So for every one person who got tetanus, 99,999 people without a vaccine didn’t get tetanus, and most of them would never get tetanus.
June 2010 . This is a work in progress. http://www.beyondconformity.co.nz/resources/tetanus
The disease: What is tetanus.
WHO DOES TETANUS PRIMARILY AFFECT?
Are splinters the
only things which cause tetanus?
COMPLICATIONS of tetanus.
The statement that the disease (or exposure to tetanus spores) does not confer
immunity is a nonsense.
Tetanus vaccine.
Vaccine reactions.
Options regarding tetanus
vaccines.
Can, and do vaccinated
people get tetanus?
In 1920, the main street of the town I live in, was compacted mud. Horses were still ridden on it, and tied up in front of stores. The farming around here was still primarily "pick and axe". Life has changed hugely since 1920. Farming is mechanised; fencing is mechanised; footwear and gloves vastly improved; tractors exist; streets are sealed; public sewage common and running water something that people in 1920 could only hope for. Even so, if you did a serological survey in the community, whether vaccinated or not, you would still find higher levels of antibodies in the rural community than in cities. Even within cities it will vary and those who love gardening will have higher levels of antibodies than those who don't. This is totally independant of vaccination, because natural immunity does exist, and vaccinated people get their natural boosters from the environment. The medical profession may greet this information with incredulity, but if they had on their shelves, the medical information I have on mine, there would be nothing they could say in rebuttal to what I have to say.
So first question. Can the vaccine save your life? Yes. Is that a guarantee? No.
So the following information is information which ALL people should know, since tetanus vaccination does NOT guarantee that you will NOT get tetanus. While the medical profession likes to take the credit for ALL the decline of tetanus courtesy of a vaccine, this is simply NOT true.
The proof of that lies with neonatal tetanus in the developed world, which DISAPPEARED well before the existence of either anti-toxin or a vaccine, courtesy of the endless work of people like Florence Nightingale (who, by the way, was 90 when she died...) and the ignored greats, Drs Ignaz Semmelweiss and Oliver Wendell Holmes who both excoriated their colleagues for refusing to wash their hands, and unsanitary medical practice and facilities. Both of them, at the end of their careers, had seen no progress on this issue. Dr Semmelweiss committed suicide, and Dr Holmes was so pissed off, he went and wrote very average novels and poetry, but made it plain in his last paper, that he was doing so, because he was disgusted with his colleagues, who he accused of being systemic murderers, and that he was leaving medicine for the sake of his own sanity.
Real progress often only happens after people ahead of their time die. Then everyone says, "Oh yes, that's blindingly obvious.' Everything we have to be thankful for historically, in terms of zero puerperal fever, neonatal tetanus; safe childbirth and safe surgery can be laid at the feet of people who were treated by medical colleagues like criminals during the time in which they tried to change their colleagues medical practice.
I know how they felt. Anyone who thinks differently to "the system" will be treated as a criminal. The choice to vaccinate is yours, but whether you do or not, you should read all of the tome below, because while it may be long, it's all important.
Of all the diseases for which there are vaccines,
tetanus is the one which frightens most people, and for
good reason. While most of us feel we can cope with chickenpox, measles, mumps
and whooping cough, tetanus is the one disease which IF we get it, can be much
more “uncontrollable”. So if you are going to chose not to vaccinate, there are
certain things you must know.
This resource will be as a series of questions in this order:
a) The disease.
b) Standard Hospital treatment.
c) Treatments ignored by hospitals..
d) Information on the tetanus vaccine.
e) What you must know if you don’t vaccinate.
That depends on what sort of tetanus you are talking about.
There are five kinds of tetanus.
All can be preceded by nonspecific premonitory symptoms such as restlessness, irritability and headache.
1) Subacute tetanus which is characterised by some degree of neck stiffness involving the muscles at the back of the neck; spasticity, as well as increased muscle stretch reflexes, especially in the lower limbs. Patients usually have brief nocturnal generalised spasms There is ankle clonus, but the plantar response is always flexor. The term “mild tetanus” is inappropriate because the presence of generalised muscle spasms is generally felt to imply at least “moderate tetanus” which is not the case in subacute tetanus.
2) Local tetanus (rare) where the contractions of the muscles are only in the area of the injury. These contractions can persist for weeks when treated by the traditional hospital method.
3) Cephalic tetanus (very rare) which can often occur after otitis media with a burst ear drum. Clostridium tetani can be found from swabs taken from the middle ear, but sometimes the entry point can be from the cone put in the ear by the doctor to have a look, or from fingers transferring tetanus spores into the ear. The main symptoms for this form of tetanus are in the head and face area.
4) Generalised tetanus (most common sort about 80%) The symptoms start at the head and work down. Reflex spasms normally occur within 24 – 72 hours, known as the “onset time”. First the person will find it hard to open their mouth; will have a stiff neck and have difficulty swallowing.
Symptoms vary hugely. Sometimes, the tetanus is very mild, sometimes moderat and sometimes serious. the intensity of spasms and sequance of muscle involvement is quite variable and individual.
Then there will be spasms, as the muscles react to the toxin, the stomach muscles will go tight. The temperature will rise in response to the toxin; there will be sweating, raised heart-rate and the blood pressure will rise. Characteristically, the manifestation of tetanus increase in severity for about 3 days after the first sign, and then remain stable for the next 5 – 7 days. After about 10 days, spasms begin to occur less frequently and by the end of 2 weeks, they disappear altogether. Residual stiffness may persist but most people recover completely in 4 weeks. Occasionally, spasms can continue for 3 – 4 weeks under normal hospital treatment, with complete recovery taking months in really serious cases. Emotional, visual and aural stimulation can cause muscle spasms.
5) Neonatal tetanus is primarily in undeveloped countries; very severe, and usually occurs within 10 days of birth. Early signs include difficulty in sucking, irritability and excessive crying, associated with peculiar grimacing. There is intense rigidity, flexion of the arms, clenched fists, extension of the legs and plantar flexion of the toes. Spasms occur eith minimal stimuli. The primary cause in underdeveloped countries is mothers putting camel or other dung on the umbilical cord and neonatal tetanus is a specific problem relating to disgusting unhygiene practices surrounding bad indigenous midwifery practices. Neonatal tetanus used to occur in westernised countries, but was eliminated before either anti-toxin or vaccines, solely through obstetricians and midwives cleaning up their act.
All the effects of tetanus toxin are self-limited and completely reversible in patients who recover from the disease., usually leaving no residual effects.
The symptoms of tetanus spasms, seizures, back arching and locking of the jaw are cause by a toxin called tetanospasmin, released by a bacteria called Clostridium Tetani of which there are many distinct types. All have one or more common antigens, and produce at least two toxins. Tetanospasmin which is the exotin which acts on the nerves, is as toxic as strychnine and is identical across all different clostridial types.
Tetanus spores are everywhere in the environment. On your bookcase, in your back yard, in clothing and house dust. Tetanus has been known to follow surgery and innocuous procedures such as skin testing or intramuscular injections of medications; injecting drug addicts, and I also have many case histories of cases following haemorrhoid and other surgery.
Clostridium bacteria are especially common in the intestines and faeces of
rats, guinea pigs, chickens, cats, dogs, sheep, cattle and horses. Approximately
5% of humans have clostridium tetani multiplying in their guts yet don’t even
know it.
Clinical tetanus, for some unknown reason, has a male/female ration 2.5/1. Toxin
production is favoured by dead or necrotic tissue with little oxygen.
There are no laboratory tests for tetanus, which is diagnosed solely on
symptoms. However, other tests may be used to rule out strychnine poisoning
which looks very like tetanus.
Other diagnoses which have to be ruled out are: dental infections, local
infections, Hysteria, neoplasm, encephalitis and dystonia. (Hegazi – last slide)
Dystonia can also be caused by drugs like stemetil, Stelazine and chlorpromazine
(Largactil) so in cases where tetanus is considered, “pseudotetanus” as a result
of drug ingestion should be ruled out first.
http://www3.interscience.wiley.com/journal/119596281/articletext?DOI=10.1111%2Fj.1365-2044.1979.tb08539.x
Benztropine of Diazapam are the antidotes recommended for tetanic like symptoms
from drugs. (Which makes you ask the question, what is the influence on the
nerves from these drugs which can cause such reactions?)
In the medical literature is the constantly repeated phrase throughout history, particularly before paved streets, running water and flush toilets..., that tetanus primarily affects the very young, the old and the immunocompromised - however they understood that concept in those days. Generally though, the "weaker" would have been protected from tetanus, since they didn't have the energy of ability to do work which would constantly expose them to tetanus spored.
The "rusty nail" originated when horses were always on the road, and barefoot people stood on horseshoe nails, often embedded in mud impregnated with horse dung. Today, we know that tetanus spores are everywhere. Puncture wounds which do not bleed are the most dangerous, and "rusty nails" aren't the only things which can carry tetanus spores into someone's body. In children, feet will be the most likely portal of entry, because they are more likely to run barefoot, but the portal of entry for older children, or adults is far more likely to be hands, knees, elbows - and if medical literature is taken not of - burst middle ear drums and... surgery!
Spores are ubiquitous. They can be found on any surface in hospital, on your bookcase, in your spit. Human bites and bullet wounds are potential portals of entry. The fact that the world was well habituated before a tetanus vaccine shows us that natural immunity existed and continues to exist in the face of commonsense cleanliness.
Today, in undeveloped countries, the primary risk groups is babies whose parents or the local midwives put camel or other dung as a traditional ritual on the umbilical cord, and older people with cuts which haven't been cleaned out properly.
When Captain Cook came here, there weren't a whole lot of Maori dead from tetanus. More maori will have died from their constant inter-tribal utu and wars than would ever have died from tetanus.
When Europeans came here, everything had to be done by hand, and even then people weren't dying from tetanus hand over foot. (bad pun) and you know that. How? Well, most of you have a family tree. How many in YOUR family tree died of tetanus?
Yes tetanus happened and can happen today... and that's why this is written.
You need to know a whole lot of information. Even more than is put here, so that you can make choices, and whatever those choices are, know what you are going to do, and why.
No. Tetanus has been noted after skin abscesses, gangrene, burns, frostbite, middle ear infections, surgery, abortions, childbirth and drug abuse, primarily "skin popping". Sometimes, no "portal of entry" can be figured out. In terms of puncture injuries, sometimes the smaller ones are the more dangerous because people don't tend to clean them out.
Complications contribute significantly to deaths in tetanus. The death rate varies from country to country and hospital to hospital, and to a degree, depends on the immune system of the person with tetanus. In underdeveloped countries with minimal medical assistance the death rate is far higher than in western countries.
In developed countries, death usually results from a secondary bacterial complication introduced by intubation, tracheotomy, or a nosocomial (hospital acquired) infection. Some other complications result from overly vigorous therapy and prolonged bed rest, while others can be attributed to the tetanus toxin itself, and failure to neutralise it adequately. According to one medical text, high fever later in tetanus, usually signifies secondary infection. Pneumonia is the most common late complication and is found in up to 70% of autopsied cases. (which I believe is scurvy induced because of high levels of toxins, and because hospitals don’t use vitamin C in the treatment of tetanus.)
The death rate from tetanus in developed countries is entirely dependant upon
the quality of medical care, treatment and nutrition given during tetanus
infection. Secondary bacterial infections may become more of an issue, as
continued overuse of antibiotics by the medical system drives the development of
more and more superbugs.
The most current e-medical article on four of these sorts of tetanus, and the
treatment can
be read here: with another emedicine site being for
paediatric tetanus here:
The standard treatment options are covered in the emedicine article above. A powerpoint on clinical features can be seen here. (Hegazi)
In New Zealand, feedback over the years has shown that New Zealand hospital
treatment depends on the symptoms, but usually involves the antibiotic
metronidazole (which is primarily used against anaerobic bacteria and
Giardia) and tetanus
immunoglobulin. Penicillin is not an antibiotic of choice, because it
causes more spasms, and tetracycline should never be used, because it strips the
body of vitamin C which is crucial in any toxin mediated disease.
Antibiotics make no difference to the course of tetanus disease –
but they use them anyway. In turn, antibiotics trash the gut flora, which
may make the patient more susceptible to hospital acquired bacteria such as
clostridium difficile and cMRSA or superbugs. They also trash good gut flora
affecting the ability of the body to absorb minerals and vitamin K, B etc. The
detrimental results of heavy duty antibiotic damage on gut flora
can be permanent.
Here is the
proper version of the study. On this basis, you wonder why they continue to
use an antibiotic that has no effect on the course of the disease.
Depending on the spasms, sedation may be midazolam and morphine, as well as a paralysing agent for spasms. Morphine however, can make some people vomit which is not a good idea, so should be carefully monitored. The room might be darkened and stimulation discouraged. If a temperature is present, the ubiquitous paracetamol will be used.
For some stupid reason, staff continue to want to bed-bath patients daily. This is totally unnecesary, and leads to spasms. The only things that need good cleaning are the nurses hands etc; luer areas; equipment used in and on the person and the skin in those areas. Physical stimulation should be kept to a minimum. So while hospitals do this (wash) they shouldn't IMO.
NZ hospitals regularly turn to avoid bed sores. This is crucial.
New Zealand hospitals also push vaccination, on the basis that they
say the disease does not confer immunity, and therefore the person
needs vaccines “immunity” by the time immunoglobulin wears off. Furthermore,
hospitals and doctors push the use of vaccine which contain other disease
antigens as well.
The New Zealand Health Department stopped bringing in single tetanus antigens in March 2007.
Hospital offer/push adults to have the Quadracel (diphtheria, tetanus pertussis and polio), and for children hospitals insist on Infanrix-Hexa, which has diphtheria, tetanus pertussis, polio, hepatitis B and Haemophilus.
As we stated in our second book in 2008, we view this attitude of the system
to be major impediment to anyone wanting to vaccinate against tetanus - before
or after tetanus ( not during ). In our opinion, the dropping of the single
tetanus antigen, and the of Quadracel or Infanrix-hexa is "wide net casting" to
“trap” people into having all vaccines. In our view, any vaccine administered
to anyone with tetanus is a totally unnecessary assault on the immune system on
a body which already has more than enough to do.
For anyone chosing to vaccinate against tetanus at any time, single tetanus
antigens, or paediatric DT can still be found in this country, but requires
going under the radar to find medical practices who privately import vaccine
stock from Europe.
Furthermore, there is no medical clinical rationale to vaccinate while
undergoing heavy duty treatment to survive tetanus. Neither are there any trials
to see whether it affects the disease outcome. The body has better things to do
than derail
the immune system resulting in a T4/T8 ratio to produce an immunological
profile which looks like that of someone with AIDS, It has since been
discovered that the influenza vaccine also results in a prolonged aberrant
immune profile as well. To vaccinate someone while their body is fighting a
serious disease lacks common sense.
Some references on this are: http://www.ncbi.nlm.nih.gov/pubmed/6680401
... http://www.ncbi.nlm.nih.gov/pubmed/1092755
“ The existence of natural immunization was unquestionably demonstrated by
presence of protective levels of tetanus antitoxin in the blood of the majority
of 59 surveyed subjects considering that none of them had ever received any
tetanus toxoid and most of them never received a single shot of any drug.” http://www.ncbi.nlm.nih.gov/pubmed/2651348
... http://www.ncbi.nlm.nih.gov/pubmed/6114281;,,,, http://www.jstor.org/stable/30115079
.
WHO recognizes these studies, but dismisses them, and it’s easy to see why.
The absolute key to tetanus management
is careful around the clock attention to mucus build-up in the lungs, use of
magnesium to stabilise the heart and blood pressure and simply nursing;
keeping the patient well hydrated,
paying attention to electrolyte balance, sedation, reduction of sensory
overload, and excellent nutrition. Patients with tetanus require about two and a
half times MORE calories than normal daily life, due to the metabolic
requirements on the body of fighting tetanus. Any nerve dysfunction and
breathing irregularities need to be carefully managed. Just relying on tetanus
immunoglobulin and sedation gets you nowhere fast.
Unfortunately, hospitals in this
country are noted for their abysmal lack of understanding about nutrition.
1) New Zealand hospitals do not generally use magnesium even though it’s a
standard medical treatment. If you want magnesium treatment you will have to
push for it.
Magnesium should be a first
line treatment for tetanus . Magnesium stabilises the heart and reduces
blood pressure; reduces the need for sedation, and also makes nursing simpler.
The medical evidence for Magnesium is sound, with the most recent 2010 article
on magnesium in adults is
found here:
and a 1997 medical article on magnesium in tetanus,
can be found here:
. A more recent 2004 article by Attygalle
can be found here. A 2003
article by Cevilla on the use of magnesium in children can be found here.
Other articles can also be found on
pubmed.
Magnesium was extensively used between 1900 and 1945, because tetanus
anti-toxin was not developed until 1924, and then had a bad reputation for
killing people, primarily because it was made from horses. But with the advent
of slightly safer anti-toxin, and antibiotics, the medical profession supported
patented pharmaceuticals rather than using safe, established unpatented
solutions. Later, human immunoglobulin replaced the use of dangerous anti-toxin.
2) New Zealand hospitals do not use vitamin C for tetanus. It's a safe bet that
hospitals will reject any suggestion of vitamin C use.
Again, in the early years, vitamin C showed great promise in animal studies.
A
human study in Bangladesh, also pointed to possibilities, but this study
suffers from design problems. Nevertheless, the Cochrane
collaboration considers that it should not be ignored, because the death
rates were so low, despite the fact that the same dose of vitamin C was used in
a baby, compared to a 64 year old, which is a scientific nonsense. Commonsense
would dictate that like antibiotics or anti-spasmodics, vitamin C should be
calibrated for both weight and severity rather than handing out a routine 1 gram
per day, no matter the age, weight or severity. In American in the 1950’s
Dr Frederick Klenner used vitamin C to good effect with all toxin mediated
diseases including tetanus. Other doctors have also used it, but they have
pretty much kept their heads below the parapet so that the system doesn’t shoot
them between the eyes.
Professor Hemila from Finland wrote a thesis on vitamin C, and in his 2006
thesis collected all animal studies that he could find. The majority of them
found that vitamin C protected against diverse viruses, bacteria and bacterial
toxins.
See pages 6-9 and 105-118 in:
https://www.doria.fi/handle/10024/1540?locale=len
Pages 6-9 are also available as HTML version
http://www.ltdk.helsinki.fi/users/hemila/animals/
(some other parts are listed at: http://www.ltdk.helsinki.fi/users/hemila/thesis.htm
) Of particular interest in this case are studies by Dey (and Buller-Souto&Lima
summarized by Clemetson)
3) New Zealand hospitals do not use N-Acetylcysteine (NAC). If paracetamol is
being used to reduce fever, it is potentially liver toxic, and NAC is the
anti-dote. The last thing anyone with tetanus needs is more pressure on the
liver, which will be doing a lot of the detoxication work getting rid of the
exotoxin tetanospasmin. It makes sense to include NAC. The other reason to
consider NAC is that tetanus toxin can thicken mucus, and NAC thins thick mucus.
4) New Zealand hospitals don’t use homeopathics. Obviously! A list for specific
homeopathics for tetanus
is available here: If you want other lists, google it.
CDC handbook on tetanus and vaccine
New Zealand handbook on tetanus
The tetanus vaccine was introduced on the back of World War II experience – (never mind that both the New Zealand soldiers who died from tetanus were vaccinated.... and when I was researching the enquiry into why tetanus happened in soldiers' hospitals, I didn’t know whether to laugh or cry when an old medical article stated that tetanus spores were found impregnated in both the cotton wool and bandages used to wrap up wounds!)
Intitially only the military were vaccinated and up until 1960, children
didn’t get the vaccine. Tetanus vaccination for children became universal in
1961. A different formulation was offered to adults were offered in 1970. If you
have looked at the CDC website in USA, you will notice that graphs for cases or
hospitalizations always start the year that vaccination started. In New Zealand,
the graph in the handbook starts in 1970, which doesn’t tell you very much, or
give you an idea of risk/benefit ratio.
There have never been randomized controlled trials with the tetanus vaccine, for
the simple reason that the medical profession, when it believes in something’s
use, considers randomised trials with unvaccinated controls, unethical.
Only this year, was
the first
study done looking at the responses in adolescents who had been vaccinated as
babies. I have read the whole article, and to say the least, the results are
disturbing. Given that this failure to respond to later boosters, doesn’t happen
when children are vaccinated with a primarcy schedule at a later age, this
should give some people pause for thought, though not to the researchers, ....
whose solution is simply to give more boosters more often!
The old “more must be better” motto.
Please note that no-one actually knows what the protective level of antibodies are in humans. This is assumed from studies of animals, decades ago. Therefore the assumed protective level is a guess.
(Yet to be done).
The list is long, and I have a whole folder full of many different types. I will
add med article URLs later. In the meantime, use pubmed.
Many parents have reported to us, that the tetanus vaccine is one which they might have considered for themselves, or their children were it available as a single vaccination or as a paediatric dT.
They have been told by their doctors, that it is only available as a
combination along with diphtheria, whooping cough polio, hib and hepatitis B,
called
Infanrix-Hexa. Even adults are telling us, if they go to A & E with an
injury, that they are being “offered”, Quadracel
under the guise of a “tetanus” shot which has pertussis, diphtheria tetanus and
the three polio strains. If they are lucky, they are only injected with
Adacel, which is diphtheria, Tetanus, and pertusis, and don’t find out until
afterwards, that it wasn’t just a tetanus vaccine. Those who brave the
inquisition and say no, are required to sign disclaimers.
Contrary to what doctors and hospitals are telling you, there are some practices
who will provide single tetanus vaccinations. They must be imported privately,
and usually, the cost of vaccination and administration is around $70.00. If you
are considering a tetanus vaccination, do not accept the statement, that a
single antigen cannot be done. It is true that medsafe no longer lists a single
vaccination, but that isn’t because a single antigen is no longer available.
That is because it’s now Ministry of Health policy to only “offer” combination
vaccinations to all age groups, which is counterproductive, if that means that
some people who might otherwise have a tetanus shot, refuse a combination shot.
Most people who are vaccinated, don’t get tetanus, but yes it can happen:
In 1978
Berger et al published case reports of tetanus despite preexisting
antitetanus antibodies
In 1982, the BMJ reported tetanus after a bone marrow transplantation in a fully vaccinated member of the military
In 1986,
Passen et al reported a case in a 35 year old who had had the primary series
and two boosters 8 and 4 years prior to tetanus. His antibody levels on
admission were 16 times higher than presumed protective levels. What did the
hospital do when this man survived? They followed up with more vaccines. When
five vaccine plus 16 times more anitbody than necessary don’t work, more surely
will!
1991. Maselle et al reported
Neonatal
tetanus despite protective serum antitoxin concentration. Seven babies with
clinical tetanus were found to have antibody levels 4 – 13 times higher than the
presumed minimum protective level. Some mothers had received multiple booster
during pregnancy with antibody levels 100 – 400 times higher than the presumed
protective level.
In 1992, Crone et al reported
tetanus in
3 immunized people.
1993
Tetanus in vaccinated children. Five of the cases in this article were
children, and four were fully immunised.
In 1994, a case was reported in
a fully vaccinated drug user.
In 1995 De Mores Pinto reported neonatal tetanus despite
vaccination and protective levels of antibodies.
In 1997 generalised tetanus was reported in a man who had had a primary series
and two booster injections, and had tetanus
antibodies
more than 100 times the protective level.
In `1998, O’Malley et al, reported a
woman with serious
tetanus despite being fully vaccinated.
1999, Shimoni et al detailed a
34 year
old construction worker fully vaccinated and boostered.
2000 Vinson presented CDC data showing that of 740 listed cases,
53 cases
had completed a primary series and 22 had received their latest boosters between
5 and 9 year, and two had had boosters within 5 years. (Follow the links to
the pdf in Pubmed)
2000, Abrahamian et all detailed a case in an injecting fully vaccinated drug
user whose
antibody levels were 16 times higher than presumed for protection.
After a 2003-2004 tetanus outbreak in UK amongst injecting
drug users (IDU) where some were vaccinated and two had had five vaccines.
It was recommended that IDU be given immunoglobulin whether vaccinated or not,
since their nutrition and lifestyle will predispose them to tetanus.
Between 2005 – 2007 half
the tetanus cases in UK were IDU’s (slide 28) I note they carefully omit to
mention the ones who were fully vaccinated…. (and don’t you love that female
prisoners should receive the rubella vaccination to prevent them from having
congenitally damaged babies? - huh?)
In 2006, Heydari et al reported tetanus in
a healthy
immunised adult.
In 2007, Beltra et al described a patient with tetanus
despite protective levels of antibodies
And so it goes on.
Many vaccinated cases don’t get reported in the medical literature anyway. I know of two people who had tetanus, who were fully vaccinated, and their cases were never reported in the medical literature as vaccinated. There are a lot more medical articles, but most don’t have abstracts or full texts available, and are in other languages. So this is a universally known about issue.
Last but not least is a doctor's story of how he,
fully vaccinated and boostered, got and survived tetanus. But his story was
never written up in the medical literature. Funny that. This story was written
for me in 2004, and published with permission.
The other interesting issue is that if you look at some of the serological
surveys, particularly those done in USA over the years, quite a large proportion
of well vaccinated people don’t have purported protective levels of
antibody – bearing in mind that these people never acknowledge the
presence of memory immunity for any disease, let alone consider it a possibility
for toxin mediated diseases.
Therefore, no doctor can ever rule out tetanus, even if someone is vaccinated. A
point made by Vinson and Shimoni mentioned previously.
If I don’t vaccinate myself, or my children, I might get tetanus, and die.
You might. But what are the chances of that? 100% if it happens to you.
Yes, tetanus happens. However, being realistic, how many people in your family
tree got or died of tetanus before the vaccine came out for universal use in NZ
from 1960? Prior to that, only military personnel received the vaccine. My
father died at the age of 95, having been brought up barefoot around horses,
never having had a tetanus vaccination in his life, and regularly shovelling
horse manure yearly in the garden. I know many people who have never had a
tetanus shot, and never will. Many of the people in new Zealand today, who are
100 years or older, have not had a tetanus vaccine, and if they did were 60
years old at least, before they had a primary series. How did they survive?
Their immune systems were up to the job, because every single one of us comes in
contact with tetanus from a very early age. If there was not an inate natural
immunity, the world would never have over-populated before the tetanus vaccine
was rolled out to civilians 40 years ago.
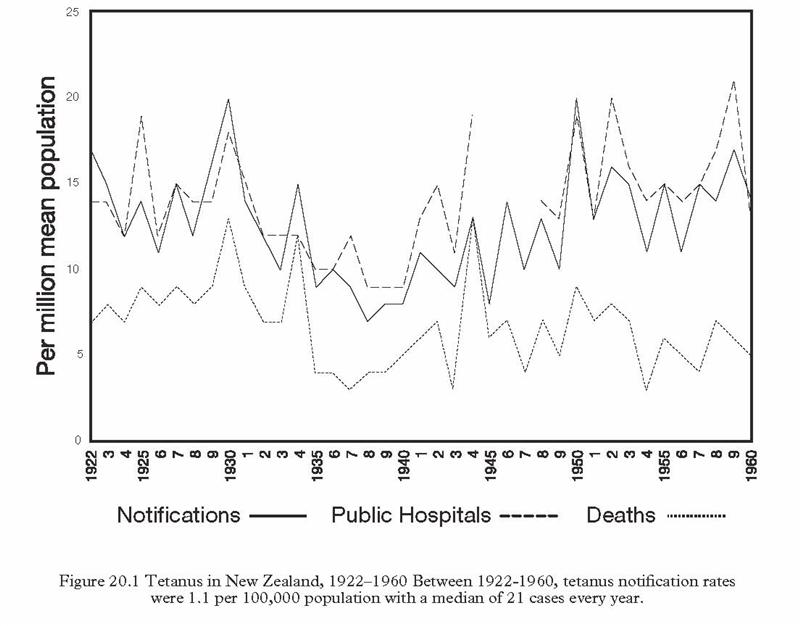
Historically, in the forty years between 1920 and childhood vaccination began in
1960, the incidence of tetanus was 1.1 cases per 100,000 per year.
So for every one person who got tetanus, 99,999 people without a vaccine didn’t
get tetanus, and most of them would never get tetanus.
Yes, that means that without vaccination, that in a country of 4 million people, you could have forty four cases a year in people, most of whom were never taught proper wound management, if we still lived in a country in which far more people still rode horses to school, played barefoot in the horse paddock next to the school, and we had a medical profession which didn’t understand how to clean out wounds.
On that note I've watched doctors NOT clean out wounds on the assumption that the person is vaccinated, forgetting that there is far more than just clostridium tetani in soil....
Please note that that huge dip in the graph above, which also appears in data from other countries, occured during the times when polio prevention included huge posters which had phrases like, "Sneezes spread diseases" ... "Wash your hands after X Y and Z" ... "Flies are deadly germ spreaders". There is a huge range of posters which emphasised cleanliness, food safety, good hygiene, and "Berty-germ". It's no coincidence to me that the minute that focus vanished, tetanus rates climbed yet again.
Serious reactions to tetanus vaccines, such as brachial neuritis, occur at the same rate as clinical tetanus ... at a rate of 1 per 100,000, so again, that's part of the risk/benefit equation which has to be weighed up, but normally people can't weigh it up, becuase people don't get told what the odds are in getting tetanus, or a reaction. I have a huge stack of letters from people with serious reactions to the tetanus vaccine which have permanently blighted their lives. Both sides of the coin, have potential consequences. Both vaccine reactions, and clinical tetanus are rare. But if you get either tetanus or a reaction, data means nothing. Reality is 100%.
The fact that serious reactions, like brachial neuritis, has the same strike
rate for complications, as for getting tetanus itself, also makes you wonder if
there is a genetic susceptibility component with regard to both getting tetanus,
and having a vaccine reaction. This has been postulated so in other infections
when looking at people who don't respond to Hepatitis B or Hib vaccines.
They appear to have the same gene pattern as those who get serious Hib or become
Hep B carriers. (See medical articles by Gregory Poland)
Remember, the choice to vaccinate or not, is yours. The responsibility to do all
you can in every facet of your life, is also yours.
No they were not.
But these are basic life-long fundamentals which prepare a person to heal well throughout life, regardless of the vaccination status, and quite irrelevant to any issues relating to tetanus, because many infections can result from any puncture wounds, shell cuts, coral punctures and skin injury.... not just tetanus.
So this information applies to all
skin puncture wounds, in all people, vaccinated or not.
1) A healthy diet with no junk food, no artificial sugar,
refined flour, alcohol, drugs or smoking anything. At any time of life. Pregnant
women even more so, to “build” a healthy baby.
2) Prolonged breastfeeding of babies to build a strong inate immune system. Most people consider breastmilk to be just food, but it is not. It's the orchestrator of immune development, as well as a sentinel within the body with the potential to destroy cancer cells and protect a person from many chronic diseases until they die. Seriously.
3) Nutrition, nutrition and nutrition. Fruit, veges, protein, whole grains…. Everyone should drink water, preferable safely collected and enclosed rain water, not chlorine, aluminium, fluoride and floculant permeated municipal supply ghastly tasting stuff.
4) Rule number one: Do not go anywhere, where there is possibly broken glass, metal splinters, wood splinters etc, with bare feet.
That includes pavements, unsafe beaches, playgrounds, widely patronized bush areas, green areas inter-city. In the bush, watch out for bush lawyer plants and other thorny traps. Beware of roses and any plants with spines. If you have a Phoenix canariensis palm in your garden, or any other dangerous variety palm for that matter, get rid of it . These sorts of palms carry a variety of serious pathogens including, "an array of aerobic and anaerobic pathogenic bacteria including Clostridium perfringens the causative agent of the life-threatening gas gangrene, Bacillus anthracis, and Pantoea agglomerans. Septic inflammation caused by plant thorn injury can result not only from bacteria. Medical literature indicates that thorns, spines or prickles also introduce pathogenic fungi into animals or humans."
Quite apart from falling palm branches hitting you on the head, phoenix and other palms can be exceedingly hazardous for gardeners, or passers by.
The splinters have barbs and can cause a wide array of serious clinical problems like septic arthritis. Dirty phoenix palm barbs would be a prime tetanus spore induction as a splinter, because they are just about impossible to remove properly without cutting everything wide open. If you get a phoenix palm splinter, you need to open it right out, which is painful, and make sure every barb and fragment is removed. If you are anywhere where there are palms or cactus, don’t touch them, and do not “wear” bare feet.
Small palm “fruit” is toxic with high levels of oxalic acid as well, and can cause dermatitis if walked on, and worse. If you live in countries with poisonous snakes, scorpions and spiders, be aware that palms are their favourite haunts, as well as for rats, mice and other rodents. In short, know your plants, poisonous animals and insects and ... plan ahead.
5) A competent wound care knowledge might not only save your life, but someone else’s as well, and a thorough understanding of progression of symptoms of the different sorts of tetanus, methods of treatment, is crucial.
6) Any cut, splinter, grazed chin from falling off bikes, or toe, knee or elbow grazes from concrete etc, must be cleaned out immediately. We always carry snap open saline solution, tweezers and splinter removers etc… when we travel, and even when we rode bikes.
If you are in hot countries, where hygiene practices are woeful, all grazes should be washed out with saline solution, sprayed with a hydrogen peroxide mix (take it with you), and if necessary, follow up with iodine and witch-hazel. BE PREPARED. BE EDUCATED.
7) Children at school should be taught why and how to treat their own grazes, because New Zealand school staff often have no idea, because they assume that all children are vaccinated, and have little understanding that cuts can cause serious infections quite apart from tetanus. If your child doesn't want to do this, get the child to ring you, and if possible, go to the school and do it yourself in the car!
A similar problem exists with doctors and hospitals. We’ve experienced it ourselves, where doctors haven’t cleaned out something on the basis that the person is vaccinated. Yet they forget that “soil” contains a whole lot else other than tetanus spores.
8) In our household all cuts are cleaned thoroughly, and washed out with a hydrogen peroxide mix. (If you want the specific recipe, email me).
Any barnacle or mini-mussel cuts from beach rocks must be treated immediately, if the person so cut, was silly enough to rock climb with bare feet! Open cuts are “dressed” when outside.
For outside work, I wear the cheap beachfeet from the Warehouse, even when gardening. These allow me to walk and run with a natural foot action, and I don’t have to worry about bee stings either. I also use these at the beach for traversing rocks to prevent cuts.
9) The most dangerous tetanus prone splinters are fish bones, fishing flies, nails in the ground, palm splinters, rose thorns, but tetanus can be got without a puncture wound.
Never bury fish bones in the garden to break down as manure. Put them in a “lockable” barrel with water where they will dissolve over time, and become a liquid compost mix.
If you have children, and are planning a garden, do not plant roses, agaves or palms and only plant thornless fruit and berry plants. Children don’t understand the word “no” in a garden. By the same token, once they are old enough, teach them which plants are dangerous. Knowledge is power.
10) If you don’t have children, and chose to have “nasty” plants, do not deal with roses, boysenberries, thorny citrus or any palms without leather gloves to protect your hands. If you have an immunodeficiency, or are immunosuppressed from medical treatment, wear cotton gloves and surgical gloves when dealing with commercial compost, and wet the compost before transferring it from the bag. (I do all my gardening with cotton and surgical gloves anyway, and have no time for nasty plants.)
11) When cleaning up large quantities of animal manure, wear cotton and long surgical gloves, or use shovels etc, and do not touch. This isn’t just for tetanus protection. It’s just plain common sense. Drum these rules into your family.
12) Even if you wear gloves, hand and feet-washing and keeping nails clean, should be a basic, understood by everyone.
13) If you get a splinter of any sort, after removing and cleaning it out, make sure that you are taking plenty of vitamin C and watch it carefully for signs of infection, pain, and red streaks travelling away from the site.
14) Make it your business to learn every possible method of treatment for
septic cuts, burns and wounds in general, so that you can pre-empt any possible
infection of any sort. Learn the nutrients needed for optimum healing.
Do all this, and you should not have cause to land up at the doctors for any
reason, and if you do, at least you will know you’ve done everything you could
to prevent problems. ( Other than to vaccinate if you so chose.) However
vaccination only provides possible protection against one of the many hazards
which can result from cuts, burns and splinters. And as you have seen, a tetanus
vaccination is not a 100% guarantee that you might not get tetanus. Even if you
vaccinate, learn how to deal with wounds properly, and clean out every splinter
and wound meticulously regardless.