe and efficient," " safe and quite harmless." Further, it states that this treatment " fails to protect only about two in every hundred done," which works out at twenty thousand per million. As there are, according to Sir G. Newman's Report, six and a half million children under ten years of age, this would mean 130,000 cases of diphtheria yearly in children alone!
This absurd figure is more than double the number of cases for the whole population (adults and children) in 1929, and 50,000 more than the total for 1930. A doubtful boon�this inoculation!
The Medical Officer of Health who accepts responsibility for this document is Dr. H, Osborne, and he has the temerity to add "no indisposition of any kind results." 1
He would do well to read the report of his colleague Dr. Davies,2 of Bristol.
" During the period covered by the increased use of toxin-anti-toxin and therapeutic serums," states the Journal of the Medical Society of New Jersey, " the incidence of serum disease has also increased."
Dr. Netter of the Faculte de Medecine de Paris reports on the injection of anti-diphtheritic serum, as follows : " The fear of these accidents which is very widespread, both in the medical profession and among the people, has too often formed an obstacle to the use of serum in cases in which this was absolutely necessary. Still more has it obstructed the use of anti-toxin for prophylaxis. It is, of course, known that disagreeable sequela, and even death, have been observed as the result of a single injection. With injections spaced out at intervals of more than ten days these accidents are more immediate and more alarming. This is the phenomenon of ana-phylaxis." 3
" It might be interesting," remarks " Medico," 4 " to note that the majority of cases of diphtheria which I have seen during the past year has been in children who have received toxin-anti-toxin at the hands of our public agencies."
1 Vaccination Inquirer, Feb., 1932.
2 The Lancet, Nov. 21, 1931.
3 Medical Officer (Oct. 14, 191G).
4 New York Medical World, Mar. 28, 1931.
The same writer truthfully observes;� "The literature which has been issued in connexion with the campaign has been distinctly misleading, and has given the public the impression that children who have received the full series of injections cannot acquire diphtheria after a period of six months following."
Whenever an enterprising manufacturer or tradesman secures a highly profitable line of goods he, naturally enough, seeks to follow up his success by introducing a similar article, and his competitors are not slow to emulate his example. Precisely the same thing is noticeable in the world of medicine.
The well-advertised " discoveries " of the French chemist, Pasteur, were followed by the, at least, equally well-advertised researches of the Berlin professor�Koch.
The general public would do well to dismiss from its mind, once for all, that such " rare and refreshing fruits " of research are for its benefit. The true position has been stated with unconscious candour by one of the most ardent advocates of inoculation, Dr. Malther Pfeiffenberger. At a conference of health officers on Dec. 3rd, 1926, he said :�" Prevention practised to its utmost will create more work for the physician and not diminish it for the full-time health officer will be educating his community constantly. There will be more vaccination, more immunizing, more consulting and use of the physician. His services will be increased many fold.
" I am informed that epidemic and endemic infections cause only 12 per cent, of all deaths and that this percentage is declining very rapidly. Less than 15 per cent, of all children would ever get diphtheria even under epidemic condition while 100 per cent, are prospects for toxin-anti-toxin. The percentage who would ever get smallpox under present time conditions is even less: but 100 per cent, are prospects for vaccination. Scarlet fever will soon come for its 100 per cent also as it may for measles, judging from the reports on that disease."
Hardly less assurance characterizes the remarks of another representative of these vested interests.
After pointing out that vaccination for smallpox is the only prophylaxis which has been recognized by the State, the President of the Association of Public Vaccinators of England and Wales, Mr. J. Foster Palmer, said :�" In fact the only practical flaw in the system seems to be that our scope is limited. Our work is confined to the prevention by prophylactic inoculation of a single disease, whereas if it were made more general we should be ready for all consequences as they arose." He suggested the addition of typhoid, tetanus, scarlet fever " or any other inoculable disease, as the necessity of the case arose." 1
1 Medical Officer, May,
If so transparent a piece of humbug as the immunization against diphtheria could be " put over" surely nothing was too farfetched if only it meant more work for the manufacturing chemist, and more fees for the doctors. The drawback to anti-toxin was that one had to wait until children showed signs of some illness that one could reasonably describe as diphtheria. Now, if only every healthy child could be inoculated with a view to finding out whether the poor mite was likely to have it in the future, two points would have been scored�every infant born would be a customer (or " prospect ") for the preliminary treatment or " test," and all those who reacted would undergo a further inoculation with anti-diphtheritic serum, thus not only establishing a new branch of the industry, but, incidentally putting an additional and substantial sum into the hands of the anti-toxin manufacturers.
Yet, there is no scientific proof that the Schick " test " is of the slightest value. It is all pure assumption. But this does not stand in the way of the interested parties moving heaven and earth, and succeeding, at least as far as the latter is concerned, in getting their proposition taken seriously by Public Health authorities in various countries including our own. The Ministry of Health recommended the Shick test in 1921. It was used on helpless workhouse children in Lambeth and elsewhere, and strenuous efforts are continuously being made to extend this and anti-diphtheritic serum treatment.
In this, as in all varieties of inoculation, the dangers are by no means slight. In a Report of the Ministry of Health 1 it was admitted that the dose originally suggested by Schick had been further diluted, one reason for this being found in the fact that reactions obtained in susceptible individuals with this dilution of toxin tend to be less severe and persistent than when the more concentrated solution, as originally employed by Schick, is used.
1 Nov., 1921.
Moreover, the Report admits that in certain instances " an unnecessarily severe reaction has been produced."
There must be powerful influences at the back of these preparations to keep them going in the teeth of such adverse results ! Dr. Wilfrid H. Kellogg of the California State Board of Health has presented unassailable proof that the Schick test for diphtheria should be abandoned absolutely, not only in private but also in public health practice. He declares that the percentage of error in reading reactions in those who are protein-sensitive is, in the hands of the most experienced, frequently as high as 50 per cent. In commenting upon Dr. Kellogg's views, the Medical Journal and Record 1 remarked, " There is a growing feeling among public health workers that the Schick test should be abandoned in the immunization of large groups of children."
1 U.S.A.
There appears to be a tendency to extend the use of anti-diphtheritic anti-toxin without the preliminary Schick " test." Unlike vaccination against small-pox, inoculation against diphtheria is not legally compulsory, but the wide powers arrogated to themselves by the officials of the Ministry of Health, the issuing of literature at the public expense with the express object of alarming ignorant or nervous parents, the exploitation of " children's clinics" and influence brought to bear upon school teachers are almost as effective a means as an Act of Parliament.
A favourite method of pushing inoculation is that of a circular letter from the Medical Officer of Health to parents whose children have recently begun to attend school, offering free protective treatment against diphtheria (the treatment being only " free " in the sense that it is paid for out of the rates).
In a recent instance 1 the letter was followed up by a second one written in the approved style of the " patent medicine" vendor. Here are a few extracts :
" WE HAVE NOT YET RECEIVED YOUR CONSENT. MAY. WE ASK WHY ? "
" Do you realise that next year it is highly probable there will be a severe outbreak of diphtheria in Beckenham ?
" ARE YOU GOING TO LET YOUR CHILD RUN THE RISK OF CATCHING THIS DISEASE ?
" PLEASE DO NOT DELAY�SIGN THE CARD NOW."
" The treatment consists of the injection into the forearm of a tiny amount of specially-prepared serum. Three doses are needed at fortnightly intervals, and no pain or illness is caused."
1 Signed " T. Philips Cole, Medical Officer of Health."
The best reply to such a lucubration is a letter asking the M.O.H. if he is prepared to give a written guarantee that no pain or illness will follow inoculation, and to undertake to compensate the parents for any loss arising therefrom.
Chapter 12: TYPHOID AND THE " PARATYPHOIDS "
In 1880, Eberth claimed to have discovered the specific bacillus of enteric fever. It is described as a short, thickish bacillus having rounded ends. In size, shape, mode of staining and growth on gelatine it has a similarity with the B.coli commune, so much so, that Rous and Rodet believe the latter may under suitable circumstances be converted into the former. Though the majority of pathologists profess to believe in the Eberth bacillus as the specific cause of typhoid, the mode and source of infection are in many cases difficult to prove.
As far back as April 8, 1899, Dr. Granville Bantock claimed to have proved that " the essential element in the case of typhoid fever is not the bacillus typhosus : that this bacillus can live but a few hours in ordinary sewage : that not a single specimen of this bacillus has ever been discovered in sewer air, and hence that typhoid fever cannot be attributed to it because of its contained germs ......that the so-called pathogenic organisms are constantly found under conditions consistent with perfect health, and that, in more than one notable instance, they not only appear to, but, actually do, exert a beneficial influence."
In a lecture delivered under the auspices of the Chadwick Trust,1 Sir Malcolm Morris expressed the opinion that " in the main the armies on the Western Front in the late war were preserved from the ravages of dysentery, diarrhoea, typhoid, typhus and cholera by good sanitation carried out on Chadwick's principle of providing a wholesome environment."
Not only did the Army water-cart and the tea-kettle play their part, but an additional expedient in the shape of chlorinated water had, according to Capt. J. Stanley Arthur, " solved the problem of a pure water supply on a large scale for the troops, and accounted for the fact that throughout the war there was no epidemic of typhoid or other water-borne disease, which caused such havoc in the South African campaign." 2
1 At Manchester, Dec. 7, 1921.
2 Lecture at Inst. of Mechanical Engineers.
As the Home Front in Flanders and Picardy was but a few hours journey from the Metropolis, the A.S.C. and A.M.S.C. were enabled to eliminate the risks which attended other campaigns. This fact was eagerly seized upon by the advocates of inoculation, though any student of military hygiene could have predicted the results.
Military hygiene in the French Army had not reached the high standard of our own, but this should not have mattered if the antityphoid inoculation is protective, as inoculation was made compulsory five months before the war. Yet, in the first years of the war (Aug., 1914, to Oct., 1916) 1 there were 113,465 cases of typhoid fever and 12,380 deaths.
Considerable light is thrown on the futility of inoculation when we turn from the Home Front to Gallipoli, Egypt, Malta, etc., where the water supplies were not so easily controlled and the parched troops had to avail themselves of whatever came to hand. The number of cases of intestinal disease has been put at 96,000, and of these nearly 28,000 are credited to Gallipoli. Fleet-Surgeon Bassett Smith declared that all cases from the Near East labelled as dysentery should be regarded as probably examples of typhoid fever."2
1 I have seen no later figures.�C.W.F.
2 Royal Soc. of Med., Nov. 23, 1915.
Disease at Gallipoli: Inoculated and uninoculated l
Dysentery .. 17,873
Cholera Nil
Trench Fever Nil
Pyrexia 1,490
Typhoid 425
Paratyphoid.. 8,103
It is difficult for any unbiased person reading this letter to come to any other conclusion than that the classification of these cases clinically would have shown an enormous increase in the number of typhoid cases and a corresponding reduction of the figures for Dysentery and Pyrexia.
Confusion is caused by an inveterate habit of those interested in pushing serum therapy of sub-dividing the various diseases and substituting a bacteriological for a clinical diagnosis, the result being that the mortality rate is augmented or reduced to the advantage of serum treatment as compared with other methods. We thus arrive at the reductio ad absurdum of Dr. Kanthack 2 that the specific germ is found in every case of the disease, and if one fail to find it, no matter how unmistakably the presence of the disease is indicated by clinical symptoms, one must refuse to admit that the disease exists !
1. Letter
from Way Office to Mr. H. Chancellor, Oct. 30, 1916.
2 See ref. to Kanthack, Chapter IV,
All sorts of fantastic classifications have been introduced to cover the failures of the serum treatments. When it was obvious that anti-typhoid anti-toxin did not confer immunity1 and that those treated with it had the temerity to develop typhoid, something had to be done. As theoretically the immunized person could not have typhoid, it was decided to invent a new name, hitherto unknown to the clinicians�paratyphoid. Nor was this altogether a disadvantage, for, of course, a new serum had to be found to apply to paratyphoid. Then, when persons inoculated with both kinds of serum developed what looked like typhoid something further had to be done. But your bacteriologists are never at a loss for expedients, and they promptly discovered that this was another kind of paratyphoid, viz.�paratyphoid B. So, yet another preventive serum was put up, and when, in spite of inoculation against paratyphoid A. and B., an outbreak of typhoid occurs on a large scale in Mesopotamia, and the natural inference would be that inoculation was useless, the interested parties will admit nothing of the kind, but produce from their capacious sleeve yet another card� paratyphoid C. (See Appendix 8.)
1 Writing of her War experiences in Serbia, Mrs. St. Clair Stobart says :�" Every member of this unit, before leaving England only two months before, had been inoculated against typhoid," yet " one after the other seventeen women members of the unit were laid low, and three including Mrs. Dearmer died."--The Flaming Sword
" Enteric fever (typhoid and paratyphoid)," writes Dr. Garrow,1 " far from being the protean disease it is usually represented to be is remarkably constant in its clinical manifestations and true to type. This applies to the inoculated and uninoculated. Every degree of intensity may exist from extreme mildness to overwhelming severity."
Dr. E. W. Goodall, the well-known fever hospital doctor, writing to the medical papers (April 15,1916) in regard to the three arbitrary varieties of typhoid fever�typhoid, paratyphoid, and paratyphoid B.�declared " it is quite impossible to diagnose clinically the three infections one from the other."
Prof. A. Castellani stated that in the tropics true typhoid and paratyphoid could not be distinguished clinically, and therefore must be separated bacteriologically. Nearly all the speakers at the conference 2 claimed to follow Prof. Dreyer's method of agglutination in making their tests, but Sir William Leishmann, a supporter of anti-typhoid inoculation, states that Dreyer's method contains some fallacies and needs " controls " before it can be accepted in its entirety.
1 The Lancet, Oct. 30, 1920 : The Myth of Atypical Enteric Fever.
2. Roy. Soc. of Med., Nov. 27, 1915,
Differentiation between typhoid fever and paratyphoid appears to be a purely arbitrary device�one of those numerous " bolt holes " which the advocates of serum-therapy find so convenient in an emergency. The same remark applies to the classification of deaths from dysentery instead of typhoid. In All-butt's System of Medicine typhoid fever is described as being synonymous with dysentery.
The eagerness of the supporters of serum treatment to avoid recognition of any fact that might bring inoculation into disrepute is shown by the admission of two medical officers (Upjohn and Martin) that " when a case came before us from an inoculated man we viewed it with suspicion." They tested bacteriologically 325 cases clinically diagnosed and treated as typhoid, but conveniently eliminated 300 ! 1
1 The British Med. Jour. (Sept. 2, 1916) contains a report by Lieut.-Col. C. J. Martin and Maj. W. G. D. Upjohn (pattiologists to No. 3 General Hospital A.I.F.).
The cruel persecution of those persons who refuse to take the risk of having these dangerous poisons injected into their blood (or that of their dependents) is a noticeable feature of vaccine and serum therapy ever since vaccination for smallpox was made compulsory by law. The extent to which illegal compulsion was enforced in the Army during the War was a positive scandal.
Speaking in the House of Commons on Aug. 22, 1916, Mr. H. G. Chancellor said :� " I am having the most pathetic letters day after day from the wives of men serving in different parts of the country, in France, and elsewhere, complaining that their husbands, who have never been guilty of any crime, and who have never had any legal punishnent inflicted on them, have been denied leave for one year, for two years and in some cases ever since the war broke out, and that the only explanation is that they have refused to undergo this process of inoculation, which they have a perfect legal right to refuse, and which they are justified in refusing, on the assurance of Minister after Minister, including the late Lord Kitchener." Mr. Chancellor then quoted the case of Privates H. Hardy and G. Latham of the 2/6th Royal Sussex Regiment (then in India) commanded by Col. Johnson. These two men enlisted at an early period of the war. They refused inoculation and were subjected to the most cruel persecution on the part of the colonel under whom they served.
They had illegally been awarded punishment in the shape of imprisonment for twenty-eight days C.B. on the voyage, for refusing inoculation, and for nothing else, because no other crime was committed by them. They were awarded a further fourteen days for complaining to the British Consul at Mysore.
Like other forms of inoculation, antityphoid inoculation is fraught with very grave danger. During the war the rank and file viewed it with well-founded suspicion. The suggestion that they submitted to it willingly is in direct conflict with the facts. Many well-authenticated cases of injury could be quoted if space permitted. Two typical cases were: Sgt, H. Nichols, aged 51, and Pte. R. Parkinson, of Lytham. Both were taken ill almost immediately after inoculation, and both died.
" The danger of inoculations of serum for typhoid is much greater than the public suppose, for in our late War thousands of healthy, vigorous soldiers in the prime of life were forced by the military authorities to submit to inoculations with typhoid serum. Many of them became ill after the injections and in one small company thirteen men had to be carried to their tents on stretchers, suffering from shock such as a sandbag might produce, and some of these men have told me that they never recovered from the effects of these inoculations."�John B. Fraser, M.D., CM. (Toronto).
Chapter 13: TETANUS OR "LOCK-JAW"
In general details the story of tetanus does not differ widely from that of other disorders which we are told have been " wiped out by serum treatment." It has not even been wiped out. Nicolaier claimed to have discovered the tetanus bacillus in 1885 in pus produced by inoculating mice and rabbits with soil, but it was not until 1889 that the Japanese bacteriologist, Kitasato, discovered a method of cultivating this organism, the essential feature being a complete absence of oxygen. This particular organism has been found in the tissues surrounding the abscesses in tetanus cases, in garden earth, in dust from the streets, between the floor-boards of living rooms, and in the pus from certain suppurating wounds. Kitasato also found other bacilli bearing a close resemblance to the tetanus bacillus, which may form spores and are equally resistant to heat,1 but do not give rise to a similar poison. Most of these microorganisms appear to have " doubles."
1 G. Sims Woodhead.
Sir David Bruce, whilst favouring the idea that anti-tetanic serum is useful as a prophylactic, states his views very fairly. He is dealing with the first 200 cases of tetanus in the British Expeditionary Forces during the early weeks of the War :�
" Most of the cases occurred during September, October, and November, 1914. This may have been due to the fact that the wounded were more exposed to contamination of their wounds at that time which included the retreat from Mons; that there was less opportunity of receiving surgical treatment as rapidly and effectually as later on ; that during this time the preventive use of anti-tetanus serum had not been developed as it has during the last six months, when it is reported that, wherever possible, every wounded man has received a prophylactic dose; and generally that experience has taught medical officers how better to cope with the conditions obtaining in time of war, to unlearn the lessons of modern aseptic surgery, and to resort to older methods of free incisions, thorough drainage, and constant removal of septic products by baths or irrigation." 1
In a subsequent article 2 Sir David expresses his views with equal cogency :�
" The mortality has been reduced to 19 per cent, for the last 100 cases, but whether this has been due to the specific treatment, or to which of the several factors which come in it is impossible at present to say. Whatever is the cause�the prophylactic dose of serum, better surgical treatment, quicker diagnosis, more thorough therapeutic treatment, etc.�the result is gratifying. It is difficult to apportion the proper awards. For example, if surgical treatment could be made successful, if wounds could be cleaned up and rendered sterile at the beginning, then there would be no more cases of tetanus.'
1 The Lancet, October 23, 1913.
2 December, 1915.
And, he might have added, no need for anti-tetanus serum. (See Appendix 9.)
That inoculation with anti-tetanic serum does not protect against tetanus was demonstrated during the War. There was no inoculation in our Army from August to December, 1914, and there were 183 cases of tetanus during that period. Yet, in the corresponding period in 1915, when practically every wounded Man was given a protective dose there were 310 cases, and a still greater number in 1916. It is no answer to these figures to say there was a greater number of men, for the raison d'etre of the serum is that it prevents tetanus !
As this increase had to be explained, Sir David Bruce attributes it to an improvement in the diagnosis of mild cases. In August, 1910, the War Office issued a memorandum directing Army medical authorities no longer to regard the " classical symptoms of tetanus as described in the majority of the text-books" as the only evidence of the disease. They were told to carefully examine the muscles of the wound, and to take note of any rigidity, twitchings or response to pressure or tappings. Any such symptoms are described as " local tetanus," and Sir David Bruce states that the result of this order was to considerably increase the proportion of cases of tetanus among the wounded. During 1916-17 nearly one-fourth of the recorded cases of tetanus were of this type, that is to say, they would not have been diagnosed as tetanus prior to the introduction of anti-tetanus serum. As this newly-invented form of " tetanus " " has no mortality " its inclusion with the real tetanus or " lock-jaw" has the effect of watering down the death-rate and enabling Sir David Bruce to say that the death-rate from tetanus has been reduced from 57 per cent, to 19 per cent.
It will be noticed how closely this procedure resembles the claim that anti-diphtheritic serum has lowered the death-rate in diphtheria, the percentage having been brought down by including mild throat disorders under the head of " diphtheria."
The more cases of " diphtheria" and " tetanus " that are not really diphtheria and tetanus added to the total, the less will he the percentage of fatal cases !
According to a writer in the Encyclopedia Britannica, " among the unprotected and unrecorded the death-rate was 53.5, whilst among the protected it was 23. The unrecorded here undoubtedly include cases which had received a dose :
Percentages.
| 1914 | 1915 | 1916 | 1917 | 1918 | |
| General | 98.9 | 98.6 | 87.0 | 76.6 | 85.5 |
| Local | 1.1 | 1.4 | 13.0 | 23.4 | 16.5 |
It is claimed that the relative increase of local tetanus as compared with general tetanus indicates the ameliorative effects of anti-toxin. It is equally probable that the classification of cases as " tetanus " which, formerly, would not have been so diagnosed has had the effect of giving a false impression.
" Local tetanus," " suspicious sore throat," " para-typhoid A, B, and C," " variola minor," are all ingenious expedients " to give an air of verisimilitude to an otherwise bald and unconvincing " 1 story.
1 W. S. Gilbeit.
Basing his convictions on 150 cases of tetanus which had occurred at the London Hospital during the last 15 or 16 years, Prof. Bulloch, F.R.S., states :�" The general impression is that there is no diminution in the mortality in the post-anti-toxin days as compared with that in the pre-anti-toxin days."
And Sir David Bruce, himself, in the course of a discussion on tetanus at the Society of Tropical Medicine, remarked :�" Nothing can be easier diagnosed than tetanus, and yet we know no more about it than people did two thousand years ago. And there is still this incompleteness of detail, so that 20 years after the introduction of anti-toxin treatment, the point is still under discussion as to whether anti-toxin benefits the patient or not."
Dr. Leslie Cole, M.A., F.R.C.P., declares that " the therapeutic value of anti-toxin is still a disputed question. Toxin reaches the central nervous system via the motor nerve endings and the axis cylinders of the motor nerves. Once it has reached the central nervous system it becomes fixed to the nerve cells, and with one exception, the experimental evidence shows that anti-toxin�even in very large doses�has a negligible neutralizing effect upon it."1
In the Times of Aug. 2, 1916, it was stated that anti-toxin treatment " has created wound carriers" of tetanus who on this account may be a source of danger to others as well as to themselves. The danger which a carrier himself incurs is due to the fact that his infection does not appear, as a rule, to excite his own tissues to develop any considerable degree of immunity or antidote. The moral is that wounds must be cleansed as quickly as possible.2
Dr. C. H. Browning, commenting on Sir David's paper, said that the figures given by him would seem to show the " utter uselessness of anti-tetanic serum as a therapeutic agent." Yet the injection of anti-tetanus serum has become an established ritual, and so powerful are the influences behind it that a London hospital,3 the subscribers to which are opposed to the use of serums, has recently been induced to adopt anti-tetanic serum treatment.
1 King died in St. Nicholas Hospital, Plumstead, despite the fact that 412,000
units of anti-tetanus serum were administered. �Daily Telegraph, Aug
12th 1931
2Brit. Med. Journal, April 23, 1923.
3
Battersea General Hospital.
Chapter 14: CHOLERA AND THE PLAGUE
The story of the discovery of the so-called cholera bacillus 1 by Koch in Egypt (1883) is not less bewildering to the searcher after truth than those already dealt with. The " comma " bacillus separated by Koch from the dejecta and intestines of cholera patients is a short, curved organism, often ranging in a spiral form. The curvature varies considerably from an almost complete semicircle to a straight line. The power of spontaneous movement is a marked feature. " Opinions have constantly changed since Koch's discovery of the comma bacillus, and, from the very outset, his conclusions have been strongly opposed.''2
1 It is actually a vibrio.
2 A. Kanthack, M.D., and J. W. Stephens, M.B., loc. cit.
It is taken for granted that the comma bacillus is the cause of cholera, but Koch himself found that amongst those who had been exposed to the possibility of infection, and who remained apparently healthy there were individuals whose fasces, though normal, contained " cholera " bacilli.1
" Koch's discovery of the spirillum or ' comma ' bacillus of cholera had to contend with an obstinate scepticism, because cholera could not be produced with it at will in laboratory animals, unlike anthrax or fowl cholera. Even when several savants swallowed cultures of it the results of these experiments ' in anima nobili' were very inconstant." 2
1 Koch�The Cholera in Germany during the Winter of 1892-93
2 Dr. Etienne Burnet.
It is clear that the bacillus may exist and may be excreted in large numbers by healthy persons, and that their presence without accompanying clinical symptoms constitutes no evidence of the existence of cholera.
It would again seem, then, that Koch's postulate " C" must be scored out, and that, as usual, we are asked to accept the dictum of the bacteriologist that there are two types of disease�the clinical and the bacteriological! In the latter, the mere presence of the suspect bacillus in an otherwise healthy person is the basis of the diagnosis !
In 1890, Dr. D. D. Cunningham published the results of his investigations.1 He had seen undoubted cases of cholera without the presence of the comma bacilli. From sixteen cases he obtained as many as ten distinct species of germs, differing morphologically, biologically and chemically.
In fact so far from the bacillus being the cause of the disease, he suggests that the special morbid condition existing in cholera enteritis is the cause of the presence of the bacillus. Cunningham failed to find Koch's bacillus. His statements as to the multiplicity of vibrios associated with cholera have been confirmed by Dr. Klein. Another observer, Sanarelli, holds the opinion that there are different races of vibrios all capable of causing true cholera. He obtained no less than thirty-two water vibrios of extreme variability. " Nous pouvons conclure," he writes, " qu'il a des races diverses de vibrions choleriques inegalement virulents." 2
1 Scientific Mem.
by the Medical Officers of the Army of India
2. Variability of some degree is common to all germs, as it is in higher animals
and plants ; but the cholera microbe is one of those in which, owing to their
organization and mode of life, the variability is particularly marked ; so much
so that not infrequently, after an examination with all available tests, it is
impossible to say whether the germ dealt with is or is not a representative of
the cholera species.'�-Haffkine, Protective Inoculation against Cholera.
In cholera the clinical lesions are uniform and characteristic, as they may be
caused by several closely-allied forms of vibrio. Accordingly we find that it is
not possible, in the laboratory, at any rate, to obtain a universal anti-choleraic
serum.� A. Kanthack.
Observations made by Pettenkofer, Emmerich, Metchnikoff and Hasterlik are collectively reported as follows :�" eighteen persons swallowed pure cultures of vibrios. In some cases severe symptoms followed, in others none, in others again slight diarrhoea. Not one succumbed to the infection."
Assuming then, upon the slenderest evidence, that a specific germ is the cause of cholera, the Pasteur school is ready with a " vaccine " and Haffkine claims success with a living virus attenuated and strengthened a la mode Pasteur. He declares that the mortality among the inoculated was 17.24 less, and the incidence of cholera 19.27 less than among the non-inoculated. But the question arises, whether, if there are such varieties of organisms involved, artificial immunity procured by one variety implies protection against the other. Sabolotny is of opinion that it does not. Experiments on animals appear, as usual, to have confused the issue. The intra-peritoneal inoculation of guinea-pigs which is generally followed by death, and was at one time thought by Koch and Pfeiffer to be characteristic of the true vibrios has proved unreliable. The idea that such inoculations were followed by specific results and therefore of great value for the purpose of diagnosis was also found to be chimerical, for Klein demonstrated conclusively that similar symptoms follow inter-peritoneal injections of a number of other bacterial forms including the Finkler-Prior vibrio, the bacterium coli, the bacillus pro-digiosus, proteus and others. His views have been confirmed by Sobernheim, Grttber and others.
" Of all the means of local dissemination water is the most important, because it affects the greater numbers, particularly in places with a public water supply. All severe outbreaks of an explosive character are due to this cause " (Encyclopedia Brit.).
Dr. Kenneth McLeod remarks :�" The theory which offers a key to the bewildering mass of cholera literature ... is that which finds the causation of cholera in a disregard of the laws of health, and in the presence of an organic (microbic) poison." The earlier portion of the above sentence is admirable, but the last nine words seem to darken counsel in the light of the facts quoted.
" The natural home of cholera is a land of foul water," writes the late Mr. Ernest Hart, and he further remarks :�" The habits of the people and the condition of the water supply in many Indian villages are such that, if one did not bear in mind that a necessary factor in the etiology of cholera is the susceptibility of the Individual, one might expect the whole mass of the inhabitants to perish rapidly of that disease.''
It seems strange that it does not occur to these distinguished authorities that a gradual modification in the habits of the people, and an improvement in the water supply might be a surer and safer means of abolishing epidemic than reliance upon such dubious and dangerous methods as inoculation.
For, although Haffkine claimed that he found the mortality seven times less in vaccinated than in non-vaccinated persons, the severity of the symptoms is quite as great among the former, which, as Dr. Burnet, of the Pasteur Institute, admits, ." is rather disconcerting."
Like cholera, the disorder known as the plague is directly associated with insanitary conditions, and it is to their removal and not to " anti-plague serums " that we should look for its abolition.
Dr. J. F. Payne remarks :�" All the localities in which plague flourishes are conspicuously filthy. The villages in Mesopotamia were in an incredible state of filth (Colvill). The sufferers from Indian plague were filthy beyond conception (Francis), the habits of the poorer classes of Chinese in Hong-Kong and Canton are notoriously of the same kind. A soil contaminated with faecal discharges and decaying animal matter of all kinds appears to be an essential condition for the vitality of the virus. Among other causes of contamination must be placed cadaveric infection from bad customs of burial." And he asserts:�" A very moderate improvement in sanitary matters at once limits or eradicates the disease."
Kitasato claimed to have discovered the bacillus pestis�the plague germ-�in 1890 at Hong-Kong. According to Dr. Emery it might be mistaken for a diplococcus.
The announcement of the discovery of the specific germ as usual diverted attention from the prevention of plague by sanitary measures to the use of an anti-plague serum�a bouillon " culture " prepared by Haffkine. A system of serum therapeutics was also suggested by Yersin, Calmette, and Borel at the Institut Pasteur. Repeated injection of virulent bacilli were made into a horse, and after six weeks' preparation, its blood serum, when injected into rabbits, was said to be capable of producing immunity against a subsequent virulent injection of plague bacilli.
The French physicians in Egypt denied the contagiousness of plague. Though they attended thousands of patients and performed many post-mortems they did not contract the disorder. Bulard went so far as to wear the clothes of a patient who had died of plague and Clot Bey failed to inoculate himself with matter taken from a pestilent bubo.
Dr. Charles Creighton confirms the views of Dr. Payne :�" The trouble always and everywhere has been from crowded sites, too long inhabited without drainage. The more compact the site, or the greater the congestion of houses upon it the more will the soil be filled with organic impurities."
Of Shahpur he writes :�" The filthiest and most dilapidated villages that I had seen anywhere, and were credibly said to be swarming with rats," and of a typical Belgaum village in the Bombay Presidency, he says :� " While the infection had crept about to all parts of this village it was the unanimous opinion that it always began in a certain quarter, the high ground on the northern side, next to the high road, which was the particular quarter of the Mahommedan butchers and cattle-dealers. . . . There was no regular slaughter house, but each householder used the space before or behind for killing in. . . . The whole soil of this elevated corner of the village was saturated with the blood and offal of many years, and swarmed with rats as shambles always do." 1
1 See a Paper read before the Indian Section of the Society of Arts
In the epidemic of plague in India in 1896 the total number of deaths for the whole year was 30,000. In the following year anti-plague inoculation was introduced. Yet, in the year 1904 the deaths were 30,000 per week, and from Sept., 1906, to April, 1907, there were 5,326,000 deaths !
An outbreak of plague occurred in Alexandria in 1899, but the common-sense views of the Director-General of the Sanitary Department, Dr. Rogers, led him to deal promptly with it on sanitary lines, which, he declared, were " directly opposed to Mr. Haffkine's views."
Chapter 15: INSULIN : A " NOBEL " PRIZE FAILURE
Although Insulin does not come under the head of a " vaccine treatment," its exploitation and subsequent failure to reduce the mortality from diabetes, is evidence of the futility of modern medical research."
Should a history of medical delusions ever be written, a lengthy chapter will have to be devoted to the story of " Insulin."
According to an article in the Toronto Star Weekly (June 27,1931), Dr. Banting was born on a farm in Ontario, graduated as a doctor in 1916, worked in England, joined the Medical Staff Corps, was awarded a medal for bravery in Cambrai and returned to Canada with a view to practice in 1920.
Prof. J. R. Macleod, of Toronto University, suggested to Banting that he should undertake investigation of the pancreas. This involved vivisectional experiments upon dogs, which Banting declares he could not afford to buy. The article above referred to states : " He also got two students named Noble and Best, who were to help him for three weeks each. He had no money to buy dogs for his experiments, and used to catch stray ones on the streets late at night. In this he was assisted by Best who was a good-looking young blond, and 'could speak nicely to policemen'."
So far from being ashamed of these dog-stealing exploits, Banting referred to them when he addressed his medical confreres in England.
His researches do not appear to have occupied him for a long period, for, in less than two years, the discovery of " insulin " was trumpeted by the press, and a confiding public was assured that, thanks to " research," that hitherto dread disease�diabetes�had at last been conquered.
Before time had been given to test the claims made for this '' epoch-marking '' discovery, the Nobel Prize was awarded to Banting in 1923, he had an interview with King George, was voted by the Canadian Parliament a sum of �1,500 per annum to carry on investigation, and had the satisfaction of seeing a Banting Research Foundation formed to commemorate his achievement. No wonder envious eyes of other research workers are turned towards " the greatest benefactor to humanity in the last fifty years " when " humanity " has so bountifully�if prematurely�-recognized his merits.
Yet, what after all, does this discovery really amount to ?
The production of insulin is little more than an exploitation of work done as long ago as 1889 by Mehring and Minkovski, and also by Schafer.
No remedy has been better advertised, or applied more assiduously by the medical profession, yet Dr William Howard Hay, speaking before the Senate Committee of the District of Columbia, declared that, since the introduction of insulin the death-rate of diabetes has been rising very rapidly, and that there was no evidence to support the claim that the life of the diabetic had been lengthened.
When the figures for the three years, 1920, 1921, and 1922, were available for comparison the result was startling.1 The deaths from diabetes in Toronto had risen from yy to 85 whilst in the whole of the United States the increase in the number of deaths was striking :
The Evening Telegram (of Toronto) of Thurs-
Year. Deaths from Diabetes.
1920 .. 14,062
1921 .. 14,933
1922 .. 17,182
1 Death-rate per million from diabetes (England and Wales): (The figures in
heavy-faced type are for the year when insulin was
ia use.)
1920 1921 1922 1923 1924 1925 1926 1927 1928 1929 100 108 119 114 109 112 115
126 131 142
day, Mar. 10, 1932, contains the following :�
" DIABETIC DEATHS IN CITY HIGHEST EVER
recorded. Last Year's Mortality was 17.9 per 100,000 Population. Dr. Jackson
reports.
" In Toronto last year the number of deaths from diabetes represented a
mortality rate of 17.9 per 100,000 population, the highest rate ever recorded
here for this disease, according to a report of Dr. Gordon P. Jackson, M.O.H.,
to the Board of Health.
" Twelve years ago it was 10.5. In 1922, the year in which the discovery of
insulin was announced to the world, the rate was 14.6 and has since fluctuated
from 12.7, in 1925, to the maximum of last year.
" ' Public health authorities,' he writes, ' are frankly puzzled and alarmed
regarding diabetes for, despite the use of insulin, the death-rate from this
disease is increasing. The increase is world wide, showing a rise of 14.4 per
cent, to a new high which was 61 per cent, in excess of the rate 20 years ago.'
"
The nebulous character of the claims made for insulin is evidenced by what
McLeod himself states, and amounts to nothing more than a pious hope as to the
possibility that the damaged organs will undergo regeneration.1
1 " In diabetes in man, although the islets are more or less diseased they are
never completely destroyed, so that when treatment with insulin is continued for
some time the damaged Wlt may possibly become regenerated."
He admits, also, that the beneficial effect of insulin injections passes off in
a few hours, and they must be repeated twice daily.1 Insulin cannot be
administered by the mouth as the digestive juices destroy it, it therefore has
to be injected either subcutaneously or intravenously. Moreover, the injection
is not a simple operation that can safely be undertaken by the patient himself,
by a nurse, or by a doctor not skilled in estimating the blood sugar.
As a result of their experiences in the treatment of ioo diabetic patients, Dr.
F. Umber and Max Rosenberg state:�" The proper dose for freeing a patient from
sugar must be tried out in every case; it is generally impossible to calculate
the dose at the outset. Only a suitably regulated diet, taking into
consideration the individuality of each patient guarantees complete success."
Insulin was pushed to the forefront by wire-
1 Sir Arthur Keith writes :�" The patient is dependent on these two doses ; if
they are withheld disease resumes its sway, and death ensues more or less
quickly. Clearly insulin is only a palliative for diabetes." He further remarks
:�" If too large a dose of insulin is given to a patient, then the sugar quickly
begins to disappear from the blood, and when it sinks from Une normal amount�15
parts in 10,000�to 4 parts in 10,000 of blood, then the nerve cells of the brain
and spinal cord begin to pass into an excitable state. Unless the sugar supply
is replenished in the blood, as the patient can do by eating a few lumps of
sugar, a state of extreme distress sets in followed by convulsions and
death."�Engines of the Human Body.
pulling and a sensational press campaign and much capital was made out of an
alleged case of recovery of a diabetic patient, Jack Keightley, whose subsequent
death after an interval of a few months was not given special publicity!
The death-rate per million from diabetes in England and Wales for a period of
ten years is, in itself, sufficient to expose the hollowness of the claims made
for insulin. It would be sufficient of a fraud upon sufferers from diabetes if
insulin treatment gave merely negative results. As a matter of fact its use is
fraught with very serious risks�risks which if they were fully explained few
patients would be prepared to take.
Dr. G. Datmann writes, " As insulin is not a harmless remedy, in a case where
the physician has had no personal experience of its use, the application should
not be made according to formula, but a colleague who is acquainted with this
preparation should be consulted." " More serious," writes Dr. R. S. Lawrence, "
are the late reactions ; four to five days after the injection a brownish, hard,
and painful swelling of the skin appears which lasts 24 to 36 hours."
One practitioner reports that, " after about 3.5�o insulin injections made
within a period of three years, the epidermal cellular tissue
and the muscles formed into a hard and cicatrised tissue."
Dr. Sevringhaus reports :�" Serious hypo-glycsemia which was diagnosed and
treated in one case as a luetic disease of the brain, and in another as
incipient autogenous meningitis."
A claim has been made that the condition known as coma diabeticorum can be
controlled by insulin. Dr. Staub, however, gives figures which controvert this.
Thus, of fourteen cases treated by Campbell, seven were fatal; out of nine
treated by Allen five were fatal; out of seven treated by Sansum three were
fatal. As Straub points out, in former times patients were treated for coma by
injections of Sod. bicarb., by diet and symptomatic medicinal treatment. These
expedients are still recommended.
" Insulin," writes M. Labbe, " does not replace dietetic therapy�diabetes must
be first eliminated or reduced to a minimum." 1
Prof. Jajiro Hattori (Tokio) observes " almost invariably in diabetic patients
under insulin treatment a nervous system complex ; fatigue, feeling of
exhaustion, nervous excitement in varying degree."
Recently letters have appeared in the
1 Le traitment du diabite par Insuline Presse Mid. (Nov. 24, I923)-
British Medical Journalx reporting loss of subcutaneous tissue (local
emaciation) following the administration of insulin.
Insulin was introduced to public notice by methods similar to those usually
adopted in connexion with laboratory discoveries.
The dangers and widespread occurrence of the disease�in this case, diabetes�were
stressed. The impression was given that the particular disorder was on the
increase, and that it was beyond the power of the medical profession to deal
successfully with it. It was then (at the earliest possible moment, and before
sufficient time has elapsed to test the matter) suggested that a marked decrease
in the death-rate had been brought about, and a series of articles and
paragraphs in the lay press created a public demand for the treatment.
Now, diabetes was not on the increase at the time insulin was introduced. Nor
was the medical profession bankrupt of ideas on the subject until McLeod and
Banting appeared on the scene.
As Dr. E. Steinitz points out:�"The war period has already furnished us with
proof of the curability of diabetes. The scanty food available during these
years cured
1 June 27-July 4 and Aug. I, 1931.
many diabetic patients, and in addition reduced the frequency of the disease to
a
fraction."
Dr. Elliot P. Joslin states :�" The improvement in methods of treatment during
the past few years is seen best by the statistics relating to diabetes in the
general hospital of Massachusetts, U.S.A. Between 1824 and 1898, 27 diabetic
patients out of 100 admitted to the hospital died there, whilst in 1918, i.e.,
long before the discovery of insulin, the advances made by dietetic methods
alone were so important that out of 100 such patients admitted only four died.
In 1910 according to Dr. Julius Dreschfleld, half of the diabetic patients
succumbed to coma. Under the direction of Dr. E. P. Poulton, the mortality at
Guy's Hospital, at first 16.9 per cent., fell as low as 5.4 per cent. ; the
average mortality in all the cases treated there being reduced from 23 to 7.7
per cent. Whilst formerly only 9 per cent, were freed from sugar even for one
day, now 73.6 per cent, can be freed from it for shorter or longer periods !
Marcel Labbe, M.D. (Paris), writing of insulin in the Medical Journal and
Record, declares that not a single cure for diabetes, through the use of
insulin, has been found.
He states that of his first twenty-four cases thus treated, twelve died within
three years, and not a single authentic cure has been recorded.
It would appear to be a settled function of the Ministry of Health to push the
sale of questionable treatments.1 In spite of the failure of insulin, here, for
instance, is a " puff " written in the approved style that the vendor of ''
patent '' medicines has made his own:�" it is probable that the advantages of
insulin treatment in diabetes are still not universally appreciated by the
medical profession in this country and that many diabetics who require treatment
are not receiving it." How this reflection upon the intelligence and zeal of the
medical profession must have warmed the hearts of the manufacturing chemists ! 2
What, too, is a paragraph like the following doing in the Official Report ?�" It
is highly desirable that Medical Officers of Health of Counties and County
Boroughs should direct the attention of their medical staff to the importance of
securing efficient insulin treatment for all diabetic patients coming under
their clinical purview for whom such treat-
1 In his brochure, La Veriti sur VA (fairs Spahhnger, Spahlinger quotes
appreciative recommendations from officials of the Ministry of Health with
reference to his tuberculosis serum !
2 Report of Chief M.O.H. (1930).
ment is indicated." Not one word of warning as to the dangers, the late
reactions, the painful swellings, the hypog-taemia, the cicatrized tissue and
the increased mortality!
" The spirit of every profession," said the late President Wilson, "is different
to the spirit of the community. I would not trust any particular business to any
particular profession exclusively if it were public business, because every
profession that I know anything about has its special point of view."1
Auditorium Theatre, Chicago, Jan. 31, 1916.
APPENDICES
C.M.H. writing to the British Medical Journal (July 16, 1932) states that between 1920 and 1930 he issued roughly about 10,000,000 doses of calf-lymph which had not been on any other animal than the water-buffalo.
According to a Government Report on Glycerinated Calf Vaccine Lymph1 cow calves
averaging eighteen weeks old are selected, and it will interest consumers of
veal and ham pies to learn that they are re-sold to butchers.
The operating table can be tilted on its side until the calf is fastened to it.
Its restoration to a horizontal position brings the calf " into perfect
subjection." It3 head is encased in a leather muzzle, and its legs are firmly
secured. The abdomen (and in some laboratories inside the flanks) is thoroughly
scrubbed with soap and hot water preparatory to shaving, after which the surface
is again washed. Then a number of incisions �varying from 100 to 120, each about
an inch long and
xBy Sir RicharJ Thome, Thorne & Dr. S. Monckton Copeman.
two inches apart�are made by means of a lancet with a spear-headed blade.
To heal up quickly and satisfactorily a wound must be kept clean, but the object
of these operators is to see the cuts fester and thus produce a maximum amount
of matter. So over each incision a drop of lymph is allowed to fall, and this is
well rubbed in. The process is a somewhat lengthy one, and when the " lymph "
has dried the calf is removed from the table and taken back to its stable.
Whilst the calves are in their stalls their heads and legs are tied up to
prevent them licking or scratching themselves. If it is only intended to collect
the " lymph " from a portion of the vesicles, the animal is allowed to stand,
but otherwise it is again placed on the operating table. The report describes
the process thus:�
" The vaccine material is always collected on the sixth day. The calf is once
more placed on the table ; or, if material is required for immediate use only,
it is usually allowed to stand. The vaccinated area is washed with warm water,
and dried with clean soft cloths. Each vesicle is now clamped separately, and
the crust first removed with a lancet, which is then wiped on a cloth pinned to
the front of the clean cotton blouse which the operator has previously donned.
" The vesicle is then thoroughly scraped with the edge of a somewhat blunt
lancet, and the resulting mixture of lymph, epithelial tissue (skin) and blood
is transferred to a small nickel crucible set in a wide wooden stand on a table
close to the operator.
" To the pultaceous (gruelly) mass contained in the crucible there is added
about an equal quantity of glycerine.
" The mixture of pulp and glycerine is triturated in a mixing machine driven by
a small electric motor.
" The mixture, having thus been rendered thin and homogeneous, is received in a
clean sterilised nickel crucible placed beneath the machine, but with a view to
still further improving its appearance and of removing any extraneous matters,
such as hairs, it is afterwards pressed through a small brass wire sieve,
consisting of extremely fine gauze, into an agate mortar. This is done by means
of a bone spoon, and there is left on the surface of the gauze nothing but a
very small quantity of epithelial tissue together with a few hairs. The mixture
is further triturated in the mortar with an agate pestle, and is then ready for
filling into the tubes in which it is distributed."
3. ENCEPHALITIS LETHARGICA (Sleepy Sickness)
This disorder was first reported from Eastern Europe in the winter of 1916-17,
and in The Lancet of April 20, 1918, two English doctors described cases as
having occurred in England. It has no connection with the " sleeping sickness "
of Africa which is confined to districts where the tsetse fly flourishes. Among
its symptoms is marked weariness, the face is expressionless, and there is a
complete lack of interest in what is going on. In a paper issued by the Ministry
of Health the following after-effects are set out:�(1) Mental symptoms. (2)
Shaking paralysis. (3) Spasms of muscles and other forms of nervous trouble. The
same authority states :� " Few cases of disease are more pathetic than juvenile
examples of this condition, and, alike in children and adults, it must be
regarded as one of the gravest sequelae."
The really alarming increase in this serious disease is shown by the following
figures :� Number of cases in England and Wales.
Year .. .. 1919 1920 1921 1922 1923 19241 No. of cases .. 538 914 1470 454 1025
2468
The association of this disorder is more than ominous, and has at last compelled
the authorities to take action.
Since the peak year of 1924 when there were 5,039 cases of encephalitis
lethargica in the British Isles there has been a decrease, the number of cases
in 1931 being 65.
Serious outbreaks have occurred in Japan, as follow :� 1924 6,551 cases
1926 1,012 �
1927 990 � 1929 2,058 �
In each of these epidemics the fatality rate was considerably over fifty per
cent.4
The following extracts are taken from an article by Dr. John P. Koehler,
Commissioner of Health of Milwaukee, Wisconsin, in the Wisconsin Medical
Journal, November, 1920.
" This we attempted to do in three ways : first, by education; second, by
FRIGHT; and, third, by PRESSURE.
" We dislike very much to mention FRIGHT and PRESSURE, yet they accomplish more
than education, because they work faster than education, which is normally a
slow process,
1 Six months to June 30 only.
2 Second Report by Matheson Committee (Humphry Milford, 1932).
" During the months of March and April we tried education, and vaccinated only
62,000. During May we made use of FRIGHT and PRESSURE, and vaccinated 223,000.
" Our educational programme consisted of warnings in the daily papers, smallpox
posters on the streets, in stores and factories, special smallpox bulletins for
all large places of employment, and special letters to all large employers from
the health department and the association of commerce, calling their attention
to a threatening smallpox epidemic. The radio was also made use of in this work.
" As the conditions grew worse, we felt justified in using stronger measures. We
had some good pictures taken of patients suffering from the confluent type of
smallpox, and had posters, showing these pictures, distributed all over the
city. The moving picture theatres co-operated at this time by issuing warnings
on the screen.
" The newspapers published daily the names and addresses of people dying from
smallpox. A second letter was sent to all factories, stores, and other places of
business, informing them of a rapidly approaching smallpox epidemic, and
advising them to have their employees vaccinated immediately, and thereby
prevent a serious financial loss to the city, which might occur if a real
epidemic developed.
" At this time the department was vaccinating thousands of people daily, BUT
THERE WERE STILL TOO MANY WHO COULD NEITHER BE EDUCATED NOR FRIGHTENED INTO
VACCINATION. Cases and deaths each amounted to a considerable number, and we now
felt justified in using all the power a health officer has, and if that was not
enough, to get more. " We sent out a third letter to all employers requesting
them to have all of their employees vaccinated and at the same time IMFORMING
THEM THAT IF A SMALLPOX CASE DEVELOPED IN THEIR PLACE OF EMPLOYMENT IN THE
FUTURE WE WOULD CONSIDER THEIR PLACE OF BUSINESS A MENACE TO THE HEALTH OF THE
COMMUNITY AND VERY LIKELY PLACE THE ENTIRE ESTABLISHMENT UNDER QUARANTINE UNTIL
IT COULD BE CLEANED UP AND MADE SAFE FOR THE PUBLIC. Putting this responsibility
on the employer drove in thousands of anti-vaccinationists who could BETTER
AFFORD TO GET VACCINATED THAN LOSE THEIR JOBS. All employers co-operated very
bravely with this last request ALTHOUGH IN A FEW INSTANCES IT WAS NECESSARY TO
LAY OFF OLD, RELIABLE AND VALUABLE EMPLOYEES."
Similar methods are becoming too common in Great Britain in connexion with
Vaccination, Anti-Diphtheritic Inoculation and the Schick test. The mendacious
statement that " Smallpox is still prevalent " appears on affiches over the
signature of many Medical Officers of Health, and certain peculiarly vulgar
illustrated posters intended to frighten mothers and induce them to have their
children inoculated with anti-diphtheritic anti-toxin deface the walls in London
and elsewhere. Enforced vaccination under threat of discharge from employment is
still too common, a recent instance being that of Miss Muirhead, employed by
British Celanese, Ltd.
On the point of going to press my attention has been directed to Bechamp or
Pasteur, by E. Douglas Hume
(Chicago, Amer. Liberty League). I had not previously read this book which, in
addition to bearing out my contention as to Pasteur's lack of any medical
training, directly challenges his claim to be the first to have solved the
problem of silkworm disease (pebrene) credit for which is accorded to Pierre
Bechamp.
Pasteur's claims as a pioneer are further challenged with respect to a
communication to the Academy of France on vinous fermentation (Comptes Rendus,
75, p. 281) made in 1872, his views being a plagiarism of those published by
Bechamp in 1864.
Believers in the Pasteur legend would do well to study the evidence in this book
of his ignorance of, and incapacity for the study of medical problems whether
concerning man or other animals.
Bechamp, who appears to have been lacking in the capacity for
self-advertisement, was not only a Doctor of Science and Medicine, but a Master
of Pharmacy and Professor of Biological Chemistry.
It is remarkable that the Medical Profession is so ready to accept at face value
the dicta of men, who like Pasteur and Tyndall have had no special training in
physiology, pathology or therapeutics.
The following cogent criticisms from the pen of W. E. McCulloch, M.D. (Dietetic
Research Laboratory, Kat-sina, N. Nigeria), appeared in the British Medical
Journal, July 9, 1932 :
" The first essential in testing the effects of any food material is to have
dietaries which are strictly comparable and adequate in all respects except the
one
under review. In much of Mellanby's work I do not find these postulates
fulfilled. The origin of the cereal toxamine theory was the fact that puppies
did not do well on diets containing cereals. The dietary in Experiment 46,
reported in No. 140 of the Medical Research Council Special Reports, is typical
of the rest. In it we find that separated milk, lean meat, and linseed oil
supplied a calorie intake of about 200 only, and the addition of white bread
increased the intake to 330 up to 600. It is no wonder that in all Mellanby's
work we find the puppies that grow more rapidly are those which were given more
or less sufficient calories on which to live. The dietary was woefully deficient
in every particular apart from a dietetic knowledge, and obvious to anyone who
has bred Utters of puppies. ... It is now general knowledge that cereals as a
whole are very poor in calcium and rich in phosphorus. For instance, 150 grains
of white bread will contain approximately 0.03 grans of calcium and 0.14 of
phosphorus, which give a Ca : P ratio of 1: 4.6 ; similarly 150 grains of
oatmeal will contain approximately 0.1 Ca and 0.588 P with a ratio of 1 : 5.9,
and so on all through the cereals. The essentially carnivorous dog is forced in
this experimental work to obtain over 50 per cent, of its energy requirements
from cereals which contain the essential salts for calcification in a ratio very
different from that required in the ideal dietary. The dietary is an ideal
high-phosphorus-low-calcium rachitogenic one without any necessity to postulate
a harmful substance in the cereals. . . . " It is remarkable that ' increased
oatmeal' in diet 4 is only 51 grains, or only 2 grams per kilogram of body
weight. As oatmeal is especially singled out for its malign influence on the
deposition of calcium, it appears somewhat remarkable to me that the crofters
and farm labourers of North East Scotland should have any teeth or
straight bones in view of the shockingly large amounts of ' toxamine ' they have
absorbed for years, including their growth years. I can assure Mrs. Mellanby
that I have lived in a bothy and have seen the teeth these men have and the
porridge they eat. As a group, they are very superior to the townspeople in
every particular, oatmeal and milk is far more important in their dietary than
potatoes and meat.
" Examination of Mrs. Mellanby's work as a whole and of the latest human
experiments in particular shows that the dietaries used are not comparable, and
such misleading basal facts have led her into her anti-cereal theory."
7. HOW DIPHTHERIA ANTI-TOXIN IS MADE
Horses are prepared for this by a course of gradual poisoning with the throat
excretion of diphtheria patients. A little of this poison is administered at the
first injection, but day by day the dose is increased until the horse is almost
ready to fall from weakness ; then the blood tappings begin. The animal's head
is stoutly, often painfully, secured ; then two laboratory assistants select a
point in the left side of the horse's neck immediately over a large blood
vessel, and suddenly a sharp-pointed half-inch tube, some twelve inches long, is
driven by main force into the horse's neck. The animal shudders and trembles,
his breathing is short and quick. The first plunge (if successful) enters the
blood vessel, and a stream of blood flows through the tube into a receptacle.
The amount taken is from two to three gallons, and the process is repeated
weekly until the horse is exhausted ; then the animal is usually sold. The Truth
Teller reports that a horse costing only $15 had eight
quarts of blood drawn from him every week for four years, having earned $75,000
in that short time.
Here follows a sworn statement secured from a former employee of the Rockefeller
Institute:
" // Dr. Joiling or Dr. Flexner came near the horses they would prick up their
ears and move back and forth, and seem to be afraid of them. They use the
twitch, which is a cruel thing they use on the upper lip, to keep them still.
Horses would rather stand the bleeding patiently than have the twitch.
" Horses suffered a great deal after the inoculations. First, the horse was
inoculated ; two weeks later he was bled; two weeks after this he was again
inoculated. Then it would swell on the shoulder where he had been inoculated,
and a lump would form and the swelling would subside; afterwards the lump would
burst, and then there would be an open ulcer with the pus running down in a
steady stream all the time for about a week. That occurs with every horse they
inoculate for serum.
"The horses were in such pain that they would stand for hours without moving,
and when they did move they would utter sounds I cannot describe: I can hear
them yet ', 1 can never for get them; they were indescribable."
A well-known English doctor and member of the Royal College of Surgeons
describes the preparation of anti-typhoid vaccine thus :
" You have a ward full of men suffering from typhoid fever, and these men are
treated for it by the medical men who attend them, and who know perfectly well
that they are suffering from typhoid fever and from nothing else. . . . The
medical men in attendance have to take a
portion of the excreta (from the intestines) of every one of these patients and
put it into a bottle labelled with the name of the patient, and . . . send it
into the bacteriological laboratory. The men in the laboratory, many of whom
could not tell a case of typhoid fever if they saw one, at once begin to submit
this excreta to a bacteriological or chemical test, commonly called the
agglutination test, which is as fallacious and untrustworthy as is the whole
system to which it is attached. The mass of filth is then injected into horses,
poisoning their blood. From this poisoned blood they obtain the vaccine, with
which they poison those into whom it is injected."
In A System of Bacteriology (Wadsworth), Vol. Ill, p. 356, a horse is stated to
have been subjected to 161 bleedings over a period of nine years, the amount
withdrawn on each occasion having been about 8 litres.
The price lists of English manufacturers of anti-tetanic serum give one shilling
and sixpence for a 2cc. dose, so that the retail value of the quantity produced
from this one horse would be between forty and fifty thousand pounds!
In the Official History of the War (Section Pathology) it is stated that "
tetanus bacilli " have been found in twenty per cent, of war wounds although no
symptoms of tetanus were present, whilst in 50 per cent, of definite tetanus
cases no tetanus bacilli were discovered.
" The whole theory of the treatment of tetanus with serum," writes Dr. Beddow
Bayly, M.R.C.S., " is based on this primary contradiction; that a germ which is
harmless in pure culture, incapable of multiplying in
the body, absent in half the cases of disease, and present frequently in cases
which never develop it, often remaining in the tissues for months and years
without causing any ill-effect, is regarded by medical science as the sole cause
of tetanus."
" Tetanus," writes Drs. Bosanquet and Eyre (Serums, Vaccines and Toxins, 1916,
p. 146), " is too uncommon a disease for statistics of it to be of value."
" There was another chamber of horrors at Mulford's we were not allowed to see.
That was in the little green building pointed out as the place where tetanus
antitoxin was made. Ugly stories were heard in the vicinity, however, of horses
with lockjaw lying on the stable floor, kicking and writhing themselves to
death." Seen and Heard in a Vaccine Plant. Lora C. Little.