Let’s Talk About Whooping Cough
http://vaxtruth.org/2015/01/pertussis/
Author: Marcella Category: Vax Facts
Let’s talk about those whooping cough outbreaks, shall we?
And while we’re at it, can we talk about DTaP? The Diptheria,Tetanus and acellular Pertussis vaccine? We have to. Because that’s what’s causing the outbreaks. I’m betting at this point 98% of those on the pro-vaccine side have stopped reading. It astounds me how many people have made up their minds, and they seem to think they “know” everything there is to know about the whooping cough outbreaks and DTaP/TDaP vaccines. I could be wrong about this, but it appears that many listen to Paul Offit as if he is a “prophet,” and they don’t feel the need to think for themselves or look further. When we are talking about science, and the human body, I just don’t see how we can ever say there is nothing left to learn. The fact that we never know everything there is to know is the basis of scientific inquiry – and that includes science that influences the medical decision-making process. For those who are still with me, thanks for sticking around and for being brave enough to use your own intellect and the discernment God gave you. Here we go…
The first thing I want to say about the acellular vaccine is that the reason it was developed in the first place was because the whole cell pertussis vaccine was so dangerous and too many babies were dying. SIDS, or Sudden Infant Death Syndrome was one of the most serious adverse events following vaccination with the whole cell pertussis vaccine. Prior to the establishment of the 1986 Vaccine-Injury Compensation Program (VICP), parents whose children were seriously injured or killed by vaccines could pursue legal action against vaccine manufacturers. There were so many lawsuits being filed that vaccine makers basically held the U.S. federal government hostage and threatened to stop making vaccines altogether if the government didn’t step in and protect them from lawsuits. And that is why now, if vaccines injure or kill your child, you cannot sue the vaccine manufacturer. For more information on the history of DTP, please go here and here.
So… it was known that the DTP (or DPT) vaccine was very dangerous.
In 1991, the first DTaP vaccine was licensed in the U.S. on the premise that the acellular version would be safer and would produce fewer side effects and deaths than the DTwP (whole cell) version of the vaccine. There are two versions (and multiple producers) of the acellular vaccine. DTaP is given to infants and children up to age ten. TDaP is given to persons who are 10 and older, including adults. Much of the information in this post refers to both DTaP and TDaP, as they are both acellular pertussis vaccines.
Safety studies for the DTaP vaccine are problematic in that the new vaccine was tested against the old vaccine. There was no true placebo group. This is common practice in vaccine safety studies. Other problems with the clinical safety studies include the use of unequal numbers of subjects between groups, and very short follow-up of participants; generally 3-4 days post-vaccination. It is also noted that in the clinical trials there is a consistent rate of attrition (children who dropped out or were removed from the study by their parents), which resulted in fewer and fewer participants as the studies progressed. There is no mention in the vaccine-manufacturer’s inserts as to why the children were removed from the study. We can speculate that one possible reason for parents pulling their child from a study might be due to the child having an adverse reaction, and the parent not wanting to take that risk again, but that would just be speculation on our part. There is some evidence to suggest this may be the case, judging from the fact that in the clinical trials, the percentage of children who experienced systemic reactions increased with each successive vaccine in the series. In other words, the percentage of children whose parents reported adverse reactions was higher at doses 4 and 5 than at doses 1 and 2. To review this information for yourself, you can obtain the vaccine manufacturer’s inserts here, with the exception of the Tripedia insert, which is no longer available on that site. It can be obtained here. I wrote a piece a while back on the Tripedia vaccine, which some folks will tell you is no longer being used in the U.S. This is incorrect. It is still used and is now being combined with the HiB vaccine to form ActHIB and TriHiBit. Just an FYI…
One other little tidbit of information about Tripedia… while you have the manufacturer’s insert up on your computer screen, go to page 11. You will see this:
Adverse events reported during post-approval use of Tripedia vaccine include idiopathic thrombocytopenic purpura, SIDS, anaphylactic reaction, cellulitis, autism, convulsion/grand mal convulsion, encephalopathy, hypotonia, neuropathy, somnolence and apnea. Events were included in this list because of the seriousness or frequency of reporting. Because these events are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequencies or to establish a causal relationship to components of Tripedia vaccine.”
Again, when you are using small groups in your clinical trials and only following them for 3-4 days after the vaccine, it’s no wonder you can’t make reliable estimates about what really happens when you give the vaccine to four million infants each year, as if they are all the same.
So… that’s a little history about how we came to have the acellular version of the vaccine and why.
As a result of issues just discussed, there really isn’t a lot of evidence that the DTaP is much safer than the DTP. When we are making decisions about whether or not a medical intervention is appropriate for our children or for ourselves, we need to do what’s called a cost-benefit analysis. Basically what we need to know is:
1. What are the reported risks (cost) of the intervention?
2. What are the reported benefits of the intervention?
3. Based on the evidence, do the benefits outweigh the risks?
When doing a cost-benefit analysis, we also must take into consideration individual differences and family history. Anyone who has ever worked in a clinical practice where patient safety is valued will tell you the importance of individual and family medical history, when considering whether or not a patient is a good candidate for medications or for invasive medical procedures. Good doctors won’t prescribe birth control pills to young women with a history of blood clots. They won’t prescribe certain medications to children who have epilepsy. Even over-the-counter medications are not safe for everyone, as anyone with high blood pressure and a head cold will tell you. Good doctors realize there is nothing in medicine (no prescription, no procedure) that is safe for 100% of their patient population, and they realize the importance of taking the time and exercising caution before prescribing or recommending any medication or procedure. It’s called patient care.
When it comes to childhood vaccinations, patient care goes out the window and it’s all about patient compliance. If we listen to Paul Offit we are all supposed to ignore family medical history and genetics, and line up and do as we are told. Dr. Offit is a vaccine-extremist. He has stated that infants can receive 10,000 vaccines in a single day without any problem. In this most recent propaganda piece from Australia, Dr. Offit also appears to express the view that parents who wish to exercise caution or who choose not to vaccinate their children should have their kids taken away by the state. I don’t know about you, but I don’t want someone that extreme making decisions about my child’s healthcare. And while we’re on the subject of Dr. Offit, it should be known that he holds a research chair position at Children’s Hospital of Philadelphia and his salary is paid by Merck – the maker of a number of vaccines given to children. I don’t know what his current salary is, but a few years ago it was reported to be $1.5 Million per year. I doubt he is making less money these days, given that his position as the voice of universal vaccination has only become louder and more extreme since that time. Dr. Offit also developed a vaccine for rotavirus – and the patent for that vaccine sold for a reported $182 Million. But, I’m sure, when it comes to the vaccination of 4 million children per year, with vaccines that sell for anywhere from $10 to $100+ each, the money is not an influence at all. RRRRiiight. (insert eye-roll)
Let’s start with the reported benefits of the vaccine. According to the CDC, the vaccine is safe and effective. If we believe what the CDC tells us, the vaccine will protect us and is the best thing we can do to ensure our children, especially our infants, are protected. According to this Whooping Cough Fact Sheet, there were 255 deaths from whooping cough in the United States between 2000 and 2012, and 221 of those deaths occurred in infants under three months of age.
Now let’s look at the risks part of our Risk-Benefit analysis of the DTaP vaccine. I should clarify that when assessing risks, this can be stated in terms of the known or reported risks of the DTaP vaccine. When trying to figure out the true risks, there are some problems; chief among them the fact that we don’t have accurate data to assess.
The only database we have is the Vaccine Adverse Events Reporting System (VAERS), which is maintained by the U.S. Department of Health and Human Services. The problem is, even though the 1986 Federal Law states that it is mandated for physicians and other health providers to report known and suspected adverse reactions to vaccines, they aren’t doing it. Estimates by the AMA indicate that less than 10% of adverse reactions is reported to VAERS, and the number may be as low as 1-2%. So, when we look at those numbers, we need to remember that the actual number is much higher.
Since VAERS is all we have to go by, what do those numbers look like?
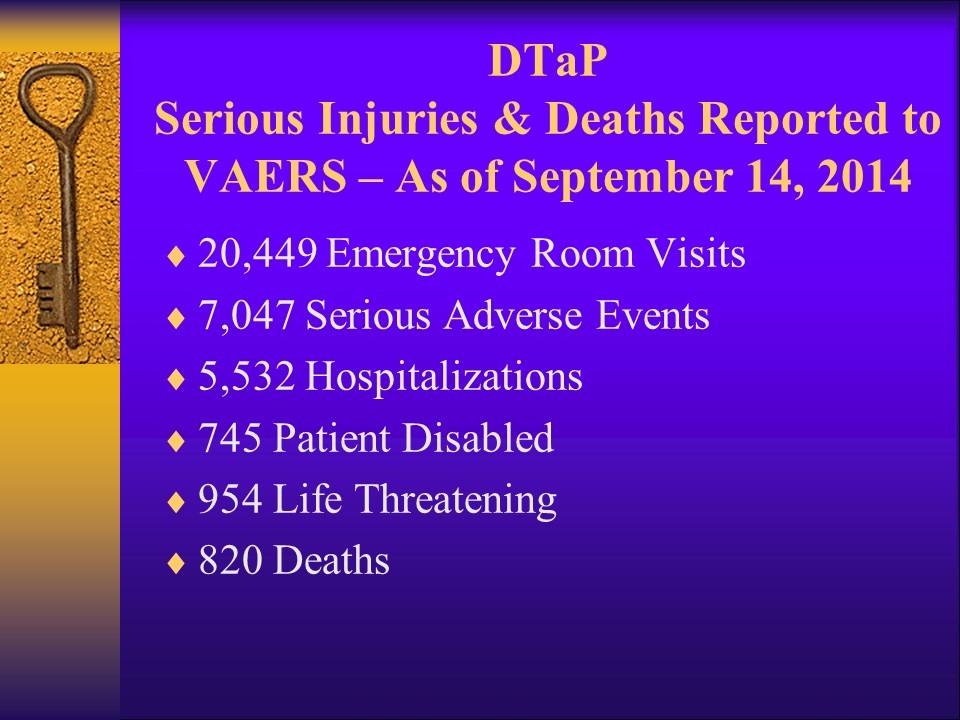
These numbers are from a search I did in October of 2014:
The VAERS database is updated in 3 month cycles.
These are the numbers today (01/06/2015), after the most recent update:
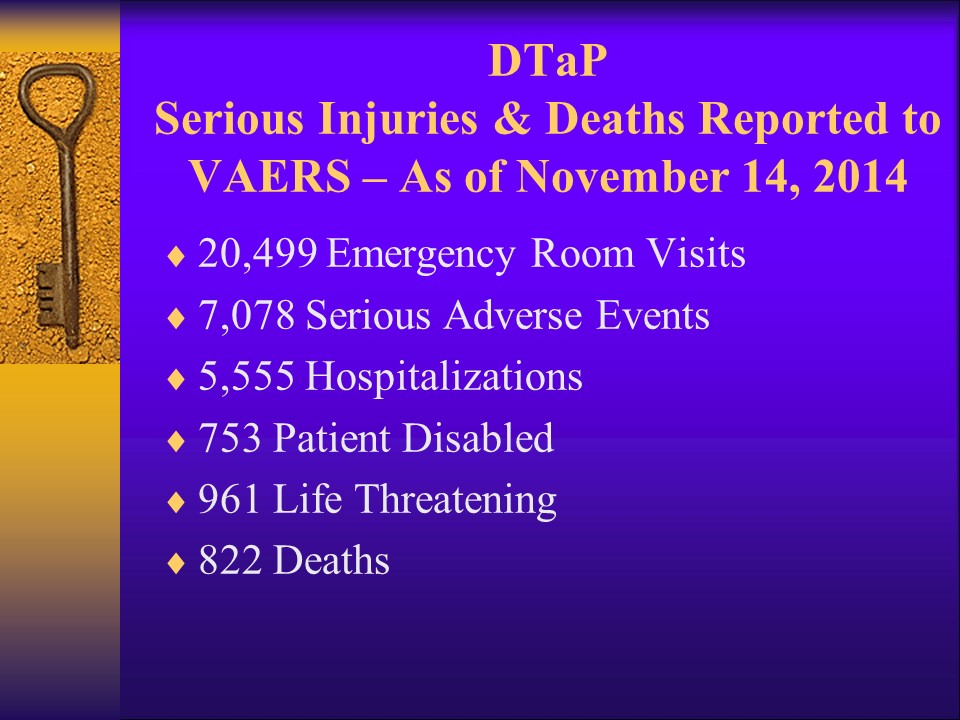
These numbers represent the total number of adverse reactions reported to VAERS, since the DTaP was licensed in the early 1990s. Remember, these numbers are very likely to be a small fraction of the real number, due to severe under-reporting by doctors, nurses, and pharmacists. Parents can also report adverse reactions to VAERS… if they know about it and if they are able to jump through the hoops to do so.
Please notice that in three months’ time, there have been:
This is what was reported to VAERS as adverse reactions to the DTaP vaccine, in just 3 months. This does not include reactions reported for TDaP, so the numbers here ONLY include severe adverse reactions in children ten and under.
Let’s look at the numbers for TDaP:
.jpg)
Why are the numbers for TDaP so much lower than for DTaP? There are probably several reasons, but the two most important are that TDaP was only licensed in 2005, so DTaP has been around much longer. The other really big reason is that it wasn’t until just the last few years that TDaP has been strongly pushed on adolescents and adults – this is in stark contrast to DTaP, which is administered five times to every infant and child born in the United States and vaccinated according to the CDC’s Childhood Vaccination Schedule. More vaccines given = more serious adverse events and deaths.
So, if we total the number of deaths from the acellular pertussis vaccine (just those that have been reported to VAERS), that number is 871.
871 deaths reported to VAERS from the acellular pertussis
vaccine.
One reason why people die from the vaccine is anaphylaxis – a severe
allergic reaction to a component of the vaccine. The vaccine-manufacturer’s
inserts warn about this, and they state that anyone who has had a previous
severe reaction or who has a known allergy to ANY of the vaccine’s ingredients
should not receive the vaccine.
How many people do you know with milk allergies? There are a lot of them. Did you know the DTaP and TDaP vaccines contain milk protein? Neither did I until my daughter had a severe reaction. She has a milk allergy.
This article reports on the observations of a group of physicians who witnessed several cases of anaphylaxis in their patients following administration of the DTaP vaccine. (Note: The online report states the children received DPT vaccine. This is an error, since the DPT vaccine was no longer in use in the U.S. at the time.) The doctors presented their observations at an annual meeting of the American Academy of Asthma, Allergy, and Immunology in 2011. What I find most interesting is that initially, the doctors (who are trained in allergy and immunology) were at first shocked to find milk protein in the vaccines they tested. They thought it was due to contamination. They knew that food proteins are not supposed to be injected into the body – they’re supposed to go through the gastrointestinal tract where they can be appropriately broken down. Well, guess what? It wasn’t contamination. The bacterial components of the vaccine are cultured on casamino acids – milk. This problem has been known since at least 2011. Have you heard anything about it? Has your doctor asked if you or your child have a milk allergy before recommending the DTaP or TDaP vaccine? Our doctor knew of my daughter’s milk allergy, but he recommended (pushed) for her to get the TDaP anyway. Why would he do that? He didn’t know. He had never read the manufacturer’s insert.
Going back to our Cost-Benefit Analysis and the questions: “Is the intervention beneficial, and if so, do the benefits outweigh the risks?”
We have already heard what the CDC has to say. “Vaccines are GREAT! Vaccines save lives! Line up and get your vaccine!”
As thinking people, we need to dig deeper and see if what
we are being told is true.
In other words… Does the vaccine REALLY work? We are told it does,
and we are also told we need to get the vaccine in order to protect “herd
immunity.” Unfortunately, there is no evidence that “vaccine-induced herd
immunity exists.” It’s a theory. Let’s think about this theory for a few
moments…
Pro-vaccine folks who try to shame you into vaccinating to protect “the herd” often state that we have to have 90-95% vaccine coverage in order to prevent outbreaks of infectious diseases. How many of you reading this are over the age of 30? I am. I’m 54. My last DTP vaccine was in the fifth grade. When I was a kid, teenagers, college students and adults were not targeted for vaccination, so after I got my fifth grade booster shots, that was it. The same is true for most adults my age. That being the case, and given that at least 50% of the adult population has been walking around with ZERO vaccine-induced immunity for years (since we now know vaccines wear off in 3-5 years, if they work at all), that kind of shoots down the whole “herd immunity” argument, doesn’t it? There IS actually something to the herd immunity thing, and it used to be a real benefit to infants and young children whose mothers had natural immunity from the childhood illnesses they caught and fought through. That natural immunity was conferred to infants during their first year of life, and they were protected from things like measles and whooping cough. So, while it is true that vaccines have had an effect on herd immunity, it has not been a positive one. You can read more about herd immunity in this article from neurosurgeon Dr. Russell Blaylock.
In spite of the evidence (and common sense) telling us that vaccine-induced herd immunity is a load of whooey, we have all heard the reports on the morning talk shows and we have seen the news stories blaming unvaccinated children and their parents for outbreaks of pertussis. We need to take a deep breath and see just how likely this is to be the case. One way of doing that is to see if there are other explanations for what is going on.
According to this study, the number one bacteria that causes whooping cough is mutating. (Any bells going off yet?) Where have we heard THAT recently? Hint… The CDC says the 2014-2015 flu vaccine doesn’t work as well as in most years because the flu strain is mutating. That’s what viruses and bacteria do. They have been around since the dawn of time and they are very resilient. They will change and mutate in order to survive. Does this surprise you? It shouldn’t. If you’ve ever taken an antibiotic for a bacterial infection, think back to what the doctor told you. It probably went something like this…
Be sure to take this antibiotic for the entire 7-10 days, and take it exactly as prescribed. Do not stop taking it when you feel better. If you don’t take it exactly as prescribed, it can cause the bacteria to change (mutate) and become resistant, and the next time you need the antibiotic it may not work.”
(Light bulb yet?)
Here’s the thing… If a bacteria can change to avoid eradication over the course of a 7-10 day administration of antibiotics, how are we supposed to believe a vaccine developed in 1991 against one strain of multiple bacteria that cause pertussis is still effective?

Ah! There it is! Light bulb moment!
Yep. At the time when the DTaP was developed in 1991, Bordatella Pertussis was the major problem bacteria that was causing whooping cough. However, it is not the only bacteria that CAN cause whooping cough. That means the DTaP is a “partial coverage vaccine.” Partial coverage just means there are other types of either viruses or bacteria that can also cause the disease in question. Right now, we’re talking about whooping cough. Other partial coverage vaccines include the pneumococcal vaccine, the flu vaccine, the meningococcal vaccine, and the HPV vaccine.
One thing that happens with partial coverage vaccines is that when the vaccine only covers one or a few strains and doesn’t cover the others, those that are not covered can (and do) become stronger. Those that are not covered can (and do) start to cause disease outbreaks when they didn’t or at least not as much, or not as serious, as before the vaccine became widespread. This has happened with the prevnar vaccine (for pneumococcal disease), and it’s why there are now three different versions: Prevnar7 (with 7 strains of streptococcus bacteria), Prevnar13 (with 13 strains of streptococcus) and Prevnar23 (with 23 strains of streptococcus). As the strep strains that are not covered in the vaccines become more problematic (this is known as “shift”), vaccine-developers have to keep going back to the drawing board (laboratory) to make new vaccines to cover more strains. Here is an article from the peer-reviewed medical literature that describes this issue. Of note… it’s not just too many vaccines at work. It’s also too many antibiotics. The overall issue is the bacteria are mutating and they are becoming more virulent and are more likely to be resistant to antibiotics. This is not a small issue. And it’s not because children aren’t getting enough vaccines or enough prescription medications. It’s because they are getting too many.
The pro-vaccine folks are probably rolling their eyes and screaming at the computer (or phone), “You don’t have any proof of that!”
Read on…
Let’s look at some very recent studies that have been done in the laboratory, using non-human subjects. Yes. Non-human subjects. Why? Because that’s where the research is being done. As far as Dr. Offit and other pro-vaccine folks are concerned, the questions have all been asked and answered and we don’t need to look any further. Unfortunately, that’s not the way science works. That’s the way religion works.
As Dr. Bernadine Healy (former head of NIH) stated to Sharyl Attkisson in a 2008 interview for CBS, we need to look at the research being done in animal models and not discount that research just because it doesn’t agree with the already-decided stance of those who benefit financially from the sale of vaccines. When we are talking about animal models and research, there are some that carry more weight than others, simply due to the fact that human beings share more DNA with certain animals (primates) than with others. I’m sorry if that offends anyone, but it’s a fact.
At this point, I’m going to take a little side-trip and discuss one animal-model study which, although it does not have anything to do with whooping cough, is a very good study to illustrate certain points.
This study, published in 2010, investigated the effects of the infant vaccine schedule (the one given to infant humans – the one Paul Offit wants to mandate without exemptions or exceptions for individuality), when adjusted for weight and given to infant macaque monkeys. The researchers used macaques because they share 93.5% of DNA with humans. In this study, the researchers divided the infant macaques into two groups. Unlike vaccine studies conducted with human participants, this was a true experimental design, with one experimental group (those who got vaccines) and one placebo group (those who didn’t get vaccines). Here are the results:
.jpg)
So, there you have it. In a true experimental research study of vaccinated vs. unvaccinated infant macaques, those that were vaccinated developed physiological symptoms consistent with what is often seen in children who have suffered reactions to vaccines and were later diagnosed with autism. Baby macaques in the placebo group, who were not vaccinated, did not.
Back to the DTaP…
As is discussed in this peer-reviewed scientific article, there are some animals that are more useful than others when we are talking about experiments investigating human physiology. Mice are often used. Baboons are the most preferred because they share 91% of DNA with humans, and therefore we can make stronger assumptions about whether or not the results of research can be applied to human beings.
So, what are we learning from the baboon studies?
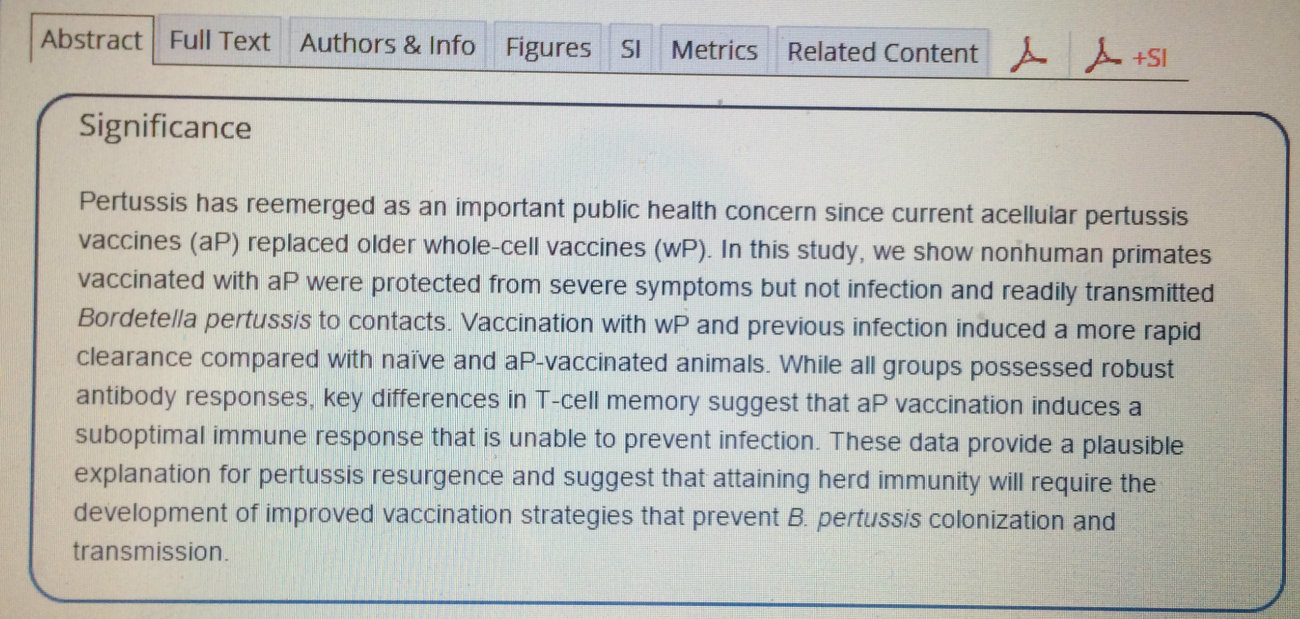
According to this study, baboons who are vaccinated with the acellular pertussis vaccine can still harbor the bacteria in their throats (with or without symptoms) and spread it to others.
WHAT???
Yes. Vaccinated baboons can spread pertussis to others EVEN WHEN THEY HAVE ZERO SYMPTOMS.
Let that soak in.
Now… think about the practice of “cocooning.” Cocooning is the insane practice of vaccinating family members of infants (0ften before the infant comes home from the hospital), under the premise that in doing so, the infant will be protected from getting whooping cough. Tiny infants are the MOST vulnerable to serious outcomes from pertussis. If the findings of non-human primate studies hold true… cocooning is probably THE MOST dangerous thing that can possibly happen, from the vantage point of the tiny infant.
Now think about this…
If an unvaccinated child has pertussis, parents will know it and can take steps to stay away from newborns. If the results of this study hold true for humans, a vaccinated child or adult can hug and kiss a newborn and spread pertussis without even realizing it. If the results are true for humans, it also means the more people are vaccinated with the DTaP or TDaP vaccine, the more likely they are to be contributing to the outbreaks of whooping cough. Could that be why, in recent history, every single pertussis outbreak has occurred in populations where the percentage of vaccinated individuals is higher than the national average? Whip out your common sense meter here.
Still not convinced? Okay… Let’s dig some more.
Remember when I told you that Bordatella Pertussis is only ONE of multiple strains of bacteria that cause whooping cough? And remember when we talked about “shift” and how those strains not covered in the vaccine can become more problematic? So far, we’ve been talking about evidence from non-human studies. As you are probably aware, the biggest and most widely publicized “pertussis outbreaks” have been in California. (“Pertussis” is in quotes, because according to the California Department of Public Health, it’s not just Bordatella Pertussis that’s causing the outbreaks.)
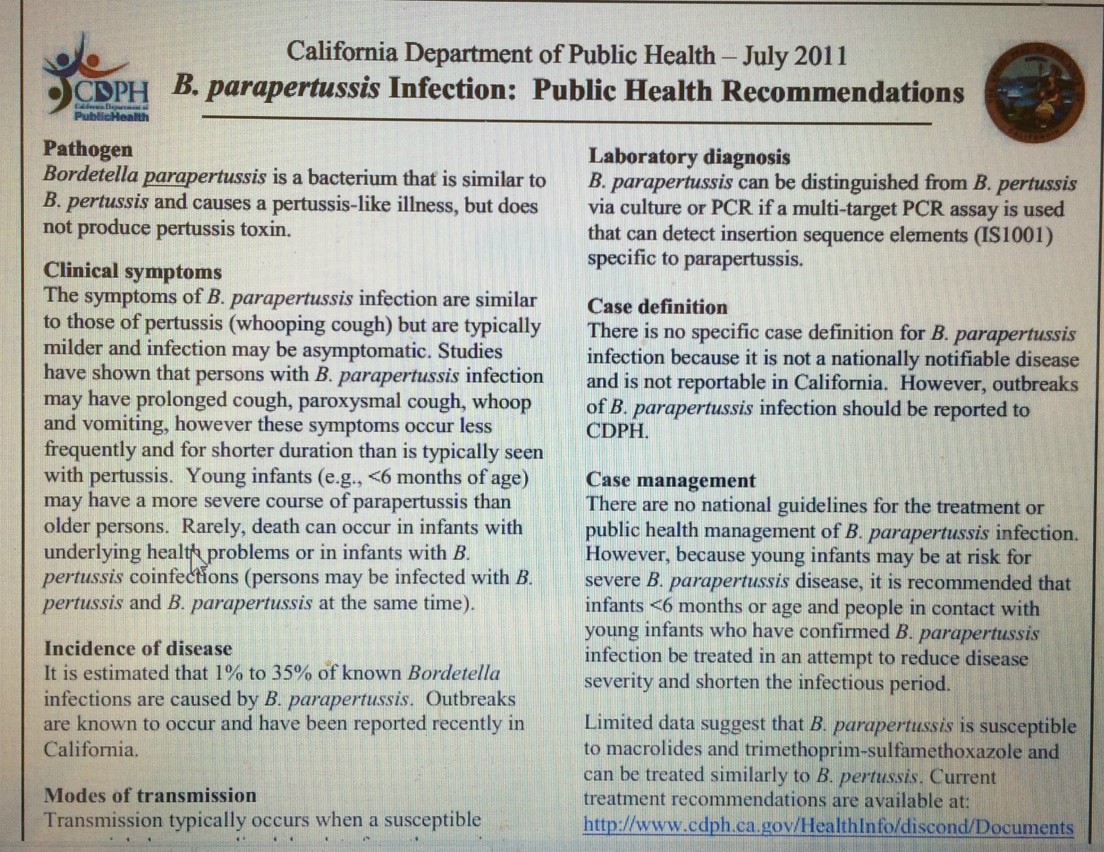
See that little blurb under the heading of Incidence of disease ???
It is estimated that 1% to 35% of known Bordatella infections are caused by B. parapertussis. Outbreaks are known to occur and have been reported recently in California.”
I’ll give you a moment to absorb that. I know it’s difficult. This is completely different from everything we’ve been told by the mainstream news sources so many of us rely on. Not to sound like your mother, but… “Don’t believe everything you hear on television. Especially when each 60 minute news cast has between 5-10 commercials for pharmaceutical products.” Yep. Just like Paul Offit, your “news” is bought and paid for by the pharmaceutical industry. Shocking. I know.
So, if up to 35% of whooping cough cases are being caused by B. parapertussis, what could be causing what appears to be an increase in those cases? For this one, we don’t have human studies, and we don’t have primate studies. We have a mouse-model.
Their data showed no within-host competition between B. pertussis and B. parapertussis, as well as a strong acellular vaccine-induced protection against infection with B. pertussis in both singly and co-infected mice. In contrast, VACCINATION LED TO A 40-FOLD ENHANCEMENT OF B. parapertussis COLONIZATION IN THE LUNGS… It is speculated to involve specific immune responses skewed or dampened by the acellular vaccine…”
This research from the Center for Infectious Disease Dynamics at Penn State University STRONGLY suggests that, despite what you are being told about how the unvaccinated are spreading disease, the opposite is true, and it is THE VACCINATED who are infecting each other through a combination of factors, including vaccines that don’t work, and which cause the development of new, more virulent strains of bacteria and viruses, which are spreading in the absence of symptoms, and which are greatly increased in the lungs of vaccine recipients WHEN THEY ARE VACCINATED.
There.
I’m so glad we’ve cleared that up.
Please. Educate yourself about vaccines before you vaccinate your children. If you choose to vaccinate, do not do it because you are fear-mongered or guilted into it. Consider where your information is coming from, and who is paying to ensure what information you receive. And remember, if something happens to your child, Dr. Offit won’t be the one paying for the funeral or for the life-long care of your child. You will.
Read more:
Healthy Children and Adults Vaccinated with Flu Shot are Dying
#CDCwhistleblower to Hit 1 BILLION TWEETS – Be Part of This!