WHOOPING COUGH: THE DISEASE AND THE VACCINE
By Dr Jayne L M Donegan (June 2000 The Informed Parent)
Whooping cough is a childhood illness caused by infection with the ‘bacterium Bordetella pertussis. It is spread by droplets in coughs and splutters. There is normally an incubation period of two weeks (when you are infectious without symptoms), a ‘catarrhal’ phase of two weeks, a paroxymal or ‘whooping’ phase of two weeks and a recovery phase of two weeks. These may all vary in length and the more dangerous whooping phase may be absent altogether.
In the catarrhal phase there is mild fever, a runny nose and the start of a hacking cough that may keep the child awake at night. The cough then starts coming in spasms as we enter the paroxysmal phase. There is repeated coughing without drawing breath, mucus and saliva stream from the nose and mouth. He/she may vomit their last meal with mucus while coughing. Young children and babies may go quite blue with bloodshot eyes. Then comes the long ‘whoop’ as the child breathes in. After a series of these they may fall asleep, exhausted.
Looking after someone during this phase is particularly tiring and time consuming. They must be kept calm and quiet as excitement and exertion provoke the coughing attacks. During a spasm of coughing the child should be held in the recovery position to avoid the inhalation of vomit. Some small babies require suction and oxygen after a spasm has ended. It is important to make sure that they get enough to drink - the best time to offer fluids is after an attack as it is less likely to be vomited.
During the last fortnight the symptoms usually start to resolve. The whoops and the vomiting become less frequent so the child sleeps more at night and starts to regain weight. After recovery, a cough or cold during the following year may start off a series of whoops as will exposure to cigarette smoke.
Although it is difficult to diagnose whooping cough in the first week because it is so like an ordinary cough or cold, the standard advice is that antibiotics given at this time will reduce the severity and duration of the illness, and giving them to siblings who have no symptoms may reduce spread to others.
Babies less than one year old usually have the most severe forms of the disease and it is in this age group that deaths most often occur. They may have convulsions at the end of the coughing spasm and in rare cases may actually have a brain haemorrhage (bleed) which may cause temporary or permanent brain damage.
Areas of the lung may collapse leading to bronchiectasis (dilated bronchioles filled with mucus) if re-expansion does not occur.
Another complication of the disease is pneumonia, again, more common in babies and a major cause of death.
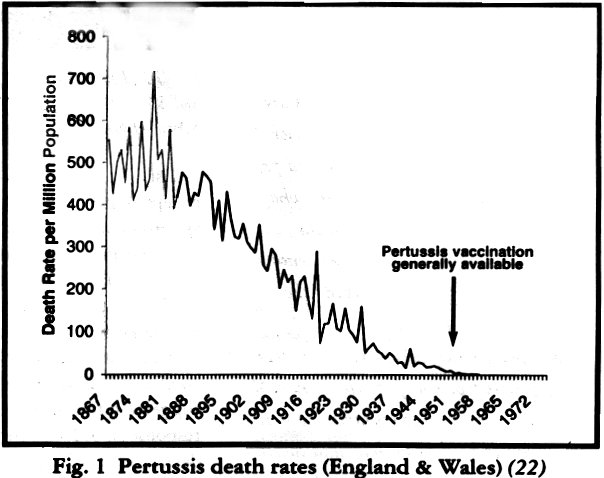
In the nineteenth century whooping cough was most definately a killer disease. "Deaths from whooping cough remained at around 10 000 a year from 1847 until the 1900s and then declined steeply as the health and care of children improved and had reached less than 400 a year by 1950. Immunisation started in the 1950s, deaths continued to fill and notifications fell sharply." (1)
It is undoubtedly the case that whooping cough became a milder disease in this country over the course of the first half of the twentieth century. The death rate had fallen by over 99% before vaccination against pertussis was introduced in the 1950s (Fig 1). The introduction of the vaccine reduced the number of notified cases of whooping cough but peaks continued to occur every three to four years as they always had. Deaths continued their steady decline. This was most clearly seen in the 1970s and 80s when the vaccine coverage fell to less than 40% in 1976 because of health scares. In 1978 and 1982 there were over 65,000 notified cases of whooping cough but no concomitant rise in the number of deaths (Fig 2). Between 30% and 70% of children in outbreaks are vaccinated (2,3,4).
Does the vaccine cause brain damage? A paper published in 1974 described neurological complications of pertussis vaccination (5). This caused widespread panic among parents and some health professionals. In order to investigate the matter, the National Childhood Encephalopathy Study was set up which looked at all ‘serious neurological events’ occurring in children aged two to thirty five months between 1976-79 and matched them with ‘controls’ who had not had such an event (6). It was a bit of a strange study in that it did not look at the number of children in the ‘event’ or ‘control’ group who had been vaccinated against pertussis compared with those who had not, but only at the numbers who had been vaccinated against pertussis in the seven days before the neurological event. This means that a child could have had a serious neurological reaction two or three weeks after pertussis vaccination and this would not have been included in the ‘pertussis vaccine’ figures. As we know, one of the major problems encountered by parents who believe that their children have been damaged by vaccines, is that symptoms coming on more than 72 hours or, in this case, seven days, after vaccination are discounted. Anyway, even with this improbable time frame, it was shown that those with severe neurological damage were 2.5 times more likely to have been vaccinated against pertussis in the seven preceding days than the ‘controls’. The numbers were small but significant. A follow up study ten years later showed that those children who had since died or had neurological dysfunction were four times more likely to have been vaccinated against pertussis in the seven days preceding their original illness. As some of the neurological dysfunction was considered to be quite mild, a reanalysis was carried out which included only those children with more severe dysfunction and death. These children were 7.3 times more likely to have been vaccinated in those seven days (7).
Fine and Chen pointed out that those being vaccinated against pertussis should be less likely to succumb to a neurological illness because those with fever, previous reaction to pertussis vaccination, family or personal history of epilepsy or pre-existing neurological impairment were generally advised not to be vaccinated. Taking this into account should make the association with pertussis vaccination stronger, which indeed it does (8).
A similar case-control study in the U.S. found an association between pertussis vaccination and neurological damage (9). The Institute of Medicine in America published the results of its study into the ‘Adverse consequences of perrussis and rubella vaccinations’ in1991 (10). It found evidence consistent with a causal relation between DPT (diphtheria, pertussis and tetanus) vaccination and acute encephalopathy, shock and ‘an unusual shock-like state’. It found no evidence to accept or reject a causal relation between DPT vaccination and chronic neurological damage, Guillan-Barre syndrome, learning disabilities, attention-deficit disorder and peripheral neuropathy. All these studies and reviews of them say that the risks of the vaccine are small and where the evidence is not sufficient to either accept or reject a causal association the conclusion is that we should regard this as proof that the vaccine is safe and encourage parents to carry on vaccinating their children (11).
In 1994 Dr Michel Odent published a retrospective (looking backwards) study in which he compared the incidence of asthma in 243 children who had been vaccinated against pertussis with 203 who had not. Vaccinated children were over five times more likely to suffer from asthma and twice as likely to have had ear infection than unvaccinated ones (12). In 1997 another retrospective study of 1934 patients born between 1975 and 1984 from one general practice in Oxfordshire showed that children vaccinated against pertussis were 75% more likely to develop asthma, hayfever and eczema later in life (13). A larger prospective (looking forward) study of 9,444 children in Avon failed to show such an association but the children have only been followed up for 42 months so far. It will be interesting to see the results of further follow up (14).
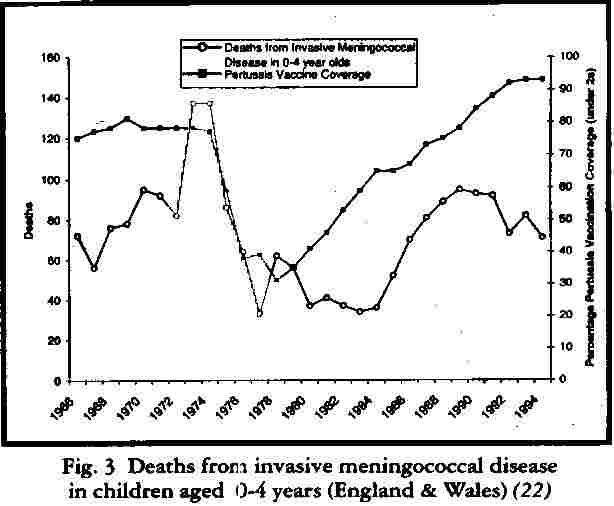
Questions have also been asked about the incidence of invasive bacterial infection in children who have recently been vaccinated against pertussis. Certainly in the ‘natural experiment’ that took place in this country when the acceptance of the vaccine fell so dramatically in the mid 1970s to the mid 80s there was an accompanying fall in the number of deaths of children aged four years and less from invasive meningococcal disease. The numbers began to rise again as vaccine uptake increased (Fig 3).
Is the acellular pertussis vaccine safer than the whole-cell one? The Americans, Swedes and Japanese certainly seem to think so. The Swedes abandoned the whole cell pertussis vaccine in 1979 because of worry about side effects and because of its perceived ineffectiveness as whooping cough swept through its population of whom the majority were fully vaccinated. The Japanese raised the vaccination age to two years in 1975 after a number of reports of severe reactions and deaths. This simple measure reduced the total number of deaths in infants younger than one year. In 1981 Japan introduced the acellular vaccine.
A Swedish trial of one and two component acellular pertussis vaccines in 1986-87 compared vaccine to placebo. It concluded that side effects of the new vaccine were mild. The placebo was the ‘vehicle’, the liquid which ‘carries’ the vaccine. It contains thiomersal (a mercury containing compound), formalin and aluminium phosphate. The side effects of the new vaccine compared to this ‘placebo’ were indeed minimal but, looking at the data, the most worrying factor was the incidence of floppiness, vomiting, inconsolable crying for more than one hour, fever and drowsiness that occurred after the ‘vehicle’ alone. The addition of the whooping cough component didn’t seem to make a lot of difference. It makes one wonder why the ‘vehicle’ in which we deliver the vaccine has to be so toxic (15).
A report from Canada presented to the Infectious Diseases Society of America in Philadelphia in November 1999 suggested that there had been an 80% drop in admissions for seizures and a 75% decline in collapse within 72 hours of being vaccinated since the acellular vaccine had been introduced in that country (16).
Clinical trials using acellular pertussis vaccines combined with diphtheria and tetanus began in the UK in 1994. Plans to introduce these vaccines were put on hold in 1995 when it was thought that they might react with the Hib (Haemophilus Influenza B) vaccine that was now mixed with DPT vaccine, and be less immunogenic than the whole-cell and cost more. Swedish trials of the five component acellular pertussis vaccine showed that it was as immunogenic as the whole-cell (17) and several countries combine the acellular vaccine with Hib in their vaccination programs. The acellular pertussis vaccine does cost more and the Dept of Health has continued to staunchly back the whole cell vaccine even though it was forced to purchase and distribute acellular vaccines during the shortages of winter 1999/2000. A spokesperson announced the return to the whole cell in March of this year.
Is the pertussis vaccine useful in preventing pertussis disease? During infection with Bordetella pertussis, the inhaled organism sticks to the little hairs lining the air passages. It is then able to multiply and cause the inflammation, mucus, pus and ulceration that so easily block the narrow airways of young ‘children and babies. During natural infection with pertussis, as well as the misery of the illness, IgG, 1gM and IgA antibodies are produced. These IgA secretory antibodies are crucial as they specifically stop the bacterium from sticking to the little hairs and multiplying. Vaccination against pertussis does not produce IgA antibody which is so important in protecting against further infection (18). It does, however produce IgE antibodies which are associated with allergic disease.
As we have seen, the incidence of pertussis death and disease was falling well before the vaccine was introduced in the 1950s. In 1978 the U.S. passed laws requiring proof of vaccination before school entry to increase vaccination uptake. This caused a recognisable increase in the incidence of whooping cough in that country and it has been rising ever since such that they now have five doses of pertussis vaccine in their immunisation program (19). By 1996 a study in California showed that 12% of adults with persistent cough had undiagnosed whooping cough (20). In 1990 the UK introduced an ‘accelerated’ schedule of vaccination to try to stem the rising tide of pertussis notifications (vaccination at 2months, 3m and 4m instead of the previous 3m,5m, l0m). Now, despite vaccination rates of 94% in under twos the incidence of pertussis has been increasing since 1995. Between 1995 and 1997, 10 of the 12 deaths from whooping cough were in babies under 2 months of age. As with a number of recent reports from the UK, USA and Australia, there seems to be a trend towards increasing numbers of deaths in very young children and a ‘waning’ of vaccine effectiveness in 1-4 year olds (21).
Our vaccination program seems to have produced generations of mothers whose poor quality vaccine antibodies are unable to protect their babies from whooping cough. They are contracting it and dying of it at less than eight weeks old. Placental antibodies from natural infection should protect children for that vulnerable first year, particularly if combined with breast feeding. Our one to four year olds, without the benefit of ‘natural’ boosting of their immunity from circulating wild disease are catching vaccine modified disease in increasing numbers. Our vaccinated adults are getting chronic coughs from it because they haven’t had natural infection in childhood. The high prevelancc of vaccination seems to be causing a drift towards a higher incidence of disease caused by the 1, 2 serotype which is more likely to be associated with complications and admission to hospital (21). And all this without worrying about whether pertusss vaccination causes an increased incidence of asthma, allergic conditions, ear infections, invasive bacterial infections or severe, permanent neurological damage.
The decision to vaccinate one’s child against whooping cough is certainly one that requires careful consideration.
REFERENCES
1. The Health of Adult Britain: 1841-1994 Vols 1,11 Ed Charlron,J, Murphy M. London. The Stationary Office, ONS 1997: 15.3.5.
2. Stewart GT. Re: ‘whooping cough and whooping cough vaccine: the risks and benefits debate.’ AmJ Epid 1984;119(1):135-9
3. Dirchburn RK. Whooping cough aher stopping immunization, BMJ 1979;1:1601-1603
4. Stewart GT. Vaccination against whooping cough. Efficacy versus risks. Lancet 1977; Jan 29 :234-7
5. KulenkampffM, SchwartzmannJS, WilsonJ. Neurological complications of pertussis innocularion. Arch Dis Child 1974; 49:46-9
6. Alderslade R, Bellman MH, Rawson NSB, Ross EM, Miller DL. The National Childhood Encephalopathy Study. In: whooping cough. Reports from the Committee on Safety of Medicines and the Joint Committee on Vaccination and Immunisation. London: HMSO, 1981:79-169
7. Miller DL, Madge M, DiainondJ, WadsworthJ, Ross EM. Pertussis immunisation and serious acute neurological illnesses in children. BMJ 1993;1171-76
8. Fine PEM, Chen RT. Confounding in studies of adverse reactions to vaccine. AmJ Epid 1992;136: 12 1-135
9. GaIeJL, Thapa PB, BoboJR, Wassilak SGF, Mendelman PM, Foy HM. Acute neurological illness and DPT: report of a case control study in Washington and Oregon. In: Manclark CR, ed. Sixth International Symposium on pertusais, abstracts. Bethesda, Maryland: Dept of Health and Human Services, 1990:228-9 (DHSS publication No (FDA) 90-1162)
10. Howson CP,Howe CJ, Fineberg HV, eds Adverse effects of pertussis and rubella vaccines. Division of Health Promotion and Disease Prevention, Institute of Medicine, Washington, DC: National Academy Press, 1991;65-124
11. Bedford H, Elliman D. Childhood Immunisation a review for parents and carets. Health Education Authority 1998, London
12. Odent MR. Culpin EE, Kiinel T. Pertussis vaccination and asthma: is there a link’ JAMA 1994;272:592-3
13. Verrall M, Pertussis vaccine linked to atopy. Pulse 1/5/99
14. HendersonJ, North K, Griffiths M, Harvey T, GoldingJ et *1. Pertussis vaccination and wheezing illnesses in young children: a prospective cohort study. BMJ 1999;318:1173-6
15. StorsaeterJ, Olin P, Renemar B, Lagergard T, ~Norberg R. Romanus V, Tim M Mortality and morbidity from invasive bacterial infections during a clinical trial of acellular pertussis vaccine in Sweden. Paed InfDisJ. 1988;7(99):637-45
16. Sheifele DW, Halperin SA, Pleas R, Delage G, Jadavji T, Vaudry W, cc al Marked reduction in febrile seizures and hypotonic- hyporesponsive episodes with acellular pertussis vaccines: resuLts of Canada-wide surveillance 1993-8 (abstract).Clin In~ect Dii 1999~29:966
17. Miller E. Overview of recent clinical trials of acellular pertussis vaccines. Biologicals 1999;27:79-86
18. Harrison’s Principles of Internal Medicine Ed Braunwald et al. 11th Ed McGraw Hill 1987, USA 19. Gangarosa EJ, Galazka AM, Wolfe CR, Phillips LM, Gangarosa RE, Miller E, Chen RT, Impact of anti-vaccine movements on pertussis control: the untold story. The Lancet 1998; Jan31:356-61
20. Minerva, BMJ 1996;312:1620
21. Van Buynder PG, Owen D, VurdienJE, Andrews NJ, Matthews RC, Miller E. Bordatella pertussis surveillance in England and Wales 1995-7. Epidemiol Inf 1999;123:403-11
22. Source of information for graphs:
Deaths/population 1867-1900. Registrar General’s Annual Returns, 1901-1994 Twentieth Century Mortality CD Rom office for National Statistics. Pertussis notification/vaccine coverage races 1940-1998, Communicable Diseases Surveillance Centre, London NW9