[back]
THE CONCEPT OF GAMMA-GLUCOSE
I believe the reader will benefit by a discussion of the concept of gamma-glucose. Ordinary glucose is a mixture of two chemical forms called alpha-glucose and beta-glucose. Alpha-beta-glucose mixture is derived from the cane sugar we eat, and from the sugar present in fruit; and it is an end product of the digestion of starch. Gamma-glucose is so labile (unstable) that it has never been isolated in the test tube and identified as such. The evidence for its existence however, while indirect, is strong. Many authorities in chemistry and physiology believe it exists since it helps explain certain phenomena which otherwise would be obscure. (Just as in nuclear physics where faith in the existence of protons, electrons, and mesons, helps to explain many phenomena.)
Gamma-glucose is considered to be labile, highly reactive, and readily oxidized. It is very likely that the cells of the body prefer to oxidize gamma-glucose to the exclusion of alpha-beta-glucose. Dr. Shaffer, an authority on the subject, in a review of the literature on gamma-glucose, has stated that the hypothesis appears attractive that alpha-beta-glucose is converted under the influence of insulin into gamma-glucose. In this discussion, and in the present state of our knowledge, it is sufficient to believe that alpha-beta-glucose is synthesized to glycogen in the liver under the influence of insulin and that the glycogen is subsequently broken down into gamma-glucose which is then liberated into the blood.
When a human lives on meat and fish exclusively, as does the Eskimo or Arctic explorer, he is living on protein and fat. Yet glycogen is stored in the liver in normal amounts and there is a constant normal blood sugar level. Where do the glycogen and glucose come from on such a diet? They are derived from protein and fat. Fifty-eight
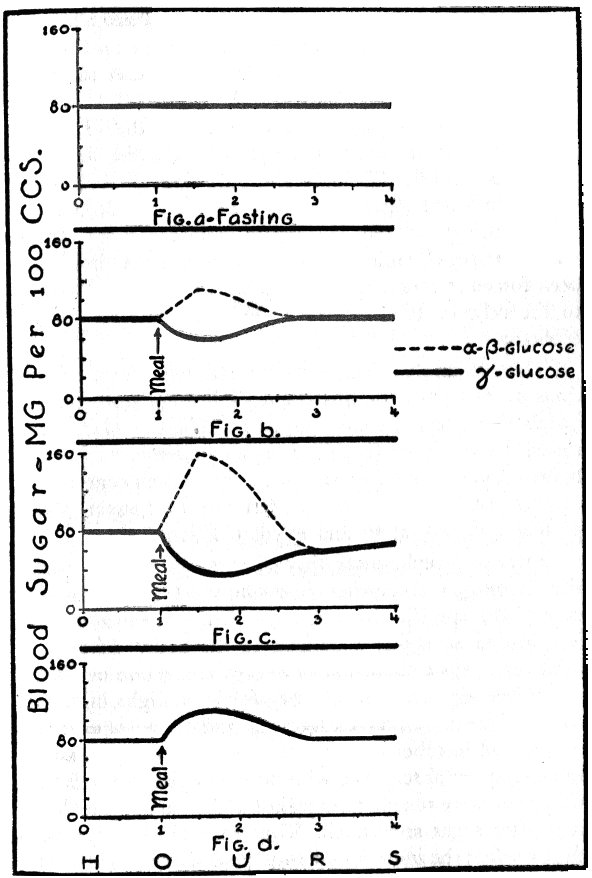
FIG. 14
Fig. a. In the fasting state the blood glucose (or blood sugar) is derived from the breakdown of liver glycogen and may be said to exist in the endogenous gamma-glucose form.Fig. b. Following the ingestion of a moderate amount of exogenous alpha-beta-glucose the blood sugar level will rise, and the blood glucose value will now be the sum of the gamma-glucose plus the alpha-beta-glucose. However, the exogenous alpha-beta-glucose inhibits the output of endogenous gammaglucose from the liver; and the concentration of the gamma-glucose will fall as shown by the heavy line in the figure. Thus there may be a fall in total body oxygen absorption because of the fall in gamma-glucose concentration and in spite of the rise in blood glucose level.
Fig. c. Following the ingestion of a larger amount of exogenous alpha-beta-glucose the blood glucose level rises to a high value and the liver output of endogenous gamm2.glucose is proportionately depressed. Under such circumstances an individual may experience hypoglycemic symptoms even though the blood sugar actually rises. The gammi-glucose output may be subnormal for 1 to 3 hours. After such a meal there may be a fall in total body oxygen absorption.
Fig. d. Following the ingestion of proteins and fat the blood glucose level rises moderately. Since no sugar or starch is ingested no exogenous alpha-beta-glucose is available to inhibit the output of endogenou.s gamma-glucose from the liver. The blood sugar will thus consist of the gamma-glucose form exclusively. The rise in blood sugar after protein and fat is due to the rapid conversion of the digested protein and fat to gamma-glucose. A meal consisting of protein, fat, and carbohydrate foods containing no sugar or starch will also cause a moderate rise in blood sugar and with no inhibition of liver output of gamma-glucose. After such a meal there will be a rise in total body oxygen absorption.
percent of protein and 10% of fat can be converted by the body to glycogen and ultimately to glucose. I want to point out that the blood sugar on such a diet may be said to exist exclusively in the gamma form. On such a diet the blood sugar is produced entirely within the body and so may be called endogenous glucose as opposed to the exogenous alpha-beta-glucose which is introduced from the outside in the foods we eat. Certainly it would appear plausible to regard the sugar derived from meat and fish (protein and fat) as being different chemically from the sugar derived from cane sugar, fruits, and starch. From my studies I have been forced to conclude that alpha-beta-g1ucose is so foreign to the cells of the body as to be harmful to the body’s economy.
There is ample evidence for this statement from observations made by two of this country’s leading researchers in metabolism, Benedict and Carpenter. These workers determined the minimum (basal) oxygen requirements of normal human subjects and then measured the oxygen consumption of these subjects after various test meals of sugar, starch, protein, and fats, alone and in combination.
After a protein meal they always observed a marked rise in oxygen absorption (consumption), a phenomenon called "the specific dynamic action" of protein and which is regarded as highly beneficial to the body. After a fat meal there was a slight rise in oxygen absorption or none at all. After sugar and starch they found a slight initial rise followed by a fall in oxygen absorption in some experiments, and in other experiments they observed a consistent fall in oxygen absorption, with no initial rise. Benedict and Carpenter were unable to explain this fall in oxygen absorption after sugar and starch. They were much surprised to discover that the ingestion of sugar and starch actually could cause a depression of total bodily oxygen absorption below basal requirements.
Here are some of the actual experimental results reported by Benedict and Carpenter. They fed one subject 400 grams of bananas (413 calories) and observed an increase in oxygen absorption of 5.5 grams during the first hour, and a fall in oxygen absorption below basal requirement during the second, third, and fourth hours. Bananas contain chiefly sugar and starch. In the same subject, after 217 grams of beefsteak, (451 calories) which consists of protein and fat, there was an increase in oxygen absorption during each of four hours, with a total increase of 17.5 grams of oxygen against a net increase of only 1.5 grams of oxygen after the bananas.
With larger meals the results were even more striking. For example, after 1382 calories of a sugar mixture, there was a fall in oxygen absorption of 11 grams over an eight hour period with no initial increase; in other words the subject would have consumed 11 grams more oxygen if he had fasted for the eight hours. On the other hand, after 1305 calories of beefsteak there was an increase in oxygen absorption of 40 grams during an eight-hour period.
Now, how does the ingestion of sugar and starch depress oxygen absorption? There are two ways by which this can be brought about: first, by causing low blood sugar, and second, by depressing the liver output of gamma-glucose. As has, been previously explained, sugar and starch may cause low blood sugar about an hour after eating, and this period of low blood sugar may last from one to three hours. During the period of low blood sugar there will be a reduced delivery of glucose to all the cells of the body with a resultant reduced oxidation of glucose; as a result, less oxygen will be absorbed by the body since cells utilize oxygen in proportion as they utilize glucose. Also, during the period of reduced glucose-oxygen consumption, less heat will be generated and so the body temperature may fall. This reduced heat production during low blood sugar readily explains the presence of subnormal body temperature in certain individuals in the morning before breakfast, and even after meals. Such individuals tolerate cold weather very poorly.
The second mechanism whereby sugar and starch may cause a depressed oxygen consumption involves the concept of gamma-glucose. During fasting, the blood sugar is derived entirely from the breakdown of liver glycogen and may be regarded as existing in the readily oxidizable gamma form. Now Dr. Soskin and his co-workers have found that when ordinary alpha-beta-glucose is injected into the blood the greater the amount of alpha-beta-glucose injected the greater the depressant effect on the liver output This reduced output by the liver occurs because there is no apparent need for the liver to pour out endogenous glucose as long as exogenous alpha-beta-glucose is being introduced from the outside. The injection of exogenous glucose raises the blood sugar level and, to prevent too great a rise, the liver responds by lowering its output. The oxygen absorption of the body may fall, however, in spite of the rise in blood sugar level which followed the injection of glucose, because of the reduced output from the liver of the more readily oxidizable form which I believe to be the gamma form.
The influx of alpha-beta-glucose into the blood drives the gamma-glucose out of the circulation, just as bad money drives good money out of circulation. The oxygen absorption of the body falls in proportion as the output of gamma-glucose falls. This concept will explain why Benedict and Carpenter observed a moderate fall after small sugar meals and a greater fall after larger sugar meals. After a pure protein and fat meal (beefsteak) there is no introduction of alpha-beta-glucose and hence there will be no depressant effect on the liver output of gamma-glucose and there will be no fall in oxygen absorption. The marked increase in oxygen absorption after beefsteak may be readily explained by the oxidation of the products of digestion resulting from the digestion of the protein and fat.
Summarizing, the ingestion of sugar and starch may depress oxygen absorption by causing low blood sugar and/or depressing the output of gamma-glucose from the liver. In some instances only one of these mechanisms may be operating, and in other instances both mechanisms may be operating. In the latter, the fall in oxygen absorption will be greater than in the former, and the fall in oxygen absorption may be so great and so prolonged that susceptibility to infection will occur.
I wish to impress the reader with this concept of gamma-glucose. Gamma-glucose is to be regarded as the "natural sugar," preferred by the cells of the body for energy purposes because it is more readily oxidized with greater release of energy. Alpha-beta-glucose is to be regarded as a "foreign sugar," and, in a sense, artificial. Alpha-beta-glucose may be oxidized directly but not as efficiently or as rapidly as gamma-glucose. The reader should remember that the ingestion of sugar and starch with resultant liberation of alpha-beta-glucose after digestion exerts a depressant effect on the liver output of the preferred gamma-glucose.
Knowledge in medicine and physiology is in a constant state of flux. New discoveries open new doors and confirm or alter previous concepts. In the light of our present knowledge, the concept of gamma-glucose presented here is fundamentally sound and warranted by supporting data, and it explains certain phenomena that would otherwise be baffling. Regardless of whether or not the above explanation is the correct one, the fact remains that the ingestion of sugar and starch may readily cause a fall in total bodily oxygen absorption through adverse effects on the blood sugar regulatory mechanism, and it is this state of oxygen lick that is responsible for susceptibility to infection.